
[box type=”bio”] What to Learn from this Article?[/box]
Hip arthroscopy is a proper technique for removal of the foreign materials from the joint, and open surgery must be reserved for further complications as in this case report.
Case Report | Volume 6 | Issue 4 | JOCR September-October 2016 | Page 13-16| Mehmet Faruk Çatma, Serhan Ünlü, Önder Ersan, Alper Öztürk.
DOI: 10.13107/jocr.2250-0685.548
Authors: Mehmet Faruk Çatma[1], Serhan Ünlü[1], Önder Ersan[1], Alper Öztürk[1]
[1]Department of Orthopaedics and Traumatology, Diskapi Training and Research Hospital, Ankara, Turkey.
Address of Correspondence
Dr. Alper Öztürk,
Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Irfan Bastug St. No 38/1 Altindag, Ankara, Turkey.
E‑mail: alperozturkort@gmail.com
Abstract
Introduction: There have been several reports on arthroscopically assisted removal of the bullet imbedded in hip joint in the literature. Similarly in this case, a bullet lodged in acetabulum was extracted with arthroscopic technique. What makes this case unique in the literature is that the bullet removed from the acetabulum traversed the femoral neck.
Case Presentation: Male patient aged 32 with a low-velocity gunshot wound was referred to emergency room on August 28, 2012. The projectile was lodged in acetabular side of hip joint transversing through femoral neck. A hip arthroscopy was performed for bullet removal. Two years after surgery patient had groin pain and underwent a safe dislocation for femoral chondral injury. In last follow up in the second postoperative year, the patient had no clinical complaint.
Conclusion: Hip arthroscopy is a minimally invasive and proper procedure for removal of foreign materials like a bullet in hip joint. Arthrotomy can be reserved for further complications like chondral injury as in this case.
Keywords: hip joint arthroscopy, wound, safe surgical dislocation.
Introduction
Low-velocity gunshot wound has been encountered with increasing frequency. Foreign materials in the soft tissue caused by gunshot wound can be managed with antibiotic treatment and superficial debridement [1]. However, it is suggested that foreign materials sucked into joint be removed in an attempt to prevent joint arthropathy, cartilage damage and septic arthritis [2]. Not long ago, arthrotomy was a technique used to remove intra-articular foreign materials. Nowadays, arthroscopic methods are opted for the removal of intra-articular foreign body. Arthroscopic methods for the removal of intra-articular foreign material are described for the knee, the hip, the ankle and the shoulder [3].
We are unaware of any report describing removal of a bullet imbedded in acetabulum passing through the femoral neck. This makes our report unique when compared with the other reports on arthroscopically assisted bullet removal.
Case Presentation
Male patient aged 32 with a low-velocity gunshot wound was referred to emergency room on August 28, 2012. Wound debridement, tetanus prophylaxis and antibiotic treatment were initially administered for the management of the wound. Physical examination showed that entry wound was placed 1 cm lateral to femoral artery, 10 cm distal and 5 cm medial to spina iliaca anterior superior (Fig. 1). There was no exit wound. The patient had limited and painful hip joint movements. His neurovascular condition was intact.
The relation of the projectile lodged in acetabulum with the joint and its path through the femoral neck was seen at radiography and CT scanning (Fig. 2). The patient was operated two days after the gunshot wound. Hip arthroscopy was performed using the supine position with the extremity in traction on a fracture table with general anesthesia. Traction weight of 30 kg was applied to the left hip joint of the patient. Hip joint was entered by making anterior and anterolateral portals. The projectile was found to be subchondrally located in posterior superior acetabulum, relating with the joint (Fig. 2). Exit point of the projectile was seen on the femoral side and chondral damage was treated with debridement. The surrounding of the projectile lodged in the acetabular side was enlarged with a probe for the removal of it. Projectile loosened with a probe was safely removed with a grasper (Fig. 2).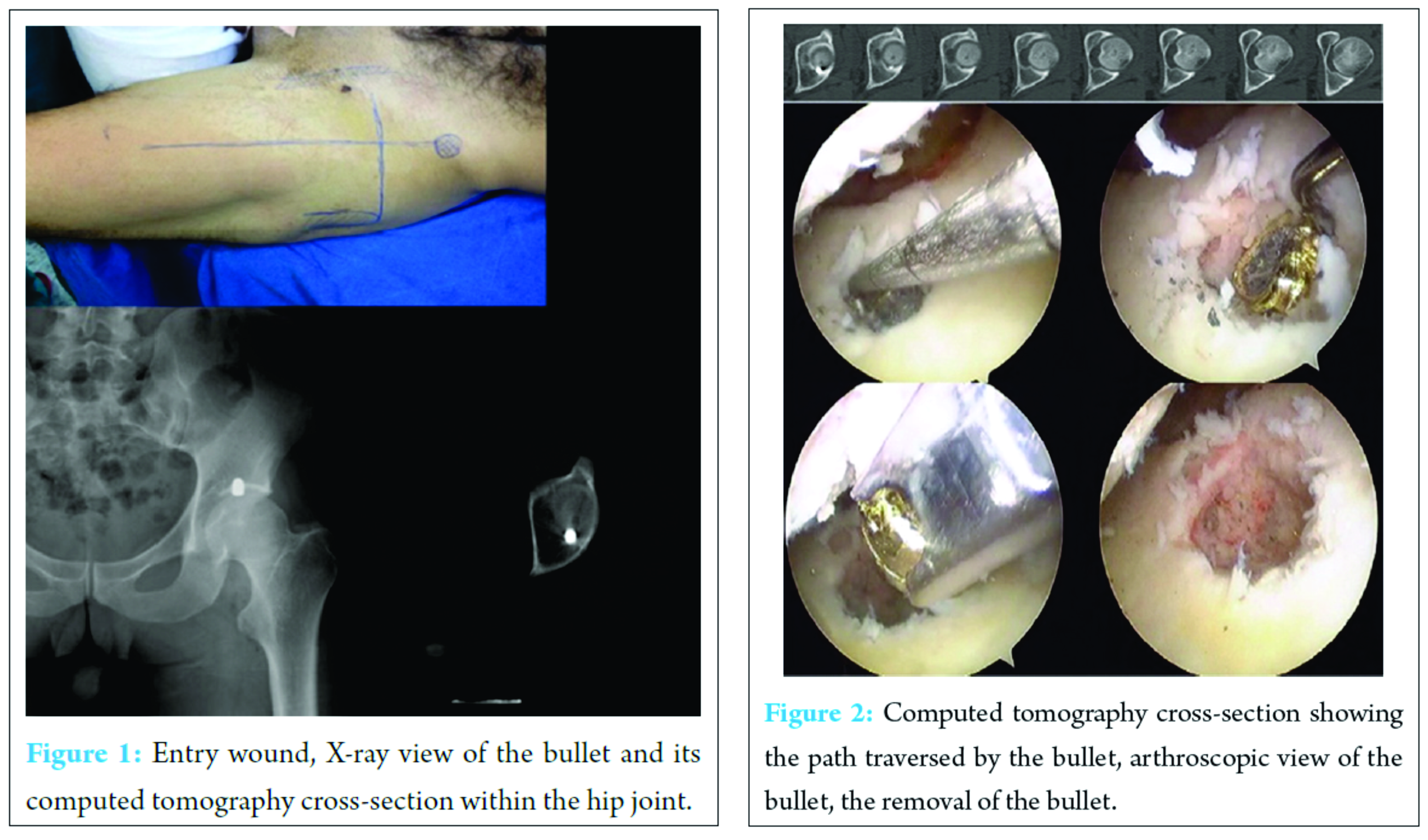
Following the debridement of the chondral damage occurred in the femoral and acetabular sides and the application of microfractures for the appropriate areas, the joint was washed out and the procedure was terminated. No complication was observed post-operatively. Limited mobilization with double crutches was permitted for six weeks. Then full weight bearing was initiated.
In second year of follow up period, patient appealed to hospital with groin pain. Patient had full range of motion but hip pain especially with weight bearing. Mr images were taken and the path traversed by the projectile through the femoral neck and 4×2 cm chondral defect on the femoral head were apparent (Fig. 3). No signs of osteoarthritis were detected.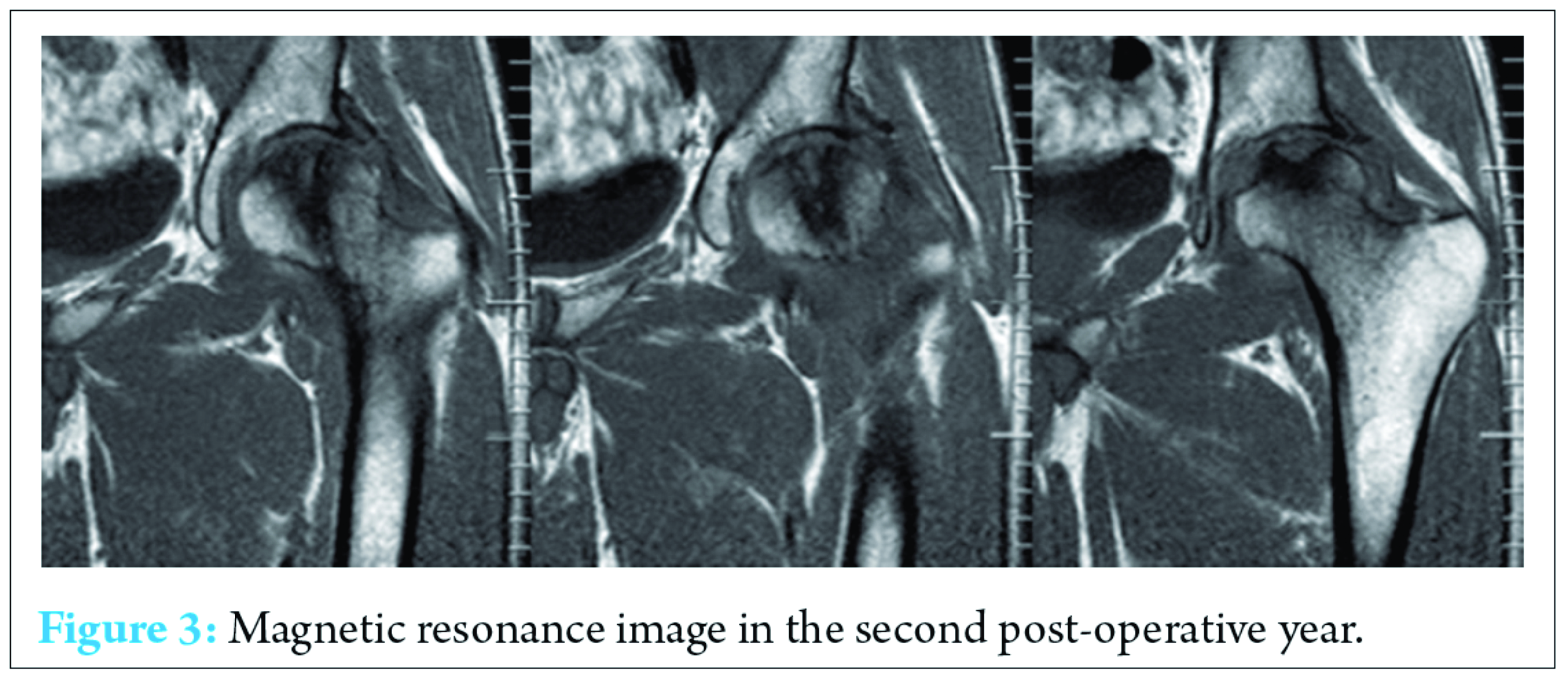
Patient was re-operated on March 2014. He was put on surgery table in lateral decubitis position with general anesthesia and safe surgical dislocation of the hip was applied (Fig. 4). Dissolved cartilage was removed and microfracture was applied to subchondral bone. Acellular collagen scaffold (marka model) was implanted on chondral defect area and fixed with fibrin glue (Fig. 5). No complication was observed post-operatively. Passive motions were allowed after two days and weight bearing was prohibited for six weeks.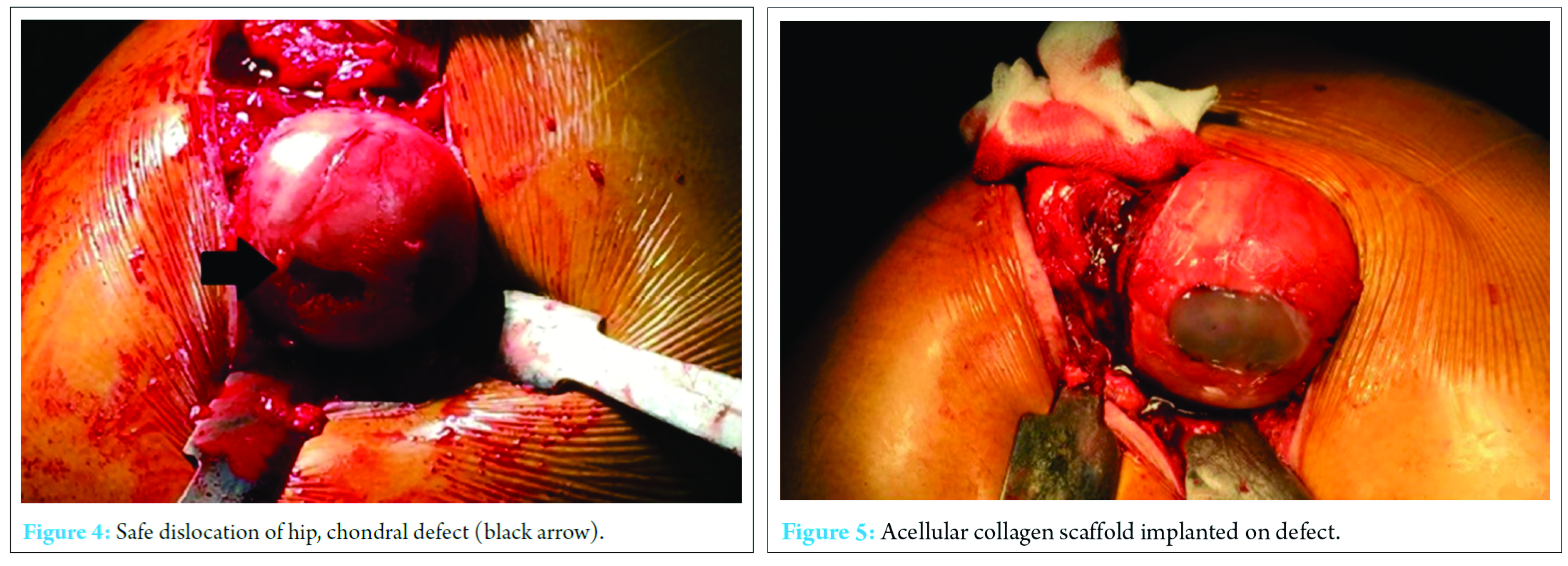
On May 2015, one year after second surgery, patient had full range of motion and no hip pain.
Discussion
Gunshot wounds to the hip joint account for 2% of all extremity gunshot wounds and 4% of lower-extremity gunshot wounds [4, 5]. Considering this frequency, it is a low possibility for the bullet to be imbedded in acetabulum, passing through the femoral neck. There is no report in literature reporting a projectile passing through femoral neck. It is a unique case and the pathway of the bullet is really interesting. To our knowledge, there are no published reports describing the arthroscopic removal of a bullet imbedded in acetabulum, passing through the femoral neck.
When left in the joint, the bullet may cause complications such as deep infection, lead intoxication, synovitis and traumatic arthritis in the long term [1, 2, 6]. Thus the projectile imbedded in the hip joint is required to be removed and the joint to be irrigated.
The location of the bullet needs to be determined with CT scanning in the pre-operative period and surgical operation should be planned accordingly. In the report by Delanay et al, they opted for safe surgical dislocation to retrieve a bullet from the femoral head since fragmentation at the femoral head was observed from CT image and the bullet was located posterior to the femoral head [2]. An experienced surgeon is able to access a satisfying view over the hip joint with arthroscopically assisted technique. Compared to arthrotomy, this technique which is less invasive allows the patient to return daily activities more rapidly [7]. In our case, having established the location of the projectile with the help of preoperative radiography and computed tomography we opted for hip arthroscopy.
Hip arthroscopy has recently become popular to treat many pathologies regarding the hip joint. Hip arthroscopy was first described by Burman in 1931 [8]. Arthroscopic technique for the extraction of the bullet from the hip joint was applied for a number of cases in the literature [9, 10, 11]. In the case report by Singleton et al, it was noted that a gunshot wound entered the abdomen, traversed the rectum and ended up in the weight-bearing dome of acetabulum, and the bullet was extracted with an arthroscopically assisted technique. They noted that this procedure can be performed safely, quickly and with minimal complications [3]. In our report, the bullet traversed the femoral neck before lodging in acetabulum. Cory et al reported on the arthroscopic removal of a .44 caliber bullet from the femoral head by using debridement of the articular surface [10]. In our case, debridement was required both on femoral head and acetabular side of the hip joint.
In contrast with arthrotomy, hip arthroscopy prevents blood loss, causes less osteonecrosis of femoral head and yields better cosmetic appearance with shorter rehabilitation time [4, 12]. However; infection was most expected complication in the cases reported in the literature since an accompanying abdomen wound existed. Osteonecrosis of the femoral head affected by the projectile and hip joint arthrosis were potential complications in our case. MR image, taken in the second postoperative year, chondral defect of the femoral head was observed. And an arthrotomy with safe surgical dislocation was needed for chondral defect treatment. After one year of arthrotomy, the patient had full range of motion and had no hip joint pain.
Conclusion
Arthroscopically assisted technique allows minimally invasive access to hip joint for the retrieval of foreign material lodged in, minimizing possible complications. Arthrotomy can be reserved to deal with further complications such as chondral problems as this case. We suggest using arthroscopical techniques for initial bullet removal; and open surgery may be reserved to handle further complications; as chondral injury like in this case. At the same time; we can conclude that acellular collagen scaffolds may be usefull for chondral injuries caused by bullets.
Clınıcal Message
It is suggested to remove foreign materials sucked into joint to prevent joint arthropathy, cartilage damage and septic arthritis. Arthroscopy is a proper procedure for removing foreign materials from hip joint. Open surgery may be reserved to handle with complications as chondral injury or osteoarthritis.
References
1. Windler EC, SMith RB, Bryan WJ, Woods GW. Lead intoxication and traumatic arthritis of the hip secondary to retained bullet fragments. A case report. J Bone Joint Surg Am. 1978 Mar;60(2):254-255.
2. Delaney R, Albright M, Rebello G. Utilization of the safe surgical dislocation approach of the hip to retrieve a bullet from the femoral head. Case Rep Orthop. 2011;
3. Singleton SB, Joshi A, Schwartz MA, Collinge CA.Arthroscopic bullet removal from the acetabulum. Arthroscopy. 2005 Mar;21(3):360-364.
4. Cory JW, Ruch DS. Arthroscopic removal of a .44 caliber bullet from the hip. Arthroscopy. 1998 Sep;14(6):624-626.
5. Bartlett CS, DiFelice GS, Buly RL, Quinn TJ, Green DS, Helfet DL. Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture. J Orthop Trauma. 1998;12:294-299
6. Rehman MA, Umer M, Sepah YJ, Wajid MA.Bullet-induced synovitis as a cause of secondary osteoarthritis of the hip joint: A case report and review of literature. J Med Case Rep. 2007 Dec 5;1:171.
7. Mineo RC, Gittins ME. Arthroscopic removal of a bullet embedded in the acetabulum. Arthroscopy.2003;19:E121-124.
8. Burman MS.Arthroscopy or the direct visualization of joints. J Bone Joint Surg. 1931;4:669-695.
9. Lee GH, Virkus WW, Kapotas JS. Arthroscopically assisted minimally invasive intraarticular bullet extraction: Technique, indications, and results. J Trauma. 2008;64:512-516.
10. Gupta RK, Aggarwal V. Indian. Late arthroscopic retrieval of a bullet from hip joint. J Orthop. 2009 Oct;43(4):416-419.
11. Teloken MA, Schmietd I, Tomlinson DP.Hip arthroscopy: A unique inferomedial approach to bullet removal. Arthroscopy 2002;18:E21.
12. Goldman A, Minkoff J, Price A, Krinick R A posterior arthroscopic approach to bullet extraction from the hip. J Trauma. 1987;27:1294-1300.
| How to Cite This Article: Çatma MF, Ünlü S, Ersan Ö, Öztürk A. Treatment of the Bullet, Traversing Femoral Neck, Lodged in Hip Joint: Initial Arthroscopic Removal and Subsequent Cartilage Repair. Journal of Orthopaedic Case Reports 2016 Sep-Oct;6(4): 13-16. . Available from: https://www.jocr.co.in/wp/2016/10/10/2250-0685-548-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


