
[box type=”bio”] What to Learn from this Article?[/box]
The joint should be preserved after hip fracture in physically active patients. If hip arthroplasty is performed in physically active patient after failure of joint preserving treatment options, activity should be limitted to moderate intensity after surgery.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 21-23 | Deniz Cankaya, Burak Yoldas, Serdar Yılmaz, Ali Tecirli1, Bulent Ozkurt. DOI: 10.13107/jocr.2250-0685.336 .
Authors: Deniz Cankaya[1], Burak Yoldas[1], Serdar Yılmaz[1], Ali Tecirli[1], Bulent Ozkurt[1]
[1] Department of Orthopaedic and Traumatology, Ankara Numune Training and Research Hospital. Turkey.
Address of Correspondence
Dr. Deniz Cankaya,
Department of Orthopaedic and Traumatology, Ankara Numune Training and Research Hospital. Turkey.
Email: cankayadeniz78@gmail.com
Abstract
Introduction: Fracture of the femoral stem following hip arthroplasty has become very rare since the developments in modern prosthetic designs. Prevention by identifying the risk factors is the best way to overcome these complex problems, as treatment is difficult.
Case Report: Femoral component fracture after cemented hemiarthroplasty in a physically active 64- year-old, male patient is reported in this present article.
Conclusion: The present case emphasizes the importance of preserving the joint after hip fracture and avoidance of using monoblock prosthesis in younger patients.If the patient is physically active, he/she should be advised to limit her/his daily activities to moderate intensity after hemiarthroplasty surgery.
Keywords: hemiarthroplasty, stem fracture, physically active.
Introduction
Femoral stem fracture is a devastating complication of hip arthroplasty. Fortunately, the development of new generation femoral prostheses decreased the rate of femoral stem fractures dramatically [1, 2]. Currently, in view of the advances in design, metallurgy, and cementing techniques, fracture of a femoral stem after total hip arthroplasty is very rare, [3]. Additionally, the low activity level and shorter life expectancy of the patients make this complication even rarer after hemiarthroplasty.
We report a case of a femoral stem fracture in a physically active adult male patient who underwent cemented hip hemiarthroplasty eight years ago.
Case Report
A 64-years-old man, who had suffered from right hip pain after jumping on the floor from 15 cm height two months ago, was seen at the orthopaedic outpatient department of a local hospital. As his pain persisted despite treatment, he was admitted to our hospital. The patient was 68 kg, 170 cm tall with a calculated body mass of 23.53 kg/cm2. He had undergone right hip cemented hemiarthroplasty after displaced femoral neck fracture caused by a motor vehicle accident eight years ago, when he was 56 years old. After the surgery, he had been controlled regularly every year for three years, and then he was lost to follow-up.
Two months earlier, he experienced a significant pain in his right hip and an analgesic drug was prescribed to him at a local hospital. As his pain increased with time, he was admitted to our hospital; radiographs taken shortly thereafter revealed a fractured femoral prosthesis (Fig.1). Physical examination revealed a healthy-appearing elder man in no acute distress with normal examination of the lower extremities. There was a well-healed posterior incision over the right hip without any evidence of skin infection. Active and passive movements of the hip caused pain. C-reactive protein, erythrocyte sedimentation rate and the other laboratory parameters were in normal range.
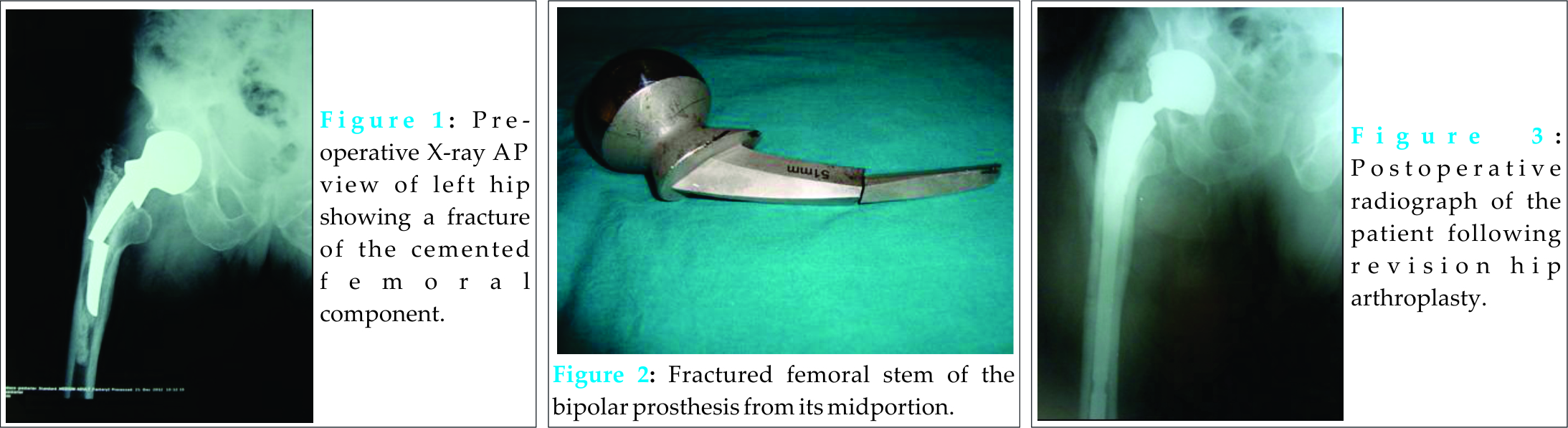
Four days later, he underwent a revision arthroplasty of the right hip. A modified Watson-Jones approach was used and the proximal part of the fractured Thompson’s prosthesis (51 mm sized) was extracted while the hip was dislocated. In order to extract the distal part of the femoral stem and cement, an anterior window was created at the distal part of the femur to the tip of the femoral stem, and cement mantle and the distal part of the fractured stem was extracted. The breakage occurred in the middle part of the femoral stem (Fig.2). Both parts of the femoral stem were found to be poorly fixed and easily extracted. A fully porous coated femoral stem (70 mm proximal body and 12/200 mm distal) was implanted (Fig 3). There was no post-operative complication and the patient was ambulated with partial weight-bearing on the second day after surgery. Patient was administered analgesics to reduce pain and first generation cephalosporin to prevent infection. Low molecular weight heparin was administered for 6 weeks postoperatively to prevent deep vein thrombosis Muscle strength training was commenced on 3rd day postoperatively alker use was initiated in the hospital and discontinued in the 3rd week following surgery. Patient underwent regular sessions of outpatient or home-based physical therapy. Follow-up visits were performed at 6 weeks; at 3, 6, and 12 months after surgery.The Harris hip score of the patient at 1-year follow-up was 88 and there was no complication during first year follow-up.
Discussion
Femoral stem fractures associated with hip arthroplasty is a serious clinical problem (4). Fortunately, fracture of a femoral prosthesis is not a frequent occurrence. Design of the prosthesis, type of the surgery, body mass index and activity level of the patient are important factors affecting the risk of stem fractures (1-6).
In their case reporting femoral stem fracture after cemented total hip arthroplasty, Jarvi et al. (7) addressed poor proximal support leading to cantilever-bending stresses on the middle part of the femoral stem as a main factor causing the fracture. In a report of ten cases, Woolson et al. (2) concluded that proximal debonding at the cement-prosthesis interface combined with a stem well-fixed distally was a cause of femoral stem fractures after cemented total hip arthroplasty. If the patient is physically active, femoral stem fracture associated with poor proximal support becomes a matter of concern (5, 6). Garg et al. (6) highlighted that active patients carrying risk factors for implant failure after hip arthroplasty should be recommended to limit their activity.
In the present case; the pre-operative X-ray revealed that the cemented femoral stem was relatively well-fixed in the distal part when compared to the proximal part. Our patient underwent cemented hemiarthroplasty when he was 56 years old. He was a very healthy and physically active man even eight years afterthe surgery. However, internal fixation was not considered and hip joint was not preserved despite the relatively young age of the patient for hemiarthroplasty. Although there was radiographic evidence of a possible failure of hemiarthroplasty, the patient who was physically very active had not been informed about the possible complications of hemiarthroplasty and his activities had not been limited in the follow-up period. Furthermore, a monoblock prosthesis was used instead of a bipolar prosthesis, despite the fact that monoblock prosthesis was a more proper choice for very elderly patients (8).
Conclusion
Present case emphasizes the importance of preserving the joint after hip fracture and avoidance of using monoblock prosthesis. Additionally, if the patient is physically active, he/she should be advised to limit her/his activity to moderate intensity after surgery.
Clinical Message
Hemiarthroplasty is not appropriate treatment choice for hip fracture in physically active patients.However, if hemiarthroplasty is performed for physically active patient, it is important to avoid using of monoblock prosthesis and advise patient to limit her/his daily activities to moderate intensity.
References
1. Dall DM, Learmonth ID, Solomon MI, Miles AW, Davenport JM. Fracture and loosening of Charnley femoral stems. Comparison between first-generation and subsequent designs. J Bone Joint Surg Br. 1993;75:259-65.
2. Woolson ST, Milbauer JP, Bobyn JD, Yue S, Maloney WJ. Fatigue fracture of a forged cobalt-chromium-molybdenum femoral component inserted with cement. A report of ten cases. J Bone Joint Surg Am. 1997;79:1842-8.
3. Della Valle AG, Becksaç B, Anderson J, Wright T, Nestor B, Pellicci PM et al. Late fatigue fracture of a modern cemented [corrected] cobalt chrome stem for total hip arthroplasty: a report of 10 cases. J Arthroplasty. 2005;20:1084-8.
4. Magnissalis EA, Zinelis S, Karachalios T, Hartofilakidis G. Failure analysis of two Ti-alloy total hip arthroplasty femoral stems fractured in vivo. J Biomed Mater Res B Appl Biomater. 2003;66:299-305.
5. Garg B, Mittal R, Rastogi S. Femoral prosthesis neck fracture following total hip arthroplasty: a case report. Acta Orthop Belg. 2011;77:406-9.
6. Huot Carlson JC, Van Citters DW, Currier JH, Bryant AM, Mayor MB, Collier JP. Femoral stem fracture and in vivo corrosion of retrieved modular femoral hips. J Arthroplasty. 2012;27:1389-1396.
7. Jarvi K, Kerry RM. Segmental stem fracture of a cemented femoral prosthesis. J Arthroplasty. 2007;22:612-6.
8. Bauer S, Isenegger P, Gautschi OP, Ho KM, Yates PJ, Zellweger R. Cemented Thompson versus cemented bipolar prostheses for femoral neck fractures. Journal of Orthopaedic Surgery 2010;18:166-71.
| How to Cite This Article: Cankaya D, Yoldas B, Yilmaz S, Tecirli A, Ozkurt B. Fracture of the cemented femoral component following hemiarthroplasty in physically active patient: A case report . Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 21-23. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-336-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


