
[box type=”bio”] What to Learn from this Article?[/box]
Description of a relatively new arthroscopic technique of Glenoid fracture fixation.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 41-43 | Prashant Acharya, Bakul Arora, Nelson Pinto. DOI: 10.13107/jocr.2250-0685.270
Authors: Prashant Acharya[1], Bakul Arora[1], Nelson Pinto[2]
[1] Department of Orthopedics, Father Muller Medical College Hospital, Mangalore – 575002, India.
[2] Department of Orthopedics, Concetta Hospital, Kinnigoli, Mangalore- 575002, India.
Address of Correspondence
Dr Prashant Acharya
Department of Orthopedics, Father Muller medical College, Kankanady, Mangalore 575002. Karnataka, India.
Email: prashantach@gmail.com
Abstract
Introduction: Intra-articular glenoid fractures are extremely rare and may be associated with other injuries. Traditionally open reduction and internal fixation has been recommended in displaced intra-articular glenoid fractures. However open reduction is difficult and it may not be possible to address the associated intra-articular soft tissue injuries. A few reports of arthroscopic assisted fixation of these fractures have been recently published. We are reporting a case of Ideberg type 3 glenoid fracture and its treatment.
Case Report: We are presenting our case where a 52 year old man presented with Type 3 intra-articular glenoid fracture. The fracture was fixed percutaneously under simultaneous arthroscopic and fluoroscopic guidance.
Conclusion: Intra-articular glenoid fractures are uncommon and difficult to treat. Arthroscopy assisted percutaneous fixation technique can be a valuable adjunct for the surgeon in dealing with not only the fracture but also the associated soft-tissue injuries.
Keywords: Glenoid fracture, shoulder arthroscopy, percutaneous
Introduction
Fractures of the scapula are uncommon and constitute less than 1% of all fractures [1]. Intra-articular Glenoid fractures form a small percentage of these scapular fractures. However their significance lies in the fact that they can lead to instability and arthritis if not treated adequately [2]. The principles of treatment of these fractures are still evolving with a lot of focus being on arthroscopic fixation in the recent years.
Case report
A 52 year old right hand dominant male patient, welder by occupation, presented with pain in right shoulder following a fall directly on the right shoulder. Radiographic evaluation revealed Ideberg type III intra-articular glenoid fracture. The patient underwent arthroscopy assisted percutaneous fixation of the fracture.
The procedure was performed with the patient in a lateral decubitus position as this facilitated simultaneous arthroscopic as well as fluoroscopic evaluation. The surgeon, the assistants and the scrub nurse were positioned posterior to the patients shoulder. The monitor was positioned on the opposite side at the foot end. The C-arm image was placed in a lateral position across the shoulder with the beam parallel to the floor. The affected limb was positioned in about 40 degree abduction and 20 degree flexion using a traction system to facilitate arthroscopic evaluation. However the traction was kept to minimum to allow manipulation of the arm during fracture reduction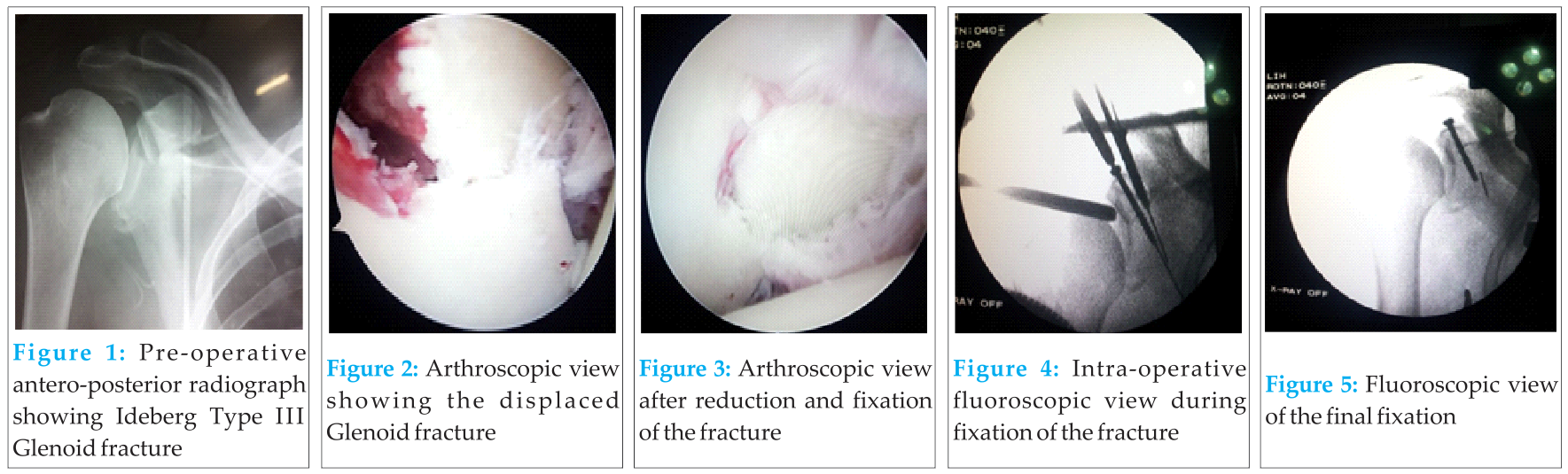
Through a standard posterior viewing portal initial diagnostic arthroscopy was performed and the fracture pattern evaluated. The joint was evaluated to rule out other soft tissue injuries. There was fraying of the margin of antero-superior labrum. A 2mm k-wire was passed percutaneously in a superior to inferior direction just adjacent to the Neviaser portal and drilled into the fractured superior glenoid fragment. This k-wire was used as a Joystick to dis-impact the fragment and restore the articular surface under direct arthroscopic vision. An arthroscopic probe introduced through an anterior working portal helped in correcting the rotation of the fracture fragment. Once a satisfactory reduction was achieved, the k-wire was advanced further into the glenoid to obtain provisional fixation.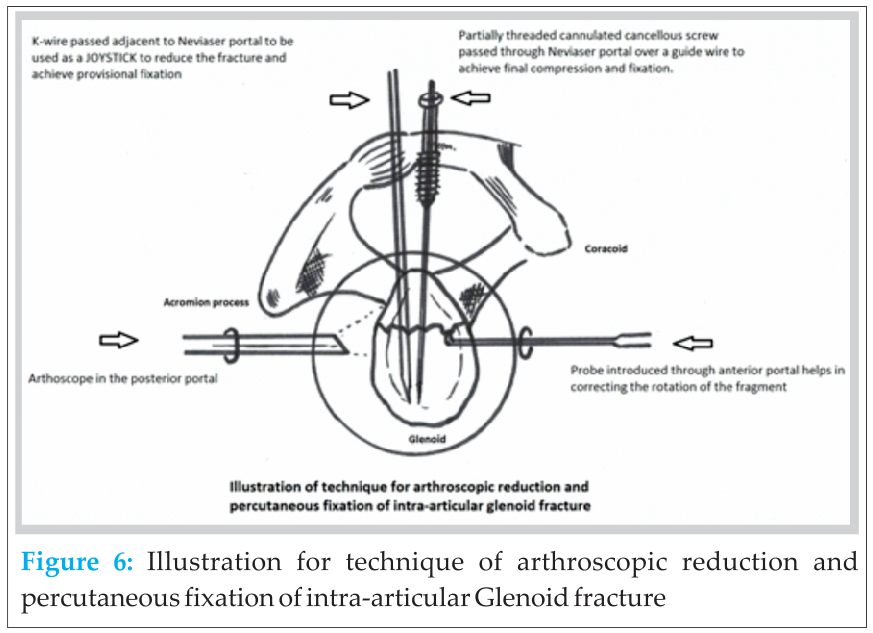
A Neviaser portal was then created and a guide wire was passed from superior to inferior direction through the centre of the fracture fragment. The correct placement of the wire was confirmed fluoroscopically. After drilling over the guide wire, definitive fixation and compression of the fracture was achieved with a 35mm partially threaded cannulated cancellous screw.The fracture reduction was again confirmed under both arthroscopic and fluoroscopic visualization. The k-wire used for provisional fixation was then removed and portals closed with simple sutures.
The operated limb was put in sling and mobilization was started as tolerated by the patient. The patient was lost to follow up after one month, by which time he was pain free and had a range of movement of 90 degree of forward elevation and abduction.
Discussion
There is a clear consensus on the need for surgical treatment of displaced intra-articular glenoid fractures [3,4,5]. An articular step-off of greater than 5 mm or instability mandates surgical intervention [6]. If not treated optimally, these fractures can result in chronic instability or post-traumatic arthritis [2]. Although surgical treatment of displaced glenoid fractures give good and predictable functional outcome, the traditionally described open reduction and internal fixation is difficult and may be associated with several complications [7]. Open surgery not only involves extensive soft tissue dissection but may also require partial removal of clavicle to gain adequate exposure for screw fixation [3]. The scarring associated with open surgery leads to poor cosmesis and difficult second surgery if required [7, 8]. Open surgery may cause weakness of external or internal rotation and anterior or posterior instability if the healing of soft tissues is not adequate [9]. Open surgery is also known to be associated with complications like blood loss, long post-operative recovery, damage to subscapularis insertion and axillary nerve injury [7, 8]. Lastly with open surgery it may not be possible to address the associated intra-articular soft tissue injuries.
Carro et al first reported the use of arthroscopy in fixation of glenoid rim fractures [10]. Since then a few reports have been published on arthroscopy assisted fixation of different types of intra-articular glenoid fractures. Presently arthroscopy is being used for the glenoid rim fractures involving greater than 15-25% of the articular surface [11]. A few reports have described the use of arthroscopy in treatment of Ideberg type III fractures where the fracture line is relatively transverse, which facilitates screw fixation in superior to inferior direction. Different methods of fixation have been described including K-wires, cancellous screws and suture anchors [2, 7]. Arthroscopy assisted technique not only facilitates accurate reduction with minimal soft tissue trauma but also allows evaluation and treatment of the other associated intra-articular soft tissue injuries.
Percutaneous screw fixation through the superior and posterior approach doesn’t put any neurovascular structures at risk [12]. However this technique is associated with learning curve and requires adequate skills and understanding of both arthroscopic and trauma surgery. Arthroscopic technique is relatively contraindicated in the presence of associated injuries like capsular ruptures and humeral avulsion of glenohumeral ligaments. The possible complications described with this technique include compartment syndrome due to fluid extravasation, anterior interroseous syndrome and injury to neurovascular structures due to incorrect portal placement [10, 13].
Conclusion
In conclusion arthroscopy assisted fixation of intra-articular glenoid fractures is still evolving as a surgical technique, but can be a valuable adjunct for the surgeon in dealing with not only the fracture but also the associated soft-tissue injuries.
Clinical
Intra-articular glenoid fractures are uncommon but significant because their treatment is difficult. Arthroscopy assisted fixation of these fractures provides an exciting option but one must understand that this technique is associated with a steep learningcurve.
References
1. Owens BD, Goss TP. Surgical approaches for glenoid fractures. Tech Shoulder Elbow Surg 2004;5:103-15.
2. Yallapragada R, Patel K, Davuluri P, Sloan A, Marynissen H. Arthroscopy-assisted percutaneous fixation of glenoid fossa fracture. Int J Shoulder Surg [serial online] 2007 [cited 2013 Nov 28];1:96-9.
3. Goss TP. Scapular fractures and dislocations: diagnosis and treatment. Journal of American Academy of Orthopaedic Surgeons 1995;3: 22-33.
4. Anavian J, Gauger EM, Schroder LK, Wijdicks CA, Cole PA. Surgical and functional outcomes after operative management of complex and displaced intra-articular glenoid fractures. J Bone Joint Surg Am. 2012 Apr 4;94(7):645-53.
5. Leung KS, Lam TP, Poon KM.Operative treatment of displaced intra-articular glenoid fractures. Injury. 1993 May;24(5):324-8.
6. Bauer G, Fleischmann W, Dussler E. Displaced scapular fractures: Indication and long-term results of open reduction and internal fixation. Arch Orthop Trauma Surg 1995;114:215-9.
7. Sugaya H, Kon Y, Tsuchiya A. Arthroscopic repair of glenoid fractures using suture anchors. Arthroscopy 2005;21:635.
8. Sears BW, Lazarus MD. Arthroscopically Assisted Percutaneous Fixation and Bone Grafting of a Glenoid Fossa Fracture Nonunion. Orthopedics 2012 Aug;35(8):1279-82.
9. Kavanagh BF, Bradway JK, Cofield RH. Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. The Journal of Bone and Joint Surgery Am. 1993 April;75(4):479-84.
10. Carro LP, Nunez MP, Llata JI. Arthroscopic-assisted reduction and percutaneous external fixation of a displaced intra-articular glenoid fracture. Arthroscopy 1999;15:211-4.
11. Calvo E, Granizo JJ, Fernandez-Yruegas D. Criteria for arthroscopic treatment of anterior instability of the shoulder: A prospective study. J Bone Joint Surg Br 2005;87:677-83.
12. Marsland D, Ahmed HA. Arthroscopically assisted fixation of glenoid fractures: a cadaver study to show potential applications of percutaneous screw insertion and anatomic risks. J Shoulder Elbow Surg. 2011; 20:481–490.
13. Sisco M, Dumanian GA. Anterior interosseous nerve syndrome following shoulder arthroscopy:A report of three cases. J Bone Joint Surg Am 2007;89:392-5.
| How to Cite This Article: Acharya P, Arora B, Pinto N. Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 41-43. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-270-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


