
[box type=”bio”] What to Learn from this Article?[/box]
Interpositional arthroplasty is a very good treatment option for elbow mobility in young arthritic elbow proscribing the future total elbow arthroplasty.
Case Report | Volume 6 | Issue 4 | JOCR September-October 2016 | Page 49-52 | R Sivakumar, V SomaSheker, Prahalad Kumar Shingi, T Vinoth, M Chidambaram DOI: 10.13107/jocr.2250-0685.566
Authors: R Sivakumar[1], V SomaSheker[1], Prahalad Kumar Shingi[1], T Vinoth[1], M Chidambaram[1]
[1]Department of Orthopaedics, Preethi Institute of Orthopaedics and Research, Preethi Hospitals (Pvt) Limited, Madurai, Tamil Nadu, India.
Address of Correspondence
Dr. V Soma Sheker,
Consultant in Orthopaedics, Preethi Institute of Orthopaedics and Research, Preethi Hospitals (Pvt.) Limited, No. 27, Ganesh Nagar, 120 Feet
Road, Madurai – 625 007, Tamil Nadu, India.
E‑mail: somuortho@gmail.com
Abstract
Introduction: Elbow is a complex joint involving many articulations and complex biomechanics come into play. Elbow motion is crucial to upperlimb movement that loss of 50% of elbow function equals to loss of 80% of upper extremity global function. Restoring movement and stability is challenging to the surgeon while treating a stiff elbow. Unlike other arthroplasties of hip and knee, Total Elbow Arthroplasty may not be a primary treatment. Interpositional arthroplasty can be considered a viable option in post traumatic arthritis of elbow in young patients .
Case presentation: We report two cases of interpositional arthroplasties done in young patients secondary to post traumatic event. First case is 22 years old female with history of stiff elbow following a post traumatic event 3 years back and second case is 24 years old male labourer with stiff elbow following trauma more the 10 years back for which he took native treatment. In both the cases through posterior approach to the elbow we did osteoclysis and prepared fascia lata graft is interpositioned over the recreated articular surfaces. Both the patients in the follow up have good range of motion, stability and are satisfied. .
Conclusion: Interpositional arthroplasty( IPA) is good treatment option in young patients with post traumatic arthritis. Elbow instabilty, fascia rupture , thigh pain and hernia are the problems of IPA. Interpositional Arthroplasty to Total Elbow Arthroplasty transition is possible.
Keywords: Post Traumatic Arthritis, Interpositional Arthroplasty, Elbow Mobility, Fascial Resurfacing Arthroplasty.
Introduction
Elbow is a complex joint involving many articulations and complex biomechanics come into play. It has basically hinge joint between ulna and humerus with pivot articulations between radius and ulna[1]. Elbow has flexion range of 0 – 1450 and supination – pronation of 800 . Elbow motion is crucial to upperlimb motion that Loss of 50% of elbow function equals to loss of 80% of upper extremity global function (Sjöberg et al, 1996). So loss of motion due to trauma, inflammatory pathology or any other reason is not acceptable by the patients functional point of view. Restoring motion and stability is challenging to the surgeon while treating a stiff elbow.
Elbow Arthroplasty is an viable option secondarily in cases of failed fixation, bone loss in distal humerus fractures, stiff elbow and primarily in rheumatoid arthritis, ankylosis. Unlike other arthroplasties of hip and knee, it may not be considered as primary treatment in elbow. There are many arthroplasties like resection arthroplasty, interpositional arthroplasty (IPA) and total elbow arthroplasty(TEA) available with its own pros and cons [2].
Material And Methods
We report two cases of interpositional arthroplasty done in young patients with stiff elbow secondary to post traumatic event.
Case 1:
A 22 years old female came with history of stiff elbow following a post traumatic event 3 years back. She had taken native treatment with no benefit. On examination she found to have an elbow fixed at 900 with no movements (Figure 1). However supination and pronation were in near complete range. Considering the patient’s age, high functional demand and time related longetivity of total elbow arthroplasty , we planned for interpositional arthroplasty.
Surgical Consideration
After routine evaluation for surgery, with patient in lateral position (Figure 2) through posterior inverted V shaped Triceps reflecting approach the elbow joint was exposed [3]. Lateral collateral ligament was reflected from humeral attachment approaching the joint from lateral aspect. Ulno humeral joint was fused and arthritic changes seen over radial head. Joint was levered out with osteotome and osteoclysis completed (Figure 3) . The recreated articular surfaces were prepared with burr to give a smooth surface and near complete range of movement. Meanwhile through lateral incision over mid thigh, tensor fascia lata graft of 15 * 6 cm was harvested (Figure 4). The graft was folded on to itself and placed over the distal humeral surface. The graft was secured with vicryl through the drill holes made over the humerus (Figure 5) . Radial head was excised and lateral collateral ligament complex repaired. Intra operatively we obtained range of motion 150 to 1100 .wound closed in layers over drain . Post operatively elbow immobilised in 900 with a splint (Figure 6) .
The recreated articular surfaces were prepared with burr to give a smooth surface and near complete range of movement. Meanwhile through lateral incision over mid thigh, tensor fascia lata graft of 15 * 6 cm was harvested (Figure 4). The graft was folded on to itself and placed over the distal humeral surface. The graft was secured with vicryl through the drill holes made over the humerus (Figure 5) . Radial head was excised and lateral collateral ligament complex repaired. Intra operatively we obtained range of motion 150 to 1100 .wound closed in layers over drain . Post operatively elbow immobilised in 900 with a splint (Figure 6) .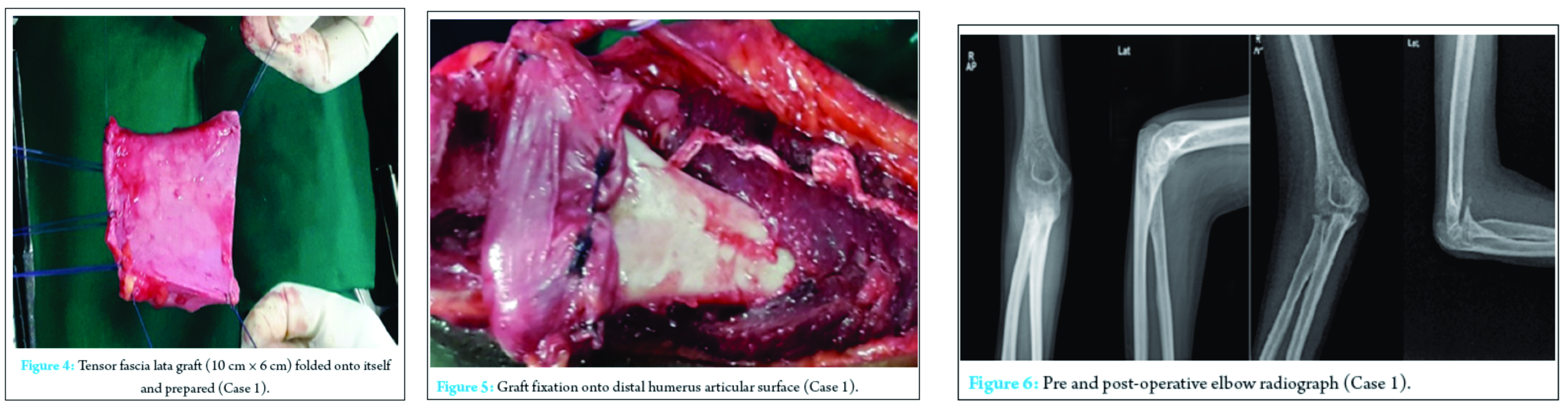
Splint was removed intermittently with elbow range of motion exercises advised upto pain tolerated by patient. Strengthening exercises were delayed. At the end of 24 weeks patient had elbow range of 300 – 1000 with good elbow stability. She is under rehabilitation with improving range of motion and Mayo Elbow Performance scores of 75 (Figure 7 and (Figure 8 ).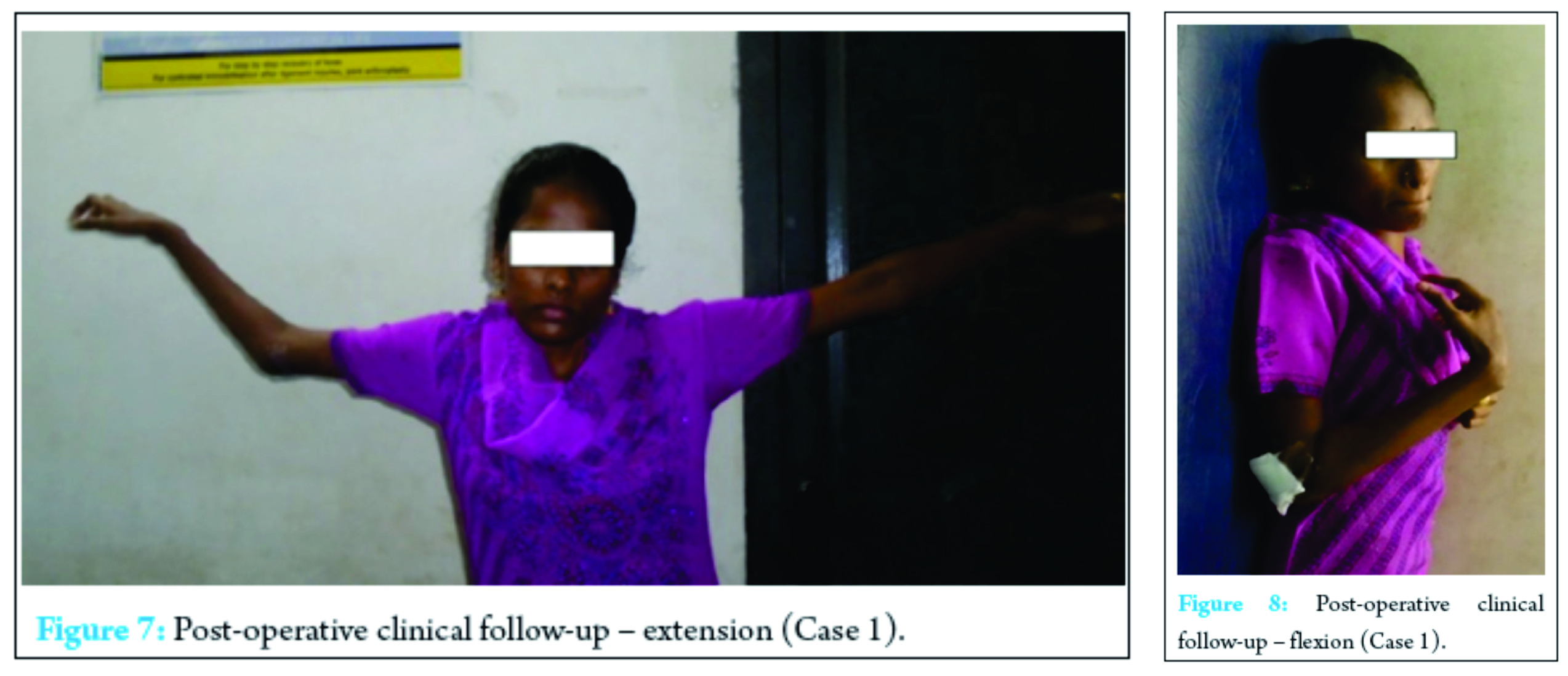
Case 2:
An 24 years old male Labourer came with complaints of stiff elbow. He gives history of trauma more the 10 years back for which he took native treatment. On examination elbow was fixed at 80 degrees of flexion with no further range of motion (Figure 9).. He under went interpositional arthroplasty similar to above procedure with preservation of radial head. Intra operatively we obtained range of motion 200 to 1100.At the end of 24 weeks patient has elbow flexion of 400 – 100 0 with reasonable stable elbow. He is under rehabilitation programme with Mayo Elbow Performance score of 65 (Figure 10).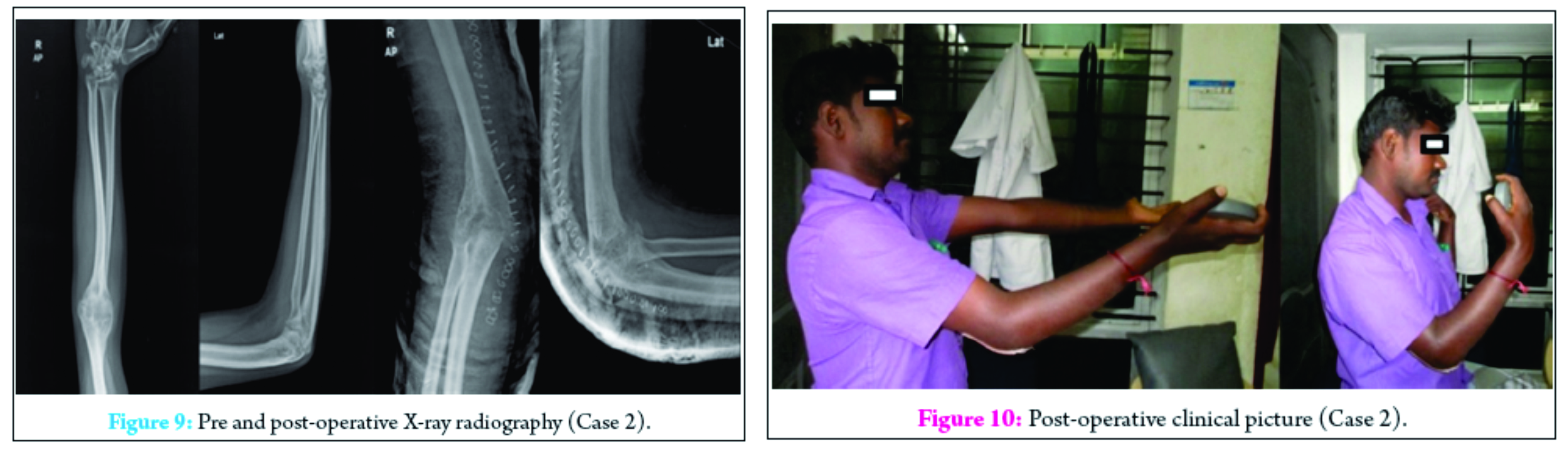
Discussion
Elbow arthroplasty is a relatively specialised procedure with few surgeons carrying out the operation frequently [4]. Prologue 1947, resection and interposition arthroplasty was the common surgical treatment for severe posttraumatic deformity, trauma, and rheumatoid arthritis[5]. Constrained, partial and total hinge arthroplasties were in vogue between 1947 to 1970 [5].
Interpositional arthroplasty is a type of resurfacing surgery which is viable option in young post traumatic stiff elbow with intact bony anatomy [6]. In their original study by S. L. Cheng et al [7] where they had a series of 13 patients who under went interpositional arthroplasty found 70 % patients had relief from pain. They concluded IPA is a useful option in young high demand patients with arthritis of elbow. Also it may not be useful in generalized inflammatory arthritis. However it has its own drawbacks of elbow instability, fascia rupture, thigh pain, neuropraxia.
There are instances where IPA can be a treatment option in post traumatic stiffness with osteomyelitis and loss of soft tissue cover. All three problems were treated in single stage by vancabeke [8]. Total elbow arthroplasty may be fascinating because of implant design and increased range of motion. However it has its limitations of longetivity , revision (22 %) for post traumatic arthritis in young patients [9] .
Arthrodesis may still be an alternative in the manual labourer or individual who can compensate for loss of movement. However arthrodesis is seldom now considered to be acceptable by high demanding young [10].
When the indications are correct in young patients interposition arthroplasty can relieve severe pain, affording a functional elbow with reasonable range of motion and bone stock is preserved [11]. Also the patient can be easily translated to semiconstrained total elbow arthroplasty who had prior interpositional arthroplasty [12]. One of our patients complained donor site related thigh pain.
In our patients in addition to interposition of fascia lata graft the lateral collateral complex of the elbow is repaired adequately and elbow is immobilised in appropriate position and time with intermittent exercise thereby bringing good stability to the joint, which is a major concern in previous studies. So interpositional arthroplasty serves as a buy back for future Total Elbow Arthroplasty.
Conclusion
• In our study both the patients achieved good range of motion and stability thereby patients had high satisfactory scores.
• Interpositional arthroplasty is good treatment option in young patients with post traumatic arthritis.
• Fascia rupture, thigh pain and hernia are the problems of IPA.
• Interpositional Arthroplasty to Total Elbow Arthroplasty transition is possible.
Clinical Message
Interpositional Arthroplasty is a very good treatment option for elbow mobility in young arthritic elbow proscribing the future Total Elbow Arthroplasty
References
1. Susan Standring PhD DSc Professor of Experimental Neurobiology and Head, Division of Anatomy, 598 – 599 , Gray’s Anatomy 39 edition, elsevier churchill livingstone 2008, ISBN:Main Edition 0 443 07168 3.
2. Thomas W Throckmorton et al 561-562, campbell’s operative orthopaedics, twelfth edition ISBN: 978-0-323-07243-4 , Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
3. Van Gorder GW. Surgical approach in supracondylar ‘T’ fractures of the humerus requiring open reduction. J Bone Joint Surg 1940;22: 278-92.,
4 . C. P. Little, A. J. Graham, A. J. Carr.Total elbow arthroplasty systematic review of the literature in the english language until the end of 2003, J Bone Joint Surg [Br] 2005;87-B:437-44.
5. Michael B. Cross, MD; Seth L. Sherman et al. The Evolution of Elbow Arthroplasty: Innovative Solutions to Complex Clinical Problems J Bone Joint Surg Am, 2010 Dec 01; 92 (Supplement 2): 98 -104 .
6. Froimson AI. Fascial interpositional Arthroplasty of the Elbow . In: Morrey B F. Master techniques in Orthopedic Surgery – The Elbow. Lippincott Williams and Wilkins . 1994 : 329-342.
7. S. L. Cheng, B. F. Morrey, Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty, vol. 82-b, no. 2, march 2000, J Bone Joint Surg [Br] 2000;82-B:233-8.
8. Vancabeke M, Lamraski G, Berthe JV, Coessens BC One-stage elbow interposition arthroplasty with a fasciocutaneous distally planned lateral arm flap. Acta Orthop Belg. 2002 Oct;68 (4) :392-5.
9. Celli A, Morrey BF. Total elbow arthroplasty in patients forty years of age or less. J Bone Joint Surg Am. 2009 Jun;91(6):1414-8.
10. Beckenbaugh RD. Arthrodesis. In: Morrey BF, ed. The elbow and its disordersThird ed. Philadelphia: W.B. Saunders Co., 2001:731-7.
11. Chen DD, Forsh DA, Hausman MR. Elbow Interposition Arthroplasty. Hand Clin. 2011 May;27(2):187-97.
12. Blaine TA, Adams R, Morrey BF. Total Elbow Arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am. 2005 Feb;87(2):286-92.
| How to Cite This Article: Sivakumar R, SomaSheker V, Shingi PK, Vinoth T, Chidambaram M. Treatment of Stiff Elbow in Young Patients with Interpositional Arthroplasty for Mobility: Case Series. Journal of Orthopaedic Case Reports 2016 Sep-Oct;6(4): 49-52. Available from: https://www.jocr.co.in/wp/2016/10/10/2250-0685-566-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


