
[box type=”bio”] What to Learn from this Article?[/box]
Hairy Elbow Syndrome, showing the case of a child with the peculiar characteristics of this benign anomaly.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page:32-34 | Vito Pavone, Gianluca Testa, Raffaele Falsaperla, Giuseppe Sessa. DOI: 10.13107/jocr.2250-0685.267
Authors: Vito Pavone[1], Gianluca Testa[1], Raffaele Falsaperla[1], Giuseppe Sessa[1]
[1] Department of Orthopedics, A.O.U.P. Vittorio Emanuele, University of Catania, Catania, Italy.
Address of Correspondence:
Dr Vito Pavone, Department of Orthopedics, A.O.U.P. Vittorio Emanuele, University of Catania, Catania, Italy.
Email: vitopavone@hotmail.com
Abstract
Introduction: The hypertrichosis cubiti also named” hairy elbow syndrome” is a benign anomaly which occurs as an isolated sign but sometime it may be associated with others abnormalities including short stature, facial dysmorphism, developmental delay and bone anomalies.
Case Report: The Authors report on a girl 8 years old, who showed a classical hypertrichosis cubiti, tufts of peluria in the thoraco lumbar region, moderate scoliosis and bilateral large big toes. In correspondence with the tufts of spinal peluria the MRI displayed areas of syringomyelia.
Conclusion: A review of the cases of hypertrichosis cubiti associated to spine and bone anomalies is reported. This is the first report of the association of hypertrichosis cubiti with syringomyelia and large big toes. The presence of peluria in the elbow and/or in the thoraco lumbar region may be a clue of malformations of spine and bone. In conclusion the HC may be a simply aesthetic, benign anomaly, but may be also a clue of malformations affecting many organs including the spine and skeletal tissue.
Keywords: Syringomyelia, hypertrichosis cubiti, Hairy Elbow Syndrome.
Introduction
Hypertrichosis cubiti (HC) is a benign, not androgenic hormone-dependent form of hypertrichosis characteristically localized on the extensor surfaces of the distal third of the upper arm and the proximal third of the forearm involving the entire elbow region bilaterally. The hairs are of lanugo type, fair colored and reach several centimeters in length. The hairs tend to appear in infancy, become coarser during early childhood and usually regress at the young-adult age [1,2]. This condition was first reported by Beighton [3] in two siblings in whom the cutaneous anomaly was associated with growth retardation and it proposed the term of “hairy elbow syndrome”. Since then about 40 cases have been reported [4].
In a wide review of the literature, Polizzi et al [5] reported that the HC in half of cases was present as an isolated cutaneous anomaly, whereas in the remainder half the condition was associated with other abnormalities including short stature, facial dysmorphism, developmental delay, infantile spasms and minor skeletal anomalies [6-9].
We report here a young girl who showed a thoraco- lumbar right convex scoliosis, a bilaterally large big toe with a left nail dysplasia and tufts of peluria localized in the elbow (as a classic hairy elbow syndrome) and in the thoraco lumbar region. In correspondence with the cutaneous thoraco-lumbar hypertrichosis, two areas of syringomyelia at the level of Th1 to Th4 and Th12 to L1 were seen at the spine MRI. A review of cases of HC associated with anomalies affecting the spine and skeletal bones is reported.
Case report
An eight years, ten months old girl was referred to the Orthopedic Clinic of the University of Catania, Italy for the diagnostic work up of her scoliosis. She was the third child of healthy, unrelated Italian parents. At the gestation, the mother was aged 31 and the father 33 years. A sister and a brother aged 4 and 2 years, are healthy and do not show hairy abnormalities at their clinical examination. The mother felt normal fetal movements during gestation and the pregnancy was uneventful. The mother denied having had any infections or having used folic acid, any drugs or alcohol during pregnancy and specifically any topical or systemic drugs which can cause hypertrichosis.
The girl was born at 39 weeks gestation by cesarean section with breech presentation. The birth weight was 2700 g, height 49 cm and head circumference 35 cm. The Apgar scores were 8 and 10 at 1 and 5 minutes, respectively. The mother referred to have noticed in the girl a tuft of hair in the thoraco lumbar region a few days after birth and the hairy at the elbow level at the age of 3-4 years. The scoliosis was noticed at the age of 8 years during a scholastic medical checkup.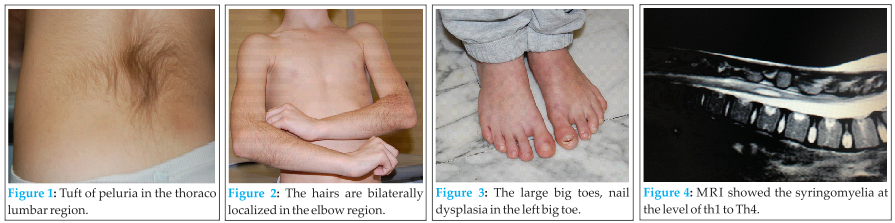
At the physical examination the girl’s general conditions were good, her weight was 24 kg (25rd centile) and height was 138 cm (50rd centile). During the examination for the scoliosis a tuft of hairs was seen in the thoraco lumbar area (Fig. 1). At the same time abnormal hairiness was noticed at the elbow from mid humerus to mid forearm bilaterally (Fig. 2). The hairs were thin, lanuginose and fair colored and reached the length of 12-20 centimeters. A thoraco lumbar right convex scoliosis was present. The big toes were large (Fig. 3) with recurrent drug resistant infections in the left big toe. Scholastic performance was good. Routine blood and urine analysis and full metabolic and endocrinologic screening yielded normal results. Abdominal ultrasound was also normal. Histological studies of hair taken from affected areas yielded no anomalies with most of the hair follicles in the anagen phase. No abnormalities were noticed at the brain-MRI. Spine MRI disclosed a wide dilation of the ependymal channel from Th1 to medullar cone with segmentary syringomyelic cavitation at the level Th1-Th4 and at the Th12-L1 lumbar level with liquoral signal (Fig. 4a-4b). Normal the intersomatic spaces. Feet X-Ray showed large big toes with absence of bone lesions. The karyotype of the patient was normal (46, XX).
Discussion
The girl showed a typical distribution of hairs bilaterally in the area of elbow suggesting the diagnosis of HC (or hairy elbow syndrome): tufts of hypertrichosis were also present in the thoraco lumbar region. Below this hairy anomaly a spine MRI disclosed the presence of areas of syringomyelia clinically correlated with the moderate right convex thoraco lumbar scoliosis. A bilaterally large big toes were also found with nail dysplasia in the left big toe.
Syringomyelia is an uncommon condition with variable prevalence of 1.94/100.000 in Japan and 8.4/100.000 in Western countries [10,11]. The syringomyelia may present within the spinal cord parenchyma as a fluid-fillet, gliosis-lined cavity or as a focal dilatation of the central canal (hydromelia) [12]. Syringomyelia may have a congenital origin or may be acquired and caused by anomaly in cerebro-fluid circulation. The congenital form is distinguished according to the time of involvement in embryonic or fetal, the last acting in the phase of primary neurolation [12]. The anomaly may present silent and asymptomatic and incidentally discovered at the spine MRI; in the most severe cases the clinical symptoms may be represented by pain, neurologic deficit of the extremities, bowel and bladder dysfunction [13,14]. Scoliosis seems to be a prominent feature of the syringomyelia particularly when it is localized in the terminal area.
Treatment of symptomatic syringomyelia is related on the etiological cause and is focalized in restoring normal cerebrospinal fluid flow dynamics [12].
In our patient the syringomyelia was asymptomatic and clinically correlated to a correspondence cutaneous tuft of peluria in the thoraco lumbar region and it was associated to a right convex scoliosis.
Examining the girl, the presence of hypertrichosis in the region of the elbow was seen. The HC has been associated with congenital anomalies. In a review of 28 patients with HC collected in the literature, Polizzi et al. [5] reported in 13 out of 28 patients the presence of short stature which was also observed in one of their three patients. Other associated features were intrauterine growth retardation, facial dysmorphism, and developmental delay. In a more recent review of 31 patients, Koç et al. [6] report the presence of dysmorphic face in 9 patients, psychomotor delay in 6 and limb anomalies in 5.
In our patient the HC was associated with right convex scoliosis related to syringomyelia and at our knowledge this association has never been reported. On the other hand HC has been associated with bone anomalies. In the Table 1 we report the patients in whom the bone anomalies in the setting of HC have been reported.
As happen with many congenital syndromes also in HC the anomaly may involve different body districts and our patient may be a further example of these associations.
Autosomal recessive and dominant transmission with variable expression have been documented in individuals with HC but most of the cases are sporadic. A mosaic hypothesis on the mechanism causing the HC has been proposed by Polizzi et al [5] on the basis of dermatomal distribution of the hairy with the excess hair localized in restricted areas of the body.
Conclusion
In conclusion the HC may be a simply aesthetic, benign anomaly, but may be also a clue of malformations affecting many organs including the spine and skeletal tissue.
Clinical
Hypertrichosis cubiti named also Hairy Elbow Syndrome is a common benign anomaly, in some cases associated with other abnormalities. In the presence of this cutaneous sign the diagnostic work up should be extended to the clinical and radiological investigations to exclude spine and skeletal tissue anomalies.
References
1. Flannery DB, Fink SM, Francis G, Gilman PA. Hypertrichosis cubiti. Am J Med Gen 1989;32:482-483.
2. Macdermot KD, Patton MA, Williams MJH, Winter RM. Hypertrichosis cubiti (hairy elbows) and short stature: a recognisable association. J Med Gen 1989;26:382-385.
3. Beighton P. Familial hypertrichosis cubiti: hairy elbow syndrome. J Med Genet 1970;7:158-160.
4. Martínez de Lagrán Z, González-Pérez R, Asunción Arregui-Murua M, Soloeta-Arechavala R. Hypertrichosis cubiti: another case of a well-recognized but under-reported entity. Pediatr Dermatol 2010;27(3):310-311.
5. Polizzi A, Pavone P, Ciancio E, La Rosa C, Sorge G, Ruggieri M. Hypertrichosis cubiti (hairy elbow syndrome): a clue to a malformation syndrome. J Pediatr Endocrinol Metab 2005;18(10):1019-1025.
6. Koç A, Karaer K, Ergün MA, Cinaz P, Perçin EF. A new case of hairy elbows syndrome (hypertrichosis cubiti). Genet Couns 2007;18(3):325-330.
7. Nardello R, Mangano S, Fontana A, Tripi G, Didato MA, Di Pace M, Corsello G. The hairy elbows syndrome: clinical and neuroradiological findings. Pediatr Med Chir 2008;30(5):262-264.
8. Rosina P, Pugliarello S, Tarocco M, D’Onghia FS, Barba A. Hairy elbows syndrome. Int J Dermatol 2006;45(2):127-128.
9. Sorge G, Baieli S, Mauceri L, Greco F, Fiumara A. The hairy elbows syndrome. Report of a case with a particularly severe phenotype. Ital J Pediatr 2002;28:322-325.
10. Brickell KL, Anderson NE, Charleston AJ, Hope JK, Bok AP, Barber PA. Ethnic differences in syringomyelia in New Zealand. J Neurol Neurosurg Psychiatry 2006;77(8):989-991.
11. Sakushima K, Tsuboi S, Yabe I, Hida K, Terae S, Uehara R, Nakano I, Sasaki H. Nationwide survey on the epidemiology of syringomyelia in Japan. J Neurol Sci 2012;313(1-2):147-152.
12. Vandertop WP. Syringomyelia. Neuropediatrics 2014;45:3-9.
13. Joseph RN, Batty R, Raghavan A, Sinha S, Griffiths PD, Connolly DJ. Management of isolated syringomyelia in the paediatric population–a review of imaging and follow-up in a single centre. Br J Neurosurg 2013;27(5):683-686.
14. Vandertop WP. Progression of terminal syrinx in occult spina bifida. Childs Nerv Syst 2003;19(5-6):267.
| How to Cite This Article: Pavone V, Testa G, Falsaperla R, Sessa G.Syringomyelia and Bone Malformations in the Setting of Hypertrichosis Cubiti (Hairy Elbow Syndrome). Journal of Orthopaedic Case Reports 2015 April-June;5(2):32-34. Available from:https://www.jocr.co.in/wp/2015/04/20/2250-0685-267-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


