
[box type=”bio”] What to Learn from this Article?[/box]
Tuberculosis of wrist presents with subtle complains and should be ruled out in cases of chronic wrist pain.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 17-20 | Shardul Madhav Soman, Bhavik Nandubhai Patel, Pratik Dineshbhai Shah. DOI: 10.13107/jocr.2250-0685.335 .
Authors: Shardul Madhav Soman[1], Bhavik Nandubhai Patel[1], Pratik Dineshbhai Shah[1].
[1] Department of Orthopaedics, M.P.Shah Medical College, Jamnagar below the photo gallery. Gujarat. India.
Address of Correspondence
Dr. Shardul M Soman
ASSI Spine Fellow , Government Spine Institute and Paraplegia Hospital, Civil Hospital campus Asarwa, Ahmedabad -361008. India.
Email: somanshardul@gmail.com
Abstract
Introduction: It is uncommon for hand surgeons to diagnose and treat persistent post-traumatic radius fracture on the lines of tuberculosis infection even in developing countries especially when the clinical picture resembles more of a complex regional pain syndrome (CRPS). Although it works for many patients, some conditions that affect the wrist don’t fall in this category and worsen with this treatment practice. We present a patient who had an extra articular distal radius fracture treated initially with percutaneous pinning and was treated as CRPS for the next ten months by local physician. He was eventually diagnosed with advanced tuberculosis of the wrist and a total wrist arthrodesis was performed. Only one such case was ever reported in literature.
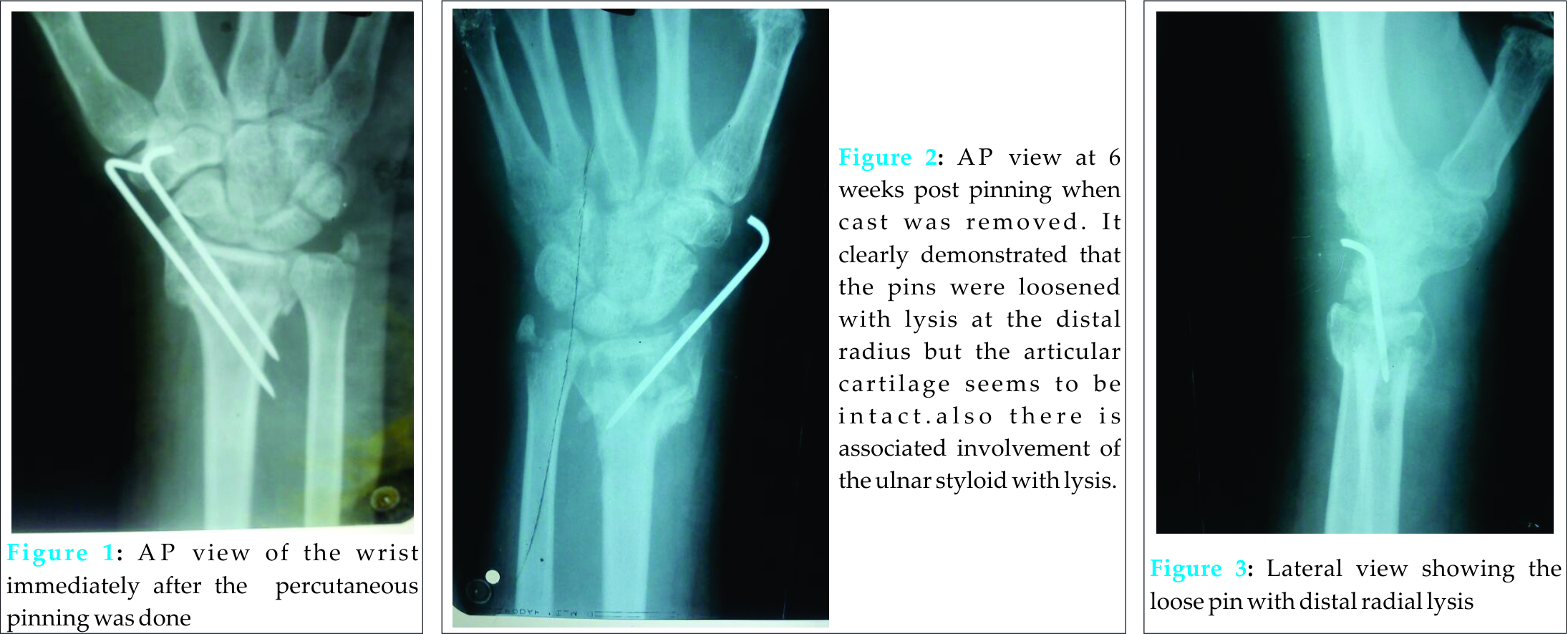
Case Report: A 50-year-old male, came to our institute with the history of pain and fullness in the wrist since one year. One year ago he had developed an extra articular fracture of the distal radius which was initially treated with percutaneous pinning and a below elbow cast for six weeks. On removal of the cast one pin was found loose and the other removed eventually after two more weeks of immobilization. Patient continued to have pain with fullness around the wrist which was treated at local place with anti inflammatory agents and ice application. Patient had complaint of other constitutional symptoms. Initially patient had full range of motion which gradually decreased. X-ray showed characteristic signs suggesting of extensive tuberculosis of distal radius which was operated with wrist arthrodesis. Per operatively, fine rice granular granulation tissue was found, histopathological examination of which confirmed the diagnosis of tuberculosis.
Conclusion: Though rare, every case of distal radius fracture complaining of chronic pain and signs suggestive of CRPS should have tuberculosis as one of the differential diagnosis, even if patient does not present any signs of tuberculosis or any primary focus is not identified. Even though skeletal tuberculosis per se is hematogenous in origin, inoculation from the pin site can be a cause and hence proper sterilization techniques should be used.
Keywords: Osteoarticular tuberculosis; arthrodesis; sterilization; inoculation.
Introduction
Osteoarticular tuberculosis is an infrequent form of the disease and accounts for only 1-5% of all cases [1, 2]. Peripheral joints are the most uncommon site of infection and present as a low-grade chronic, progressive local infection with a paucity of systemic manifestations. Most frequently tuberculosis affects the hip or knee [3]. Establishing the diagnosis is difficult in TB wrist. Culture positivity rate is 80% for synovial fluid and 90% for synovial tissue [4]. Biopsy is of particular importance in determining organism sensitivity in areas in which drug resistance is common [5]. Polymerase chain reaction (PCR) for M. tuberculosis may increase the diagnostic rate [6]. Anti-tubercular chemotherapy and immobilisation is treatment of choice, but helpful when diagnosis is established early. Since most patients present late with arthritis and deformity, they usually require wrist arthrodesis.
Case report
A 50-year-old man presented with progressive left wrist pain and swelling, following a trauma one year back, in which he fell on his left upper extremity. He was operated by percutaneous pinning for the extra-articular lower end radius fracture. Post operative period was uneventful but then patient started developing pain and fullness over the operated wrist on removal of the cast 6 weeks post-operatively with loosening of pins, which were removed. Patient continued to have fullness with gradual & progressive loss of wrist movement. Patient was treated on the lines of CRPS by local physician with non-steroidal anti-inflammatory agents. No improvement was observed and the stiffness and pain progressively worsened for the last 9 months. Past medical history was non-significant. He had no history of tuberculosis (TB) or any other immune-suppressive disease. There was neither any family history of TB infection nor of any rheumatic or autoimmune disease. He had been immunized with BCG vaccine at birth. Constitutional symptoms such as fever, anorexia, fatigue and weight loss were absent. He was not receiving any regular medications. When seen in our institute, he had considerable pain and severely restricted range of motion of the left wrist. The rest of the musculoskeletal examination was normal.
Routine laboratory investigations including biochemical tests, complete blood cell count were all normal apart from an elevated ESR (42 mm in 1st hour; normal: <20 mm in 1st hour) and CRP (8.93 mg/L; normal: <5 mg/L). Serological tests for Anti-Nuclear Antibodies (ANA) and hepatitis viruses were negative. Tumour markers and HIV test, as well as test for Brucella antibodies were also negative. The result of tuberculin skin test (5 tuberculin units) was strongly positive with induration of 17 mm diameter. His chest x-ray was normal with no evidence of any active pulmonary disease.
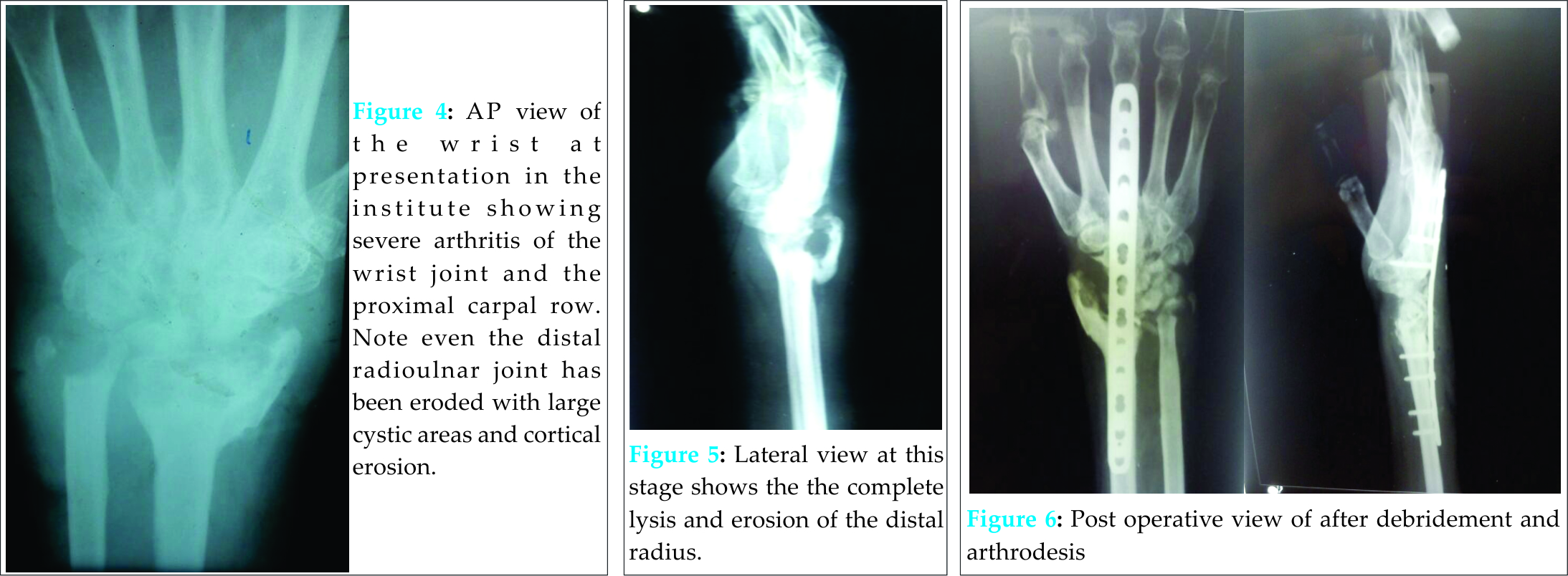
An antero-posterior radiograph of the left wrist indicated soft tissue swelling, loss of joint space, gross articular destruction with erosion and cavities throughout the carpus, distal ulna and radius with destruction of the proximal row of carpal bones. Diffuse osteoporosis of the carpal bones was also observed (Fig 2). A CT scan of the wrist showed total disappearance of bony trabeculae with marked osteoporosis and cortical cysts associated with erosions in the carpal, metacarpal bones, as well as in the ulna and radius. A diagnosis of osteoarticular TB was made depending on the clinical, radiological and pathological (biopsy) findings and he was started on anti-tubercular treatment and wrist arthrodesis performed using a wrist joint spanning plate and cancellous bone graft. Over a three-month period thereafter; his symptoms and functional disability regressed, ESR returned to normal.
Discussion
The wrist is an unusual site for osteoarticular TB. Isolated involvement of the wrist is rare and accounts for only 1 % of all cases of peripheral osteoarticular TB [9].Our case represents a number of typical features of this condition:
1) Only about one third of patients who have osteoarticular TB, have evidence of pulmonary disease and the majority of the cases have normal chest X-rays [7].
2) A history of trauma is commonly followed by inert progressive inflammation, weeks or months later [10].
3) Constitutional symptoms are usually absent & signs of inflammation are mild [11].
4) Although the symptoms may not be dramatic, chronic infection tends to be progressive and eventually results in radiographically evident destruction of cartilage and bone [1, 10].
5) Synovial fluid culture for mycobacteria is positive in only 60-80% of cases and an open synovial biopsy is frequently required to establish the diagnosis of the arthritis in the vast majority of cases [8, 11].
6) A positive tuberculin test result can be helpful in confirming a suspicious TB, but a negative result cannot rule out.
7) The diagnosis is often delayed and surgical intervention is often indicated especially when there is extensive bone and articular destruction [6].
Common radiological findings that should arouse suspicion of tuberculous arthritis include, soft tissue swelling with little periosteal reaction and periarticular osteopenia; later joint effusion, narrowing of the joint space, and finally subchondral erosion involving both sides of the joint, cortical irregularity and large areas of cystic
osteolysis [8,10]. Our patient had all these extensive radiological findings.
The radial side of the wrist (distal radius, scaphoid, trapezium, capitate, bases of second and third metacarpals) is most frequently affected. [12] Involvement of carpus leads to marginal punched out lesions due to synovial involvement or there may be cystic lesions due to intraosseous granulomas. Occasionally there have been cases of accidental inoculation of tuberculous bacilli during operative procedure but these cases are extremely rare.
The wrist joint has an articular cavity between the radius and the scaphoid on the radial side and the ulna and lunate and triquetrum on the ulnar side. This cavity does not communicate the very complex joint cavity which makes its way into all the carpal bones except the pisiform which has a separate joint cavity and articulates with only the triquetrum. Thus if the tubercle bacilli seeds in the first cavity, all the carpal bones may not be involved, whereas if the second cavity is involved they will all be involved.[13] The pisiform is almost never involved.
Osteoarthritis, rheumatoid arthritis and subacute gonorrhoeal arthritis may present with pain, swelling, disability more or less resembling tubercular arthritis. The later however is unilateral and nearly always a monoarticular affection. Though CRPS is more common cause of post traumatic local swelling at wrist joint, tuberculosis should always be ruled out by proper investigations.
Conclusion
In treatment of any case of persistent wrist one should have tuberculosis as one of the differential diagnosis even though there are no signs and symptoms suggestive of the infective etiology. Also in case of wrist tuberculosis early diagnosis with appropriate intervention in the form of modern anti-tubercular drug therapy, immobilization can help prevent the need of arthrodesis in the future. In developing conditions inoculation of tubercle bacilli through unsterile instruments could be a mode of transfer of the bacilli.
Clinical Message
Every case of distal radius fracture complaining of chronic pain and signs suggestive of CRPS should have tuberculosis as one of the differential diagnosis. In late diagnosed cases with severe joint destruction arthrodesis along with appropriate medical therapy is the key to achieve a painless stable joint.
References
1. Garrido G, Gomez-Reino JJ, Fernandez-Dapica P, Palenque E,
Prieto S. A review of peripheral tuberculous arthritis.
Semin Arthritis Rheum 1988;18:142-49.
2. Ravigliane MC, Snider DE, Kochi A. Global epidemiology of tuberculosis: Morbidity and mortality of a worldwide epidemic. JAMA 1995;273:220-26.
3. Sequeria W, Co H, Block JA. Osteoarticular tuberculosis:current diagnosis and treatment. Am J Ther 2000;7:393-8.
4. Resnick D, Niwayama G. Osteomyelitis, septic arthritis and soft tissue infection: organisms. In:Resnick D, Niwayama G., editor. Diagnosis of bone and joint disorders. Philadelphia. WB Saunders Company1995: 2448–2558.
5. Watts H, Lifso RM. Current concepts review, tuberculosis of bones and joints. J Bone Joint Surg Am 1996;78-A: 288–98.
6. Li Q, Pan Y X, Zhang C Y. Specific Detection for Mycobacterium tuberculosis In Clinical Material By PCR and Southern blot. Chin J Tuberc Respir Dis 1994; 17:238–240.
7. Gonzalez-Gay MA, Garcia-Porrua C, Cereijo MJ, Rivas MJ, Ibanez D, Mayo J. The clinical spectrum of osteoarticular tuberculosis in non-human immunodeficiency virus patients in a defined area of northwestern Spain. Clin Experimental Rheumatol 1999;17:663-69.
8. Garcia-Porrua C, Gonzales-Gay MA, Sanchez-Andrade A, Vazquez-Caruncho M. Arthritis in the right great toe as the clinical presentation of tuberculosis. Arthritis Rheum 1998; 41:374-75.
9. Turgut M. Spinal tuberculosis (Pott’s disease): its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurg Rev 2001;24:8-13
10. Resnick D, Niwayama G. Osteomyelitis, septic arthritis and soft tissue infection:organisms. In Resnick D, Niwayaoarticularma G (eds). Diagnosis of bone and joint disorders. WB Saunders Company, Philadelphia 1995, pp:2448-2558.
11. Watts HG, Lifeso RM. Current concepts review. Tuberculosis of bones and joints. J Bone Joint Surg Am 1996; 78A:288-99.
12. Davidson P, Horowitz I. Skeletal tuberculosis. Am J Med 1970; 48: 77-84.
13. Hodgson; Smith, Taylor King. Clinical Orthopaedics & Related Research: March/April 1972 ; Volume 83:Issue – 73-83.
| How to Cite This Article: Soman SM, Patel BN, Shah PD. Persistent Posttraumatic Wrist Pain – Tuberculosis Infection Should be in the Differential Diagnosis. A Rare Case Report. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 17-20. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-335-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


