
[box type=”bio”] What to Learn from this Article?[/box]
Rare diagnosis like congenital insensitivity to pain should be kept in mind while dealing with unusual limb swellings in pardiatric age group.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 78-80| M Javed Shaikh, C Rex, R Vignesh, Madhav Chavan. DOI: 10.13107/jocr.2250-0685.446
Authors: M Javed Shaikh[1], C Rex[1], R Vignesh[1], Madhav Chavan[2]
[1]Department Of Orthopaedics, REX Ortho hospital, Coimbatore. Tamil Nadu
[2]Department Of Paediatrician, REX Ortho hospital, Coimbatore. Tamil Nadu.
Address of Correspondence
Dr. Javed Shaikh,
Gulistan Bunglow, Yashdha Colony, Rahatani Phata, Pimpri, Pune – 411017. India.
E-mail: mjishaikh@gmail.com
Abstract
Introduction: Congenital insensitivity to pain (CIP) is a rare disorder, and often presents to an orthopaedic surgeon as recurrent fractures, dislocations, pseudoarthrosis, osteomyelitis etc. Here, we report a case of congenital insensitivity to pain presenting with distal femoral physeal separation in a child.
Case Report: A 12-year-old girl child came with complaints of limp while walking and swelling in the left knee for past 5 weeks. Mother gave a history that the girl is a known case of congenital insensitivity to pain with clear history of no pain on intramuscular injection since birth. She was born of consanguineous marriage and had no significant trauma, fever, other joint involvement or any features of rheumatism. On local examination, she had no bony tenderness, mild warmth, and moderate knee effusion with restricted range of movement. Plain radiograph showed epiphysiolysis of distal femur with widening of physis. Examination under anaesthesia demonstrated gross movement indicating lower femoral physeal separation. This unstable distal femoral epiphysis was treated under general anaesthesia with closed reduction, percutaneous cross pinning and above knee plaster cast.
Conclusion: Congenital insensitivity to pain (CIP) is a rare disorder to diagnose. Emphasis is given on early diagnosis of orthopaedic problems and prompt treatment, educating parents and prevention of accidents. Physeal separation without significant trauma must prompt an orthopaedic surgeon to think about congenital insensitivity to pain as a differential diagnosis.
Key words: Congenital insensitivity to pain, physeal separation.
Introduction
Congenital insensitivity to pain (CIP) is a rare disorder, which comes under group of hereditary sensory and autonomic neuropathies (HSAN). In this condition, patient has insensitivity to deep pain only, but superficial sensation and deep tendon reflexes are normal. Affected individuals at times have associated anhydrosis. Orthopaedic complications of congenital insensitivity to pain are recurrent fractures, dislocations, pseudoarthrosis, osteomyelitis, and charcot arthropathy [1]. We report a rare case of congenital insensitivity to pain presenting with physeal separation in a child similar to neuropathic joint in adults.
Case Report
A 12-year-old girl child came with complaints of limp while walking and swelling in the left knee for past 5 weeks (Fig. 1: clinical picture). Mother gave history that the girl is a known case of congenital insensitivity to pain with clear history of no pain on intramuscular injection since birth. The diagnosis was made by our senior neurophysician on the basis of clinical examination and findings of sensory and motor system. The diagnosis of congenital insensitivity to pain is done by positive family history and characteristic symptoms. Nerve conduction studies and EMG has no role in diagnosis of this condition and it was not recommended in this child by our neurophysician. Genetic studies were not done, as it only reflects the way of inheritance and will not add to the diagnosis, but were advised to the parents while counselling. She had no significant trauma, fever, other joint involvement or any features of rheumatism. Physical examination of the skin, nails, heart and lungs were unremarkable. On local examination, she had no bony tenderness, mild warmth, and moderate knee effusion. Range of movement was terminally restricted, with normal distal pulse, power and deep tendon reflex. Pin prick sensation was normal. Plain radiograph showed epiphysiolysis of distal femur with widening of physis (Fig. 2: radiograph showing distal femoral epiphysiolysis). Knee aspirated in emergency department showed straw coloured synovial fluid. Synovial fluid analysis for microscopic and biochemical parameters were normal. Blood tests for infection, clotting profile and arthritis profile markers were normal. Examination under anaesthesia demonstrated gross movement at physis on varus, valgus stress views under fluoroscopy guidance indicating lower femoral physeal separation. This unstable distal femoral epiphysis was treated under general anaesthesia with closed reduction, percutaneous cross pinning [2] and above knee plaster cast (Fig. 3: post-op radiograph). After 8 weeks (Fig. 4: 8 weeks post-op radiograph), the pins were removed in emergency department and knee range of motion exercises started. Twelve weeks follow-up showed complete disappearance of swelling around the knee and child could walk normally with no limp. Radiograph showed increased radio-opacity (healing) at physis. As a measure of prevention of further fractures, we advised her to use preventive splints during any vigorous activity. At 1-year follow-up, the patient was perfectly normal with no signs and symptoms around knee and normal physeal growth.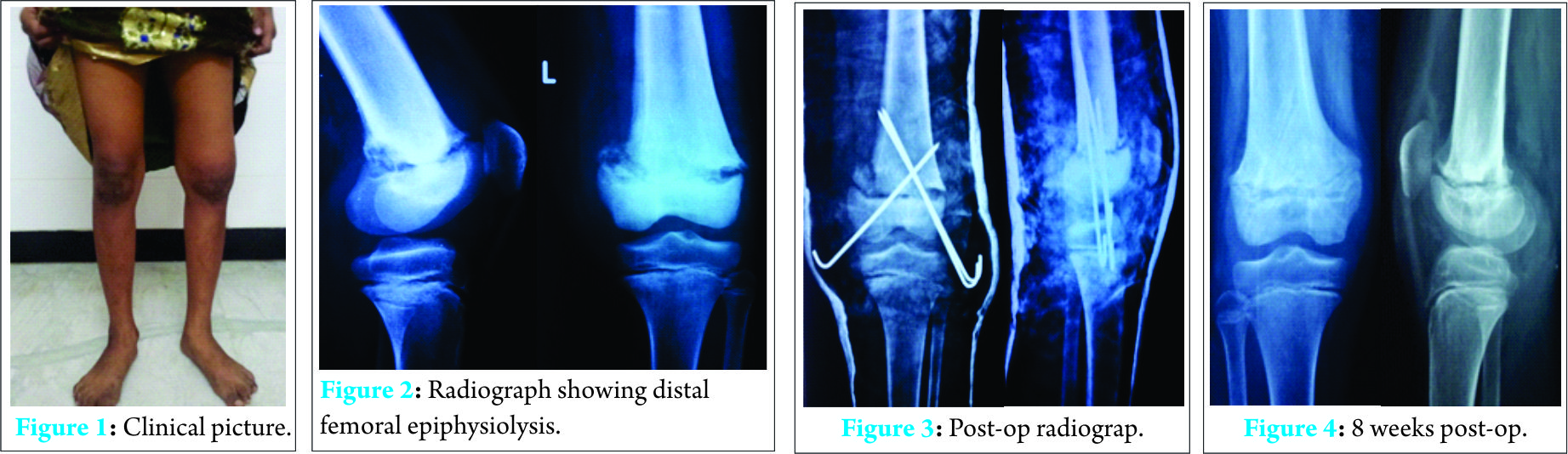
Discussion
Congenital insensitivity to pain is a rare inherited disorder first described by Dearborn in 1932 [2]. It can be inherited as autosomal dominant or recessive, and can be sporadic. The disorder is characterized by absence of reaction to painful stimuli, self-mutilating behaviour and anhydrosis. Dyck in 1984 divided these neuropathies into five types [3]. Out of 5 subtypes of HSAN, congenital insensitivity to pain with anhydrosis (HSAN-IV) and congenital insensitivity to pain (HSAN-V) is very common. Type IV patients usually develop complication due to anhydrosis and do not survive beyond 3 years of age. Our patient had an impaired sense of pain which was noticed from birth had no mental retardation, normal muscle tone and normal nerve conduction velocity suggests the diagnosis of HSAN type 5. The aetiology is not clear. One recent study claims mutation in the sodium channel (Nav1.7) encoded by the SCN9A gene located on the chromo- some 2q24.3 causes inability to experience pain [4]. Congenital insensitivity to pain usually manifests with multiple joint involvement and recurrent fractures. We are reporting the first case of isolated physeal separation of distal femur as a manifestation due to congenital insensitivity to pain. Isolated distal femur epiphysiolysis consists of nearly 3% of all physeal fractures [2]. As the aetiopathogenesis of physeal separation (macro/micro trauma) is similar to neuropathic joint, the similar line of management was followed in our case to hasten the healing process by temporary immobilisation with K-wires and cast [5]. The disappearance of swelling and normal temperature at the knee is an indication of normal healing. There is no single gold standard drug available for this condition. Reports suggest naloxone and naltrexone can be used to reverse the analgesia [6], but there is no strong evidence to support these drugs.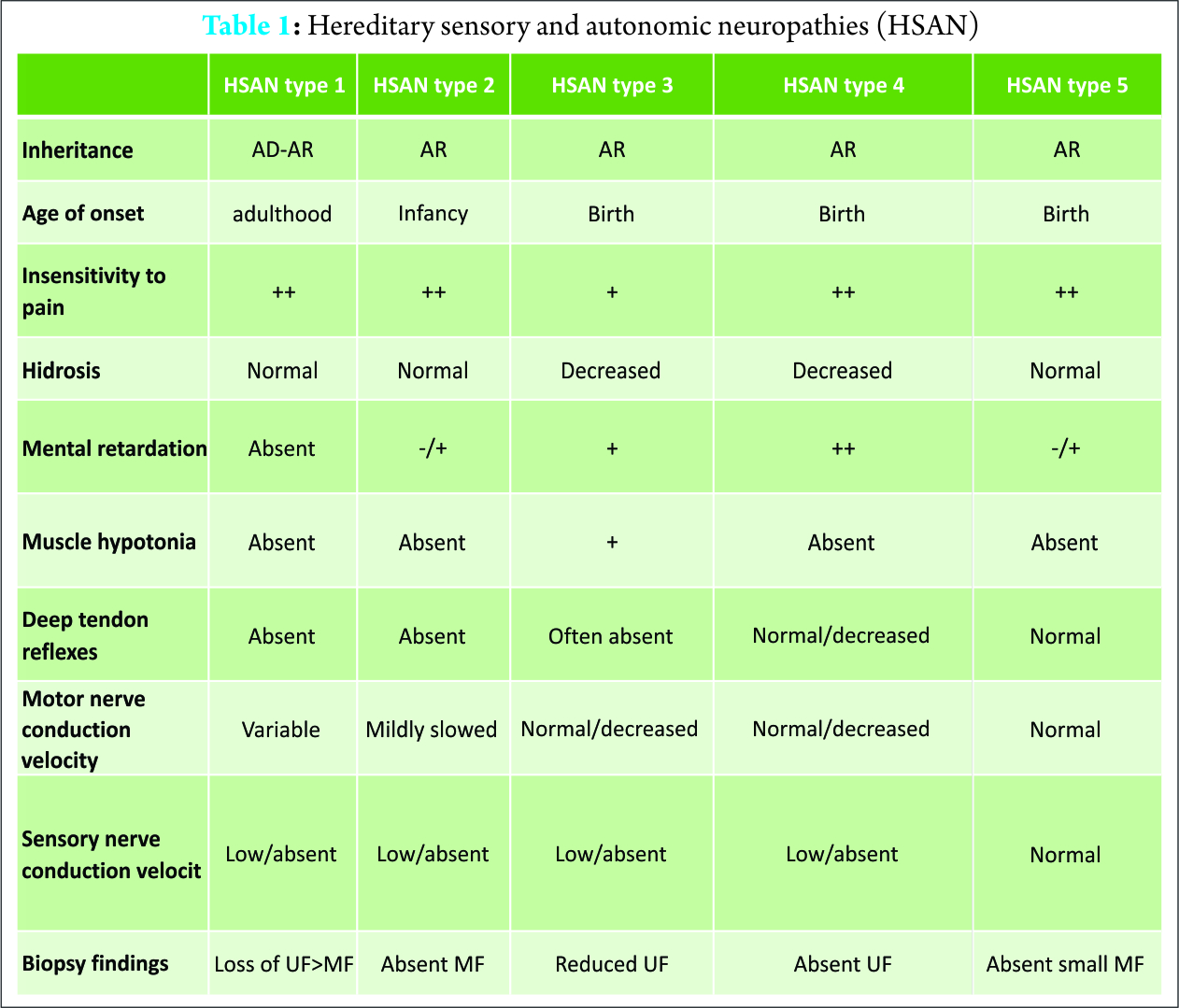
Conclusion
Exclusive distal femoral epiphysiolysis is an extremely rare presentation in congenital insensitivity to pain. But diagnosis at right time and intervention can save patient’s life and give better functional outcome. Protective splints may prevent further fractures and neuropathic joint formation.
Clinical Message
In congenital insensitivity to pain, emphases is given on early diagnosis of orthopaedic problems and prompt treatment. Parents should be educated for regular medical check up of the child, prevention of accidents, proper family planning and genetic counselling to avoid consanguineous marriages. The other relatives should also be counselled to prevent happening of such cases in their family. These cases appear due to consanguinity. Physeal separation without significant trauma must prompt an orthopaedic surgeon to think about congenital insensitivity to pain as a differential diagnosis.
References
1. E.bar-on et al. Congenital insensitivity to pain, orthopaedic manifestation. J Bone Joint Surg [Br] 2002;84-B:252-7
2. Dearborn G. A case of congenital general pure general analgesia. J Nerve Mint Dis1932;75:612
3. Dyck PJ. Normal atrophy and degeneration predominantly affecting peripheral sensory and autonomic neurons. Peripheral Neuropathy. 3rd edition. Philadelphia, etc. W.B. Sanders Company 1993:1065-93
4. Drenth JPH, Waxman SG. Mutations in sodium-channel gene SCN9A cause a spectrum of human genetic pain disorders. J. Clin. Invest 2007;117(12):3603-3609.
5. Garrett BR, Hoffman EB, Carrara H: The effect of percutaneous pin fixation in the treatment of distal femoral physeal fractures. J Bone Joint Surg Br 2011;93:689-219.
6. Protheroe SM. Congenital insensitivity to pain. Journal of the Royal Society of Medicine 1991;84:558-559.
| How to Cite This Article: Shaikh MJ, Rex C, Vignesh R, Chavan M. Slipped Distal Femoral Epiphysis in Congenital Insensitivity to Pains. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 78-80. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-446-ful |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


