
[box type=”bio”] What to Learn from this Article?[/box]
GCT of metatarsal is quite a rare entity which can be managed with local resection of metatarsal followed by autograft replacement.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 3-6 | Kumar Prashant, Tulsi Das Bhattacharyya, Herman Frank, Prema Ram. DOI: 10.13107/jocr.2250-0685.604
Authors: Kumar Prashant[1], Tulsi Das Bhattacharyya[2], Herman Frank[2], Prema Ram[3]
[1]Department of Orthopaedics, Trauma Centre, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India,
[2]Department of Orthopaedics, Gauhati Medical College & Hospital, Guwahati, Assam, India, 3Department of Orthopaedics, Jeevan Jyoti Hospital,
Pali, Rajasthan, India.
Address of Correspondence
Dr. Kumar Prashant
Department of Orthopaedics, Plot No. 120, Ashokpuram Colony, Dafi, Varanasi – 221 011, Uttar Pradesh, India.
E-mail: dr.kumarprashant83@gmail.com
Abstract
Introduction: Giant cell tumor (GCT) or osteoclastoma is an osteolytic, mostly benign but locally aggressive tumor occurring in young adults at the epiphysis. Area of predilection is mainly long bones (85-90%). 4% of GCT are also found in iliac bone, spine and only 2% in hand (of which GCT phalanges are more common than metacarpal). GCT of metatarsal is a very rare occurrence with very few cases being reported so far. We report a case of GCT 1st metatarsal in a 40-year-old male which is a very rare entity. We shall discuss the clinical features, pathological and radiological hallmarks, and the various treatment modalities of such lesion.
Case Report: A 40-year-old male presented with complain of swelling over the dorsum of left foot for the duration of 2 years and pain in that foot for 4 months. Swelling was insidious in onset and has progressively increased in size. Pain was mild to moderate in intensity, dull aching and continuous. On examination, there was a localized ovoid shaped swelling 7 by 4 cm over the dorsum of the left foot opposing 1st and 2nd metatarsal area with well-defined margins, tender on deep palpation, hard in consistency and the overlying skin was free. Radiographs revealed an expansile osteolytic lesion of entire 1st metatarsal involving the articular surface of tarsometatarsal joint and metatarsophalangeal joint with impingement on 1st metatarsal and cortical thinning. The classical “soap bubble appearance” was also present. Fine needle aspiration cytology was done to confirm our diagnosis of GCT. According to Campanacci et al., the tumor was histologically graded as Grade II tumor. A reconstructive surgery with fusion of the Cuneiform metatarsa and metatarsophalangeal joint was planned. The tumor was carefully removed with a cuff of normal tissue and the proximal and distal joints were inspected. There was no articular cartilage of the Cuneiform metatarsa joint. A fibular graft was taken and was inserted into the troughs created in medial cuineform and proximal phalanx and fixed with K-wire, both proximally and distally. The patient was given a below knee cast for three months postoperatively. Full weight bearing was started after 3 months. After 9 months of follow-up, the graft was well taken up and there were no signs of recurrence both clinically and radiologically.
Introduction
Giant cell tumor (GCT) of bone is a benign, aggressive tumor with features of frequent local recurrences and the potential for the metastasis and the malignant transformation. It usually occurs in young adult of 16-35 years in the physical region. The male to female ratio is 3:5. Nearly, 85-90% are found in long bones, of which 50% occur in the region of knee. Other frequent sites are distal radius, proximal humerus, and fibula. 4% occur in pelvic bone and spine. Involvement of small bones of hand and foot is very rare. Unni has reported an incidence of 2% in the hand and 1.5% in the foot (phalanges being more involved than metacarpals and metatarsals). We are presenting a case of GCT of 1st metatarsal of left foot which is a very rare site for such tumors.
Case Report
A 40-year-old male presented to us with the chief complaints of swelling over the dorsum of left foot for the duration of 2 years and pain in that foot for 4 months. Swelling was insidious in onset and has progressively increased in size. Pain was mild to moderate in intensity, dull aching and continuous. It was relieved by taking medication and rest and aggravated by activity. There is no history of any constitutional symptoms or trauma.
On physical examination, there was a localized ovoid shaped swelling 7 by 4 cm over the dorsum of the left foot opposing 1st and 2nd metatarsal area with well-defined margins. Swelling was tender on deep palpation, hard in consistency, and the overlying skin was free.
Radiographs revealed an expansile osteolytic lesion of entire 1st metatarsal involving the articular surface of tarsometatarsal joint and metatarsophalangeal joint with impingement on 1st metatarsal and cortical thinning. The classical ‘soap bubble appearance’ was also present (Fig. 1). Fine needle aspiration cytology was done to confirm our diagnosis of GCT. According to Campanacci et al., the tumor was histologically graded as Grade II tumor (Fig. 2).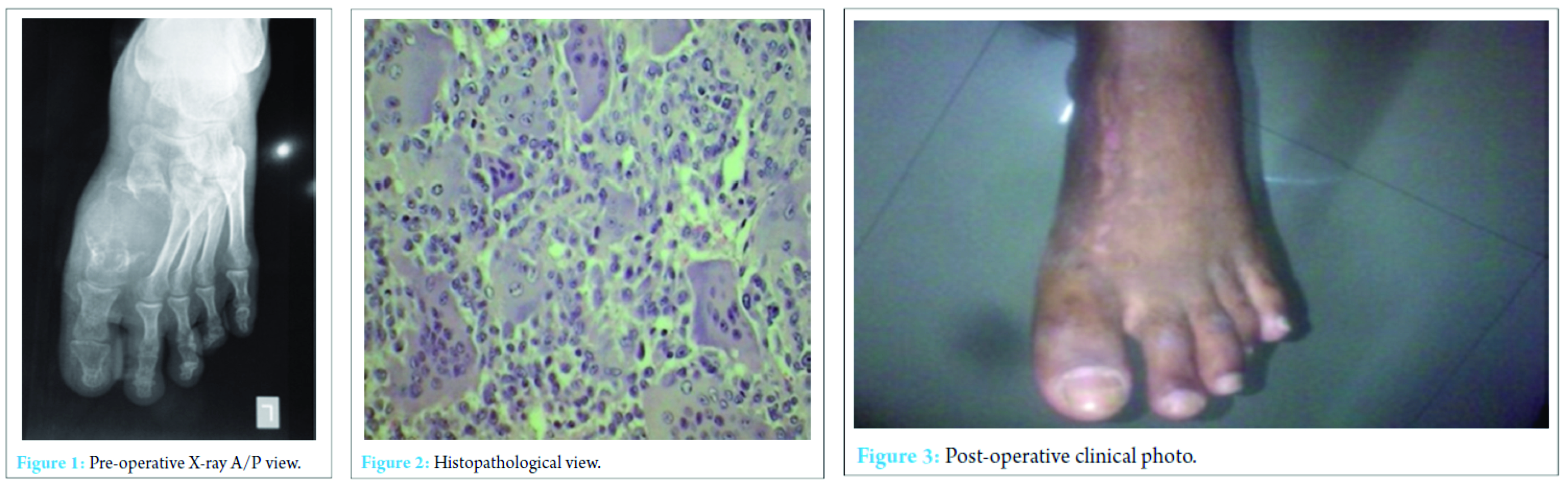
A reconstructive surgery with fusion of the Cuneiform metatarsal and metatarsophalangeal joint was planned. The tumor was carefully removed with a cuff of normal tissue and the proximal and distal joints were inspected. There was no articular cartilage of the Cuneiform metatarsa joint. A fibular graft was taken and was inserted into the troughs created in medial cuineform and proximal phalanx and fixed with K-wire, both proximally and distally (Fig. 3 and 4) [10].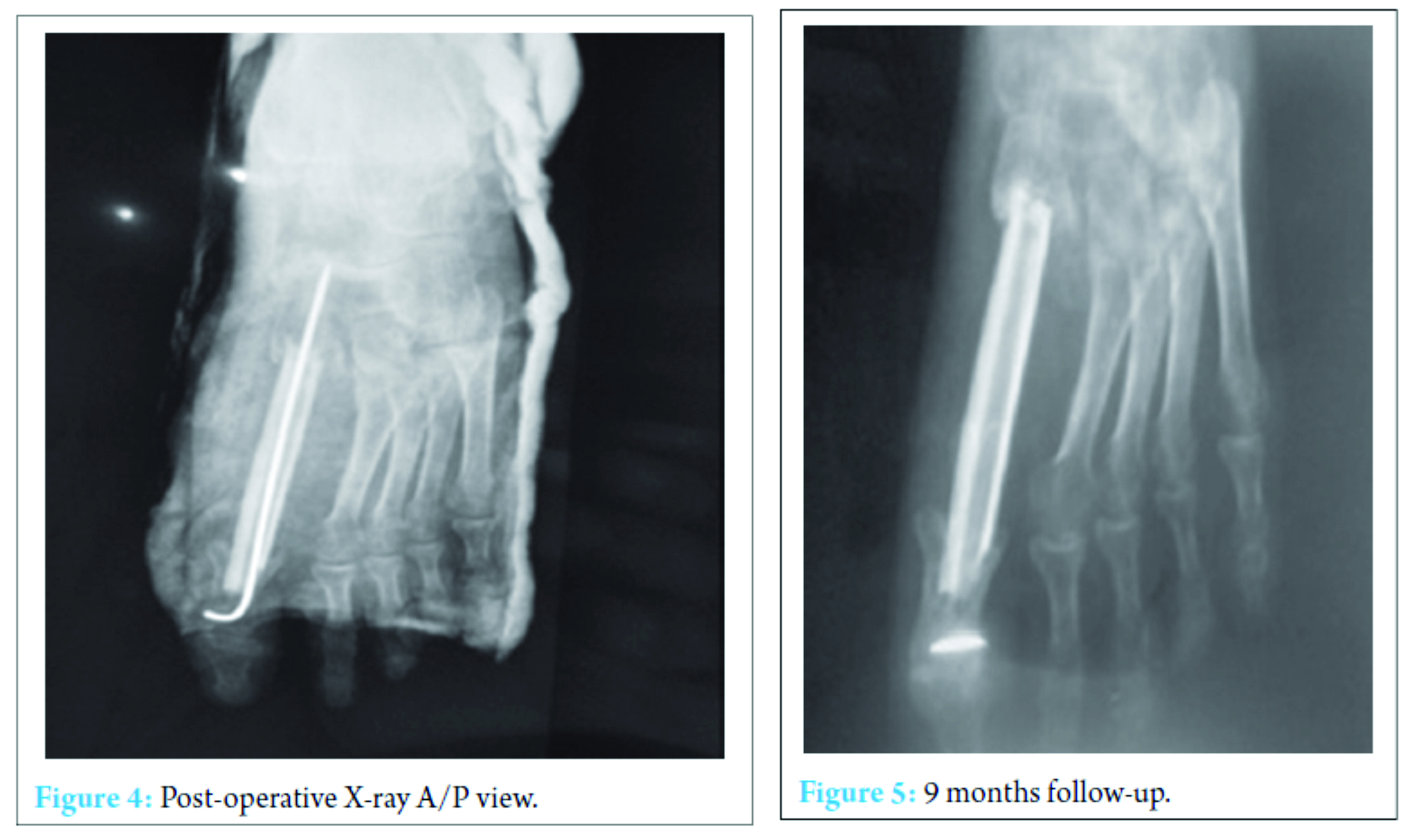 The patient was given a below knee cast for three months postoperatively. Full weight bearing was started after 3 months. After 9 months of follow-up, the graft was well taken up and there were no signs of recurrence both clinically and radiologically (Fig. 5).
The patient was given a below knee cast for three months postoperatively. Full weight bearing was started after 3 months. After 9 months of follow-up, the graft was well taken up and there were no signs of recurrence both clinically and radiologically (Fig. 5).
Discussion
GCT of the bone is benign, but locally aggressive lesion. It is a relatively rare tumor composed of connective tissue stromal cells having the capacity to recruit and interact with multinucleated giant cells that exhibit the phenotypic features of osteoclasts [1].
GCT predominates in the long bones (75-90% of cases) especially the femur (approximately 30% cases), tibia (25% cases), radius (10% cases), and humerus (6% cases) [1, 2, 3, 4]. The spine and innominate bone are involved occasionally. GCT of the bones of the hand are rare, accounting for only 2% of cases and here too phalangeal location of the tumor is more common than metacarpals. GCT of foot is even rarer than GCT of hand. GCT of the hand and foot seems to represent a different lesion than conventional GCT in the rest of the skeleton [1, 6, 9]. There is an 18% incidence of multicentric foci [7] indicating that a bone scan should be a part of routine workup of these tumors. Overall they appear in a younger age group [8]. They also have a shorter duration of symptoms averaging 6 months or less before a diagnosis is made [5, 9].
Furthermore, differential considerations based on the appearance and location of this tumor included GCT, giant cell reparative granuloma, aneurysmal bone cyst, chondromyxoid fibroma, brown tumor of hyperparathyroidism, angiosarcoma, myeloma, and an expansile metastatic lesion, such as renal cell carcinoma must be taken into consideration. Despite the fact that the GCT is not a sarcoma, the extent of tumor at the time of diagnosis and the high recurrence rate following limited resection often dictate the need of an en bloc resection through normal tissues to prevent local recurrence of the lesion. Such a treatment creates a significant skeletal defect and a challenging reconstructive problem. Reconstruction of the foot after en bloc excision is particularly difficult because of the need to restore the joint surface as well as the bone. The fibula has been used for reconstruction since it matches the anatomy of the foot which is a weight bearing structure.
The various treatment modalities described in literature are curettage, curettage and bone grafting, irradiation, amputation, and resection with reconstruction.
Conclusion
GCT or osteoclastoma is an osteolytic, mostly benign but locally aggressive tumor occurring in young adults at the epiphysis. Area of predilection is mainly long bones (85-90%). 4% of GCT are also found in iliac bone, spine and only 2% in hand (of which GCT phalanges are more common than metacarpal). Local resection of the involved metatarsal with autograft or allograft replacement is the preferred surgical treatment for several reasons. First, no correlation has been found between the grade of GCT and the rate of recurrence. Therefore, all giant tumors of foot should be considered locally aggressive. In addition, curettage with or without bone grafts has resulted in recurrence rates of about 90%. Thus curettage is an unacceptable form of treatment. Second, although amputation may prevent recurrence, it is cosmetically deforming and decreases the function of the foot.
Clinical Message
All giant tumors of foot should be considered locally aggressive. In addition, curettage with or without bone grafts has resulted in recurrence rates of about 90%. Thus curettage is an unacceptable form of treatment. Second, although amputation may prevent recurrence, it is cosmetically deforming and decreases the function of the foot.
References
1. Saikia KC, Bhuyan SK, Borgohain M, Saikia SP, Bora A, Ahmed FJ. Giant cell tumour of bone: An analysis of 139 Indian patients. J Orthop Sci 2011;16(5):581-588.
2. Goldenberg RR, Campbell CJ, Bonfiglio M. Giant cell tumor of bone. An analysis of 218 cases. J Bone Joint Surg Am 1970;52(4):619-664.
3. Murphey MD, Nomikos GC, Flemming DJ, Gannon FH, Temple HT, Kransdorf MJ. From the archives of AFIP. Imaging of giant cell tumor and giant cell reparative granuloma of bone: radiologic-pathologic correlation. Radiographics 2001;21(5):1283-1309.
4. Dahlin DC, Cupps RE, Johnson EW Jr. Giant-cell tumor: A study of 195 cases. Cancer 1970;25(5):1061-1070.
5. Cavender RK, Sale WG 3rd. Giant cell tumor of the small bones of the hand and feet: Metatarsal giant cell tumor. W V Med J 1992;88(8):342-345.
6. Wold LE, Swee RG. Giant cell tumor of the small bones of the hands and feet. Semin Diagn Pathol 1984;1(3):173-184.
7. Cummins CA, Scarborough MT, Enneking WF. Multicentric giant cell tumor of bone. Clin Orthop Relat Res 1996;322:245-252.
8. Khanna AK, Sharma SV, Kumar M. A large metatarsal giant-cell tumor. Acta Orthop Scand 1990;61(3):271-272.
9. Mohan V, Gupta SK, Sharma OP, Varma DN. Giant cell tumor of short tubular bones of the hands and feet. Indian J Radiol 1980;34:1-17.
10. Mendicino SS. Giant cell tumor of the first metatarsal bone en bloc resection with autogenous middle fibular strut graft. J Foot Ankle Surg 1993;32(4):405-410.
| How to Cite This Article: Prashant K, Bhattacharyya TD, Frank H, Ram P. An Unusual Case of Giant Cell Tumor of First Metatarsal: A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):3-6. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-604-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


