
[box type=”bio”] What to Learn from this Article?[/box]
How erythromycin sclerotherapy can be an effective and safe option for the treatment of seroma in orthopedic surgery.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 92-94| Martin Salgado, Felipe Fernández, Carolina Avilés, Cecilia Cordova. DOI: 10.13107/jocr.2250-0685.454
Authors: Martin Salgado[1],[2], Felipe Fernández[1], Carolina Avilés[1], Cecilia Cordova[1]
[1]Department of Traumatology and Orthopedics Hospital of the Catholic University of Chile. Santiago, Chile.
[2]Section of Reconstructive Joint Surgery Division: Pelvis, Hip and Thigh. Dr. Sotero del Rio Hospital. Santiago, Chile.
Address of Correspondence
Dr. Martin Salgado,
Marcoleta 352, 2nd Floor, Santiago, Metropolitan Region. Chile. Postal Code: 8330033.
E-mail: msalgadog@gmail.com
Abstract
Introduction: The presence of postoperative seromadesis is common, corresponding to the presence of serum in the subcutaneous tissue post a surgical event. Erythromycin has been reported as sclerosing, although not in orthopedic surgery. We report a case of erythromycin seromadesis in orthopedic surgery.
Case Presentation: We present a case of a 63-year-old woman having undergone femoral prosthesis surgery and total hip replacement with a subfacial seroma without findings of infection, refractory to standard treatment of compression bandages, massage and cleaning surgery in two oportunities. A literature review was undertaken to obtain the therapeutic alternatives where erythromycin seromadesis is chosen with excellent response.
Conclusion: Erythromycin sclerotherapy should be considered as an effective and safe option in the treatment of seroma in general surgery and traumatology. More studies are necessary to get a better evidence. We believe that this is the first study of use of erythromycin as sclerotherapy in a traumatology case.
Keywords: Seromadesis, Erythromycin, Arthroplasty.
Introduction
A seroma is the collection of fat, liquid, serum and lymph in one area of the body following a traumatic or surgical event. Usually, it is formed in a wound in the immediate postoperative period, usually in the first week, although it may be delayed. It is a common complication in mastectomies, herniorrhaphies and plastic surgery. Generally it is benign, but often annoying to the patient and has a moderate risk of infection. The presence of a seroma may be asymptomatic, or may have swelling, pain and exude from the wound. The diagnosis can be by inspection and palpation of the wound, with computed tomography and the ultrasound beign useful for identifying fluid collection. Seroma’s have been seen in orthopaedic surgery as well, where they are likely to have serious repercussions. This is true especially in prosthetic surgery,with greater chances of infection of prosthetic components and failure of the joint replacement associated with high costs, lengthy hospitalizations, and at times need for a subsequent surgery. Treatment options can be categorized as preventive or curative, xonsisting of intraoperative application of sclerosing chemicals as hypertonicsaline [1] and talc [2] in humans and gram positive anaerobe like Corynebacterium parvum in rat models [3], tissue adhesives (fibrin or platelet concentrates), use of negative pressure drainage, repeated percutaneous aspiration and surgical drainage with complete removal of seroma and its capsule. There is no evidence of a clear superiority of one method over the other. The use of erythromycin as a sclerosing agent was described in animal studies, that was first assessed as a pleural sclerosant, proving effective and with fewer sideeffects than talc, tetracycline and diazepam. This is used safely in humans in the management of breast surgeries [4], non neoplastic ovarían cysts [5] and pleurodesis. There are no reports of its use in orthopedics, and we believe that this is the first study of this kind.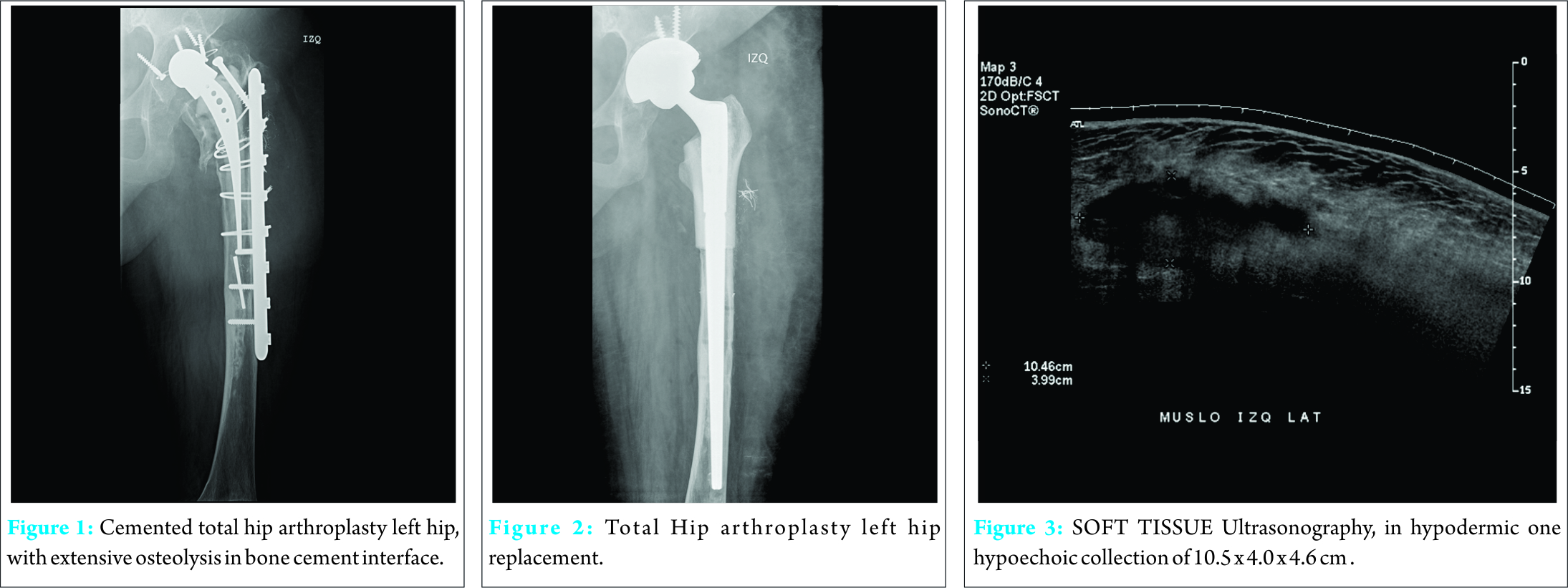
Case Presentation
A female patient of 63-year-old presented to our orthopaedic department with prosthetic loosening of the isoelastic stem (Fig. 1), also femur and acetabulum with massive osteolytic defect performed by modular aloprosthesis of proximal femur and acetabulum of tantalum, and metal on polyethylene pair of friction (Fig. 2). Patient had good clinical evolution with the drain removed at the first postoperative day with output of 100 cc. serohematic. Patient was discharged in good condition on the fifth postoperative day. Five days later, patient was re-admitted to the emergency room for increased volume in relation to wound without infectious signs. The blood inflammatory parameters are normal. Soft tissue ultrasonography subfascial evidence seroma with estimated volume of 500 cc is taken. (Fig. 3). To avoid superinfection of a large extent surgery, it was decided to make an early cleaning surgery, in order to drain and take tissue samples and fluid culture. A collection is located under muscle planes adjacent to the aloprotesis, with communication between up fascia lata muscleplane. After the cleaning surgery and drainage, equally the seroma is maintained for 5 days with daily output of 200 cc of serous fluid. It was decided to perform a new scouring, with obliteration of third space, massage and Compression bandages. Negative cultures were obtained. Given the persistence of seroma, a literature review was undertaken to obtain therapeutic alternatives. Finally, surgical cleanliness was performed with resection of pseudocapsule seroma with curettage, making crops and application of 2 g. erythromycin diluted in 200 cc.of 0.9% saline solution. Customary closing was performed flat leaving a aspiration drainage N° 9 undert he fascia, which was measured daily. The next day, the drainage measured serohematic liquid 100cc, and 60cc was measured on the 2nd day. On the 3rd day, 10 cc of liquid was measured, and the drainage was removed on the 4th day. Subsequently, the patient was discharged in good condition without signs of infection, tension, edema or collection in the thigh wound.
Discussion
It has been assessed that there are certain factors that could favor the formation of seroma, such as a high bodymass index, use of electrocautery to dissect, early withdrawal of drain (within 24 hours), obliteration of dead space and use of drains under vacuum. In our case, it is highlighted that the drainage was removed on the first postoperative day, which could have favored the formation of seroma. Although, maintaining a drainage for more number of days also increases the risk of infection. It is important to consider the differential diagnosis of surgical wound infection, hence blood inflammatory parameters were evaluated, and fluid cultures of the wound were taken. If an infection is confirmed, systemic antibiotic treatment should be given. In addition, open the wound, drain the liquid and perform irrigation and debridement folllowed by wound closure. In the search for bibliographical studies, with terms “Mesh” in PubMed for “Seroma” and “Erythromycin” a single study was located, Ali-Khan et al. 2009, which refers to the use of erythromycin as sclerotherapy in the management of seroma in series of patients of plastic surgery, showing effectiveness and no serious complications [6]. The search for terms “Mesh” in PubMed for “Seroma” and “Sclerotherapy”, located two investigations, Throckmorton et al. in 2008 with povidoneiodine or ethyl alcohol in postmastectomy [7] and Moritz et al. in 2013 with polidocanol in varicose vein surgery [8]. The current evidence allows the use of this therapy in this patient, although there is no evidence in trauma surgery. It is necessary to conduct more studies to evaluate the effectiveness and reproducibility of this therapy.
Conclusion
It is known that erythromycin as sclerosing product tends to be very effective with fewer adverse effects than other compounds used for the same condition. It has evaluated with satisfactory results in pleurodesis, non-neoplastic adnexalcyst, and plastic surgery. Erythromycin use as sclerosing product in orthopedic surgery must be evaluated as a effective and safe therapeutic alternative.
Clinical Message
The presence of a seroma may facilitate a surgical infection and surgical failure. Small seromas can be managed expectantly, while large collections should be drained. Safe and efficient sclerosing products may be used as associated therapy. Erythromycin also seems to be an excellent example in orthopedic cases.
References
1. Gruver DI. Hypertonic saline for treatment of seroma. PlastReconstrSurg.
2003;112:934.
2. Saeb-Parsy K, Athanassoglou V, Benson JR. Talc seromadesis: a novel technique for the treatment of chronic seromas following breastsurgery. Breast J 2006;12:502-4.
3. Tekin E, Kocdor MA, Saydam S, Bora S, Harmancioglu O.Seroma prevention by using Corynebacterium parvum in a rat mastectomy model. EurSurg Res. 2001;33:245-8.
4. Srivastava V, Basu S, Shukla VK. Seroma Formation after Breast Cancer Surgery: What We Have Learned in the last two decades. Journal of Breast Cancer 2012;15(4):373-380.
5. Kafali H, Yurtseven S, Atmaca F, Ozardali I. Management of non-neoplastic ovarían cysts with sclerotherapy. Int J GynaecolObstet. 2003;81:41-5.
6. Ali-Khan A S, Orlando A, Kenealy J Erythromycin sclerotherapy in the management of seroma J PlastReconstrAesthetSurg. 2009;62(3):e55–e58..
7. Throckmorton AD, Askegard-Giesmann J, Hoskin TL, Bjarnason H, Donohue JH, Boughey JC, et al. Sclerotherapy for the treatment of postmastectomy seroma. Am J Surg. 2008;196:541-4.
8. Moritz RK, Reich-Schupke S, Altmeyer P, Stücker M. Polidocanol foam sclerotherapy of persisting postoperative seromas after varicose vein surgery: a series of six cases. Phlebology 2013 Oct;28(7):341-6.
9. Miller Q, Meschter C, Neumaster T, et al. Comparison of pleurodesis by erythromycin, talc, doxycycline, and diazepam in a rabbit model. J SurgEduc 2007;64:41e5.
| How to Cite This Article: Salgado M, Fernández F, Avilés C, Cordova C. Erythromycin Seromadesis in Orthopedic Surgery. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 92-94. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-454-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


