
[box type=”bio”] What to Learn from this Article?[/box]
Risk factors and management of fracture diaphyseal femur following ipsilateral nonunion neck femur or resection arthroplasty of hip.
Case Report | Volume 6 | Issue 4 | JOCR September-October 2016 | Page 111-113 | Kunal Shah, Tushar Ubale, Rahematullah Abdul, Vaibhav Kasodekar, Ashish Assudani, Kiran Makwana DOI: 10.13107/jocr.2250-0685.598
Authors: Kunal Shah[1], Tushar Ubale[1], Rahematullah Abdul[1], Vaibhav Kasodekar[2], Ashish Assudani[1],Kiran Makwana[1]
[1]Department of Orthopaedics, R. N. Cooper Hospital, Mumbai, Maharashtra, India, 2Department of Orthopaedics, Sushrut Hospital, Mumbai, Maharashtra, India.
Address of Correspondence
Dr. Kunal Shah,
Department of Orthopaedics, R. N. Cooper Hospital, Mumbai, Maharashtra, India. Phone: +91‑9930731911.
E‑mail: orthokunal@yahoo.com
Abstract
Introduction: Although fracture diaphyseal femur is commonly seen in orthopaedic practice, its association with ipsilateral resection arthroplasty of hip/pseudoarthrosis of neck is rare. The technique of excision arthroplasty has undergone modification with emphasis on preserving as much bone as possible. However it is not always possible to preserve bone while removing the earlier prosthesis and cement. This often leads to extensive proximal bone loss. Associated ipsilateral fracture femur presents a unique scenario. Till date only one case report is published highlighting its surgical management.
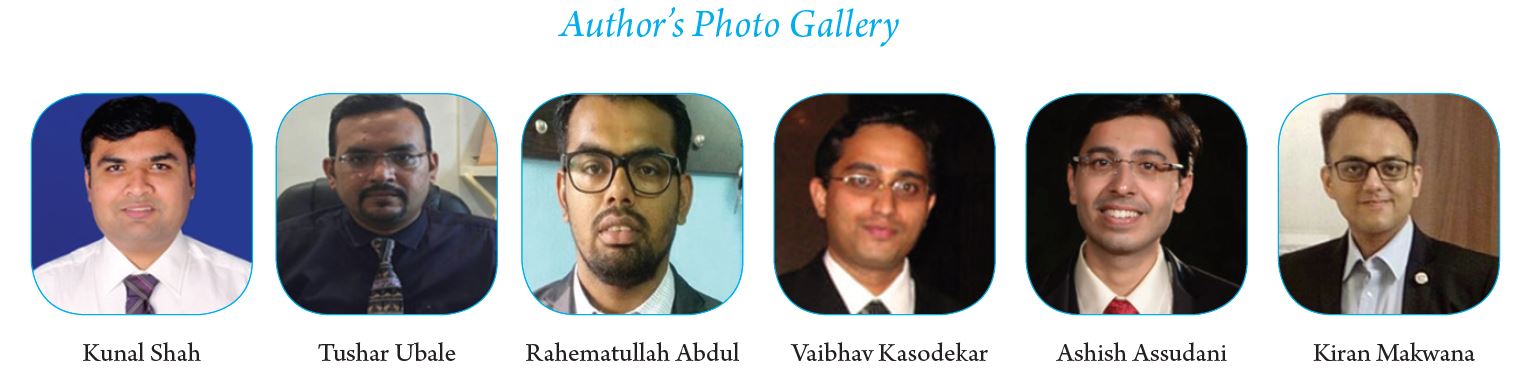
Case Presentation: We report two cases of diaphyseal fracture femur associated with resection arthroplasty of hip at sub trochanteric level with greater trochanter as separate fragment (case 1) and other with pseudoarthrosis of neck of femur with intact greater trochanter(case 2). First case was operated with surface fixation while second was operated with closed antegrade intramedullary nail.
Conclusion: Decision making and formulating treatment plan includes taking various factors into account like level of resection arthroplasty of hip/pseudoarthrosis of neck, status of greater trochanter (intact or separate fragment), osteoporosis and postoperative ambulation and rehabilitation. In this report we highlight the unusual occurrence, probable mechanism of injury, risk factors for fracture and decision making in surgical management of such a condition.
Key words: diaphysis fracture; resection arthroplasty; pseudoarthrosis; surface fixation; intramedullary nailing
Introduction
Fracture shaft femur is a commonly encountered injury in day to day practice. Orthopaedic surgeons are well versed with management of this type of injury. It usually occurs following road traffic accidents.Pathological femoral shaft fractures are mainly attributed to osteoporosis, pre-existing femoral pathology etc [1]. Uncommonly there can also be stress fractures of diaphysis of femur . Treatment includes intramedullary nailing or surface fixation depending on the age, aetiology of fracture,surgeon’s preference and clinical scenario [3] .
Resection arthroplasty of hip includes removal of necrotic bone in proximal femur along with the prosthesis and cement if present .Although uncommonly done nowadays itis described as a treatment option in cases of periprosthetic recalcitrant infection, septic sequelae,recurrent hip dislocation etc. [4]. Pseudoarthrosis of neck of femur is a common occurrence because of precarious blood supply to neck of femur, lack of cambium layer in periosteum, inadequate fixation,lack of anatomical reduction etc [9]. Resection arthroplasty of hip andpseudoarthrosis of neck presents as loss of proximal fulcrum for fracture diaphysis of femur to occur.
We present two cases with unique scenario of fracture diaphyseal femur concurrent with resection arthroplasty of hip/pseudoarthrosis neck of femur operated surgically. Till date only one similar case is reported of subtrochanteric fracture in femur postgirdlestone arthroplasty treated with intramedullary nail [6]. In this report we intend to highlight the unusual occurrence, probable mechanism of injury, risk factors and clinical decision making in surgical management of such a condition.
Case Report
Case 1: A 70-year-old lady came to trauma centre with pain and swelling in the left thigh .She gave history of slip and fall at home with thigh directly hitting the table. Radiographs of thigh suggested diaphyseal fracture left shaft femur with greater trochanter as separate fragment and ipsilateral excision arthroplasty of hip (Fig. 1a).There was no other associated injury and distal neurovascular examination was within normal limits. She had resection arthroplasty done in ipsilateral hip 15 years ago for an infected total hip replacement arthroplasty (cemented). Prior to fall she was walking full weight bearing with shoe raise and stick support. She did not have any co morbidities. There was no finding suggestive of pathological fracture other than osteoporosis. After optimising the patient she was offered surgery in the form surface fixation. She was operated in the form of open reduction internal fixation with locking compression plate (Fig. 1b).
Case 2: A 65-year-old lady presented with spiral proximal diaphyseal fracture following a trivial fall at home. Further radiographs suggested that she had pseudoarthrosis at neck of femur due to neglected fracture neck of femur (Fig. 2a). She was full weight bearing ambulating since last 10 years without any pain. However she used shoe raise and stick while walking. There were no comorbidities. After adequate preoperative work up and planning, she was operated with closed intramedullary nailing (Fig. 2b).
Postoperative protocol
After surgery both patients were mobilised non weight bearing for 6 weeks followed by gradual weight bearing walking. Knee range of motion exercises and quadriceps strengthening was started in immediate postoperative phase. At 3 months radiograph showed good callus formation and full weight bearing walking was started (Fig. 2c). Presently at one year follow up both patients are full weight bearing walking with a stick support and full range of motion of knee. Limb length discrepancy was same as before surgery.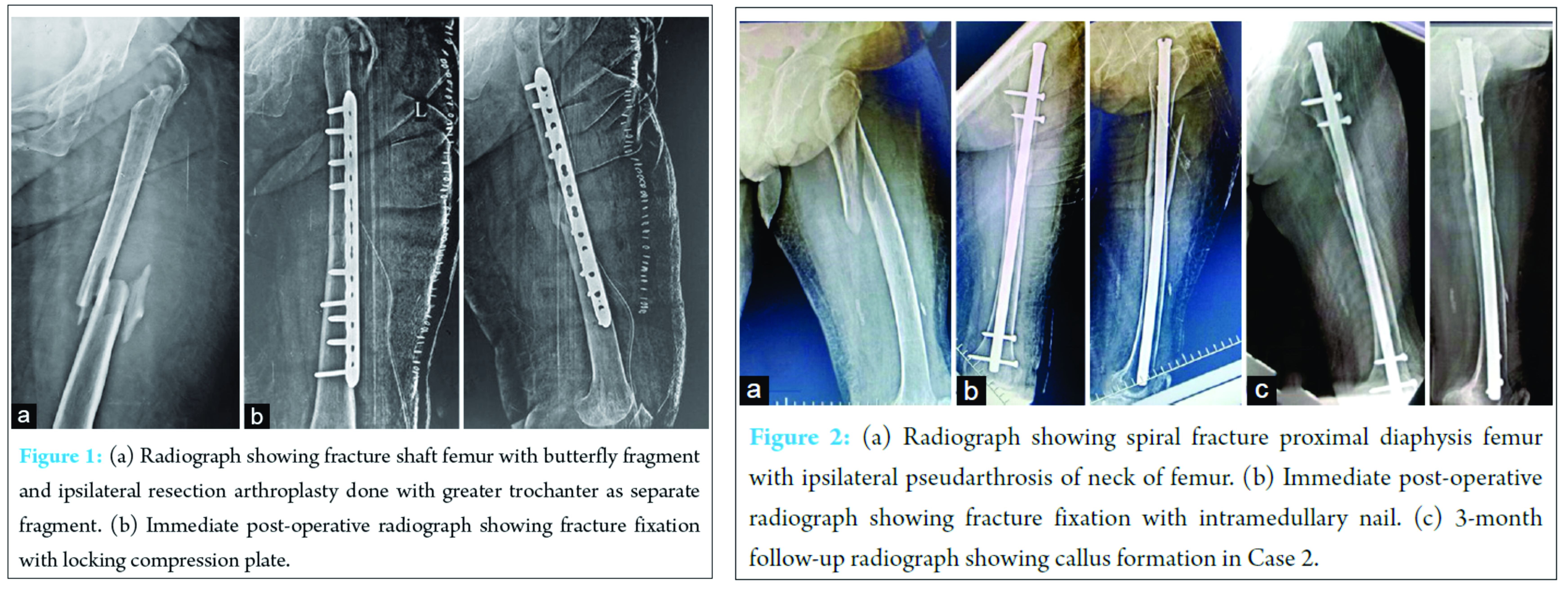
Discussion
The mechanism of injury in case of femoral diaphyseal fractures is usually due to direct blow to femoral shaft. Femur like other bones gives away in tension, depending on the direction of force. Elderly patients typically present with spiral fracture due to torsional forces, whereas axial and bending forces act on young patients to produce fractures [7]. In case 1 since there was a resection arthroplasty of hip done and in case 2 there was pseudoarthrosis at neck of femur suggesting loss of fulcrum proximally for axial, bending or torsional forces to act and produce fractures.Therefore biomechanically there was less chances of fracture. We feel that probable mechanism in case1 was direct blow to femur due to fall and in case 2 was twisting injury due to fall. The long standing fibrosis would have provided enough leverage for torsional forces to act and produce spiral fracture in pathologically weak bone. Moreover the femur bone appeared to be weakened due to senile osteoporosis and previous attempt of cement removal during resection arthroplasty (case 1). Dunn et al cited similar risk factors of weakening of bone forsubtrochanteric fracture in their case [6].
The goal of resection arthroplasty is to create stable pseudoarthritis site with eradication of infection and pain. Resection arthroplasty of hip leads to instability, limb length discrepancy, abductor weakness etc. Majority of patients require some form of ambulation assistance[8]. The technique of girdlestone arthroplasty has undergone modification with emphasis on preserving as much bone as possible [4, 9]. However it is not always possible to preserve bone while removing the earlier prosthesis and cement.Incase 1 resection arthroplasty lead to severe bone loss with excision of proximal end of femur uptosubtrochanteric level.
Management of this unique case scenario posed several challenges. Clinical decision making in formulating treatment plan included taking various factors into account like presence of resection arthroplasty of hip at subtrochanteric level with greater trochanter as a separate fragment (case 1), pseudoarthrosis at neck of femur with intact greater trochanter (case 2) osteoporosis and postoperative ambulation and rehabilitation. As in case 1 the greater trochanter was not intact, so we did not choose an intramedullary interlocking nail. Also there was a concern about disturbing a stable pseudoarthrosis site while doing intramedullary nailing. In case described by Dunn et al, the greater trochanter was intact and they performed open intramedullary nailing. However they cited several problems like getting a closed reduction due to lack of adequate traction and difficulties in reaming the canal [6]. Retrograde femoral nailing could have been an option in such cases if intramedullary device is preferred and greater trochanter is shattered. However this method would also pose problems with traction and getting closed reduction. Also there was concern about opening the knee joint which is already arthritic in old age. For these reasons we chose plate fixation as a modality of fracture fixation. As the fixation was stable and proximal pseudoarthrosis site was not disturbed, we could start early joint mobilisation and subsequently patient returned to preoperative ambulatory status. In case 2 since the greater trochanter was intact we preferred intramedullary fixation. There were difficulties with traction and getting a closed reduction .However the main advantage was that biology of fracture was preserved due to closed technique which aids in union.
Conclusion
Thus we conclude that ipsilateral diaphyseal femur fracture with resection arthroplasty/pseudoarthrosis is a rare case scenario. Risk factors leading to such a complication should be borne in mind. The case requires careful consideration and analysis of various factors in formulating the plan of management.
Clinical message
Fracture diaphyseal femur can occur after following nonunion neck femur or resection arthroplasty of hip. Risk factors leading to this should be understood and analyzed. Meticulous planning taking various factors into account should be done.
References
1. Lenart BA, Neviaser AS, Lyman S, Chang CC, Edobor-Osula F, Steele B, van derMeulen MC, Lorich DG, Lane JM. Association of low-energy femoral fractures withprolonged bisphosphonate use: a case control study. Osteoporos Int. 2009Aug;20(8):1353-62.
2. Boden BP, Speer KP. Femoral stress fractures.Clin Sports Med. 1997Apr;16(2):307-17.
3. Beaty JH. Operative treatment of femoral shaft fractures in children andadolescents. ClinOrthopRelat Res. 2005 May;(434):114-22.
4. Hudec T, Jahoda D, Sosna A. [Resection hip arthroplasty–mid- and long-termresults]. ActaChirOrthopTraumatolCech. 2005;72(5):287-92.
5. Marti R, Raaymakers EL, Nolte P, Besselaar PP. [Pseudarthrosis of the proximalfemur]. Orthopade. 1996 Sep;25(5):454-62.
6. Dunn J, Scully WF, Crawford DA, Manoso MW. Ipsilateral diaphyseal femurfracture after resection arthroplasty.J Arthroplasty. 2012 Sep;27(8):1580.e17-9.
7. Tencer AF, Kaufman R, Ryan K, Grossman DC, Henley BM, Mann F, Mock C, RivaraF, Wang S, Augenstein J, Hoyt D, Eastman B; Crash Injury Research and EngineeringNetwork (CIREN). Femur fractures in relatively low speed frontal crashes: thepossible role of muscle forces. Accid Anal Prev. 2002 Jan;34(1):1-11.
8. Sharma H, De Leeuw J, Rowley DI. Girdlestone resection arthroplasty following failed surgical procedures. IntOrthop. 2005 Apr;29(2):92-5.
9. Esenwein SA, Robert K, Kollig E, Ambacher T, Kutscha-Lissberg F, Muhr G.[Long-term results after resection arthroplasty according to Girdlestone fortreatment of persisting infections of the hip joint]. Chirurg. 2001Nov;72(11):1336-43.
| How to Cite This Article: Shah K, Ubale T, Abdul R, Kasodekar V, Assudani A, Makwana K. Fracture Diaphyseal Femur in a Case of Ipsilateral Excision Arthroplasty of Hip: Report of Two Cases with Description of an Unusual Injury Pattern, Mechanism, and Clinical Decision-making in Management. Journal of Orthopaedic Case Reports 2016 Sep-Oct;6(4): 111-113.. Available from: https://www.jocr.co.in/wp/2016/10/10/2250-0685-598-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


