
[box type=”bio”] What to Learn from this Article?[/box]
Snapping scapula is a syndrome of variable etiology and it is important to differentiate between idiopathic and anatomical causes as conservative treatment is less likely to be successful if a clear anatomical cause can be found.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 96-99 | Raja Rameez, Mehmood Ul-Hassan, Hilal A Kotwal, Khursheed A H Kangoo, Asif Nazir DOI: 10.13107/jocr.2250-0685.652
Authors: Raja Rameez[1], Mehmood Ul-Hassan[1], Hilal A Kotwal[1], Khursheed A H Kangoo[1], Asif Nazir[1]
[1]Department of Orthopaedics, Government Medical College Srinagar, Jammu and Kashmir, Himachal Pradesh, India.
Address of Correspondence
Dr. Raja Rameez,
Department of Orthopaedics, PG Hostel, Bone and Joint Hospital, Barzullah, Srinagar, Jammu and Kashmir, Himachal Pradesh, India.
E-mail: rajaramulf@gmail.com
Abstract
Introduction: Osteochondroma or exostosis is most common benign bone tumors. They are usually seen in the metaphyses of long bones with more than 35% of cases affecting the bone around the knee and are seldom found in flat bones like scapula. When present in scapula, they may cause abnormal scapulothoracic movements leading to pain, snapping, and pseudowinging of scapula.
Case report: We describe a novel case of osteochondroma arising on the ventral aspect of right scapula in a 16-year-old otherwise healthy female patient causing snapping and pseudowinging of scapula and occasional pain in affected area. X-ray and computed tomography findings were consistent with an abnormal bony mass arising on ventral aspect of superior border of the scapula. The patient was treated with open extraperiosteal resection of the mass with relief of symptoms. The histopathological diagnosis was consistent with osteochondroma with no signs of malignancy.
Conclusion: In a patient with winging and snapping of scapula one should be aware of rare diagnosis osteochondroma along with other more common etiology.
Keywords: Osteochondroma, scapula, snapping scapula, pseudowinging.
Introduction
Osteochondromas constitute 10-15% of all bone tumors and 30-50% of benign bone tumors, representing the most common benign bone tumors [1, 2, 3]. They are usually solitary tumors (90%) but can be multiple in hereditary exostoses (10%). Although considered as a tumor, an osteochondroma is actually a developmental physeal growth defect and usually occurs in the metaphysis of long bones such as femur, humerus, and tibia. It is unusual in flat bones such as scapula [4, 5, 6, 7], seen only in 4% cases [8]. However, this is the most common benign primary bone tumor affecting scapula. Although usually presents as an asymptomatic slowly-growing mass, a scapular osteochondroma may be symptomatic mainly due to its mass effect. In addition, It may produce symptoms as a result of overlying bursa [1, 2, 8 ,9], soft tissue impingement [10], a fracture of the stalk [11], a vascular injury [12, 13], a neurological injury [14], and malignant transformation. The classic etiology of winging of scapula is serratus anterior muscle impairment secondary to long thoracic nerve palsy [15, 16, 17]. However, bone, muscle, various nerve and shoulder joint pathology may be associated with winging of scapula. Snapping scapula is an uncommon disorder resulting from derangement of the scapula-costal mechanism. The etiology is usually idiopathic. However, an anatomical cause such as osteochondroma, especially if it arises on the ventral aspect, may lead to snapping scapula; in such cases, excision of the tumor is required to obtain normal scapulothoracic motion [18]. Ventral osteochondroma may produce mechanical problems due to mass effects also [16, 19, 20]. An exostosis over the ventral surface of the scapula has been reported to have locked with the chest wall preventing scapulothoracic motion [21]. There are only few reports of osteochondroma on the superomedial angle of the ventral surface of the scapula [5, 22, 23, 24, 25]. This report describes a case with a large scapular osteochondroma causing pseudowinging and snapping scapula syndrome and treated with excision.
Case Report
A 16-year-old right-hand dominant female presented to our orthopedic department with tolerable pain in upper back associated with “clunking” during active movements of right shoulder. The parents also had noticed an abnormal prominence in the right scapular region. She developed gradual symptoms over a 6 month period before her presentation with no antecedent history of trauma and constitutional symptoms. Other siblings and parents were normal.
Physical examination revealed a nontender palpable mass at superior border near medial angle of scapula. A grating sensation, both palpable and audible, was produced during active shoulder range of motion. Vertebral border of right scapula was more prominent than left (Fig. 1a). The winging of scapula was noticed even at rest which did not increase as the patient did push against the wall. There were no signs of infection or inflammation. A bony mass was felt over the superomedial angle of the right scapula, which was minimally tender and corresponded to the area from where the crepitus arose. The upper extremity and shoulder girdle muscles were neurologically intact. Laboratory investigations were within normal limits.
Radiographs showed a large bony tumor arising from superior border close to angulus superior scapulae and directed toward the thorax (Fig. 1b). Computed tomography scan images revealed a pedunculated bony mass measuring 5.3×3.0×1.5 cm attached to ventral surface of superior border of scapula by a small stalk (Fig. 2a-c). Magnetic resonance imaging revealed this mass was extending anteriorly against the ribs and had a characteristic mushroom-shaped appearance with no obvious soft tissue component. A diagnosis of ventral scapular exostosis is made and patient was offered for surgical treatment in view of her complaints and cosmetic concern. Wide, open excision is the treatment of choice; however, there are recent reports of arthroscopic excision [2, 6, 5, 21, 20].
The patient was treated with excision of osteochondroma in prone position under general anesthesia. The shoulder was held in internal rotation thus facilitating lifting of medial border of scapula. A longitudinal incision along the medial border of scapula was used. Trapezius muscle was incised in line with its fibers (Fig. 3a). Levator scapulae and rhomboid minor muscles were detached. No bursa was demonstrated and we encountered no technical difficulties during surgery. Extraperiosteal resection of the swelling was done and sent for biopsy (Fig. 3b). Histopathological examination confirmed the mass to be an osteochondroma (Fig. 3c). a. No malignant transformation was noticed in the cartilaginous cap. Post-operative clinical examination showed painless full shoulder mobility as well as the absence of scapular winging and crepitus. Radiograph confirmed complete removal of the tumor. The arm was immobilized in a sling for 4 weeks during which period only pendulum exercises were permitted. After 4 weeks, she was sent for a rehabilitation program to improve her shoulder range of movements. Her symptoms resolved dramatically in the immediate post-operative period and she felt no abnormal movements of the shoulder at 6 weeks follow-up. There is no recurrence of symptoms till last follow-up at 6 months.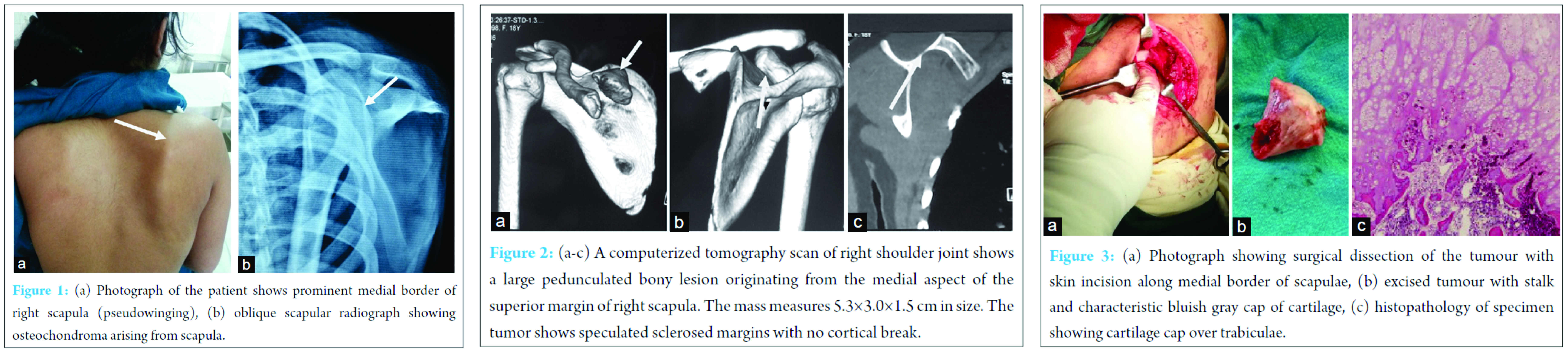
Discussion
The snapping scapula syndrome was first described by Boinet in 1867. Since then, case reports of painful snapping scapula due to scapular osteochondroma have been infrequent [26, 27, 28, 29]. The syndrome presents with pain in back and around the shoulder girdle associated with audible and/or palpable crepitus of scapula on scapulocostal movements. Milch [27] described this crepitus as a tactile-acoustic phenomenon secondary to an abnormality between the anterior surface of the scapula and the thoracic wall. Milch [27] also reported that Mauclaire divided the sounds into three classes – froissement or gentle friction sound, frottement or somewhat louder sound, and craquement or loud snapping sound. According to Milch, the second category is the most common. Although most subscapular osteochondromas are frequently associated with a snapping or grating sensation in the shoulder region [20, 27, 28, 29, 30], some of the patients reported were associated with winging or pseudowinging of the scapula [15, 28, 30].
Winging of the scapula can be either dynamic or static [15, 16, 17]. Dynamic winging is due to neuromuscular disorders and because of the resulting muscular imbalance. The deformity is produced by active and resisted shoulder movements and is often absent at rest. Static winging is due to a fixed deformity in the shoulder girdle, spine, or ribs and is characteristically present at rest with the arm at the side. Solitary exostosis or osteochondroma of the underside of the scapula may produce static winging [15, 16, 17]. Osteochondroma is the most common primary benign tumor of the scapula with an incidence of 3-4.6% [27]. Surgical resection of the tumor is the treatment of choice for a large symptomatic osteochondroma [20, 28, 30]. Carlson et al. [26] in a review of 89 cases of snapping scapula syndrome reported skeletal abnormalities in 11 cases. 27 cases were idiopathic and osteochondromas were seen in 3 cases. Carlson [26] reported that 52% (12 out of 23) patients with idiopathic type had relief of symptoms with conservative therapy, while no patient (0 out of 4) with skeletal abnormality had relief with conservative line of management. In the report of 3 cases by Danielsson and el- Haddad, winging of the scapula was the reason the children sought medical advice [16]. Out of the 5 cases of ventral osteochondroma reported by Frost et al., one case presented with pseudowinging and another had snapping scapula on presentation [19].
The osteochondroma in this case report expanded the deep surface of the right scapula, showing the scapula away from the chest wall and producing static winging. Total surgical resection was performed. Scapular osteochondroma causes snapping usually in adolescence or early adulthood [28]. The “pseudowinging” is indicative of a subscapular mass with neurologically intact serratus anterior [1]. The osteochondroma in this case report expanded the deep surface of the right scapula, showing the scapula away from the chest wall and producing static winging. Total surgical resection was performed and led to relief of symptoms.
Conclusion
To conclude, snapping scapula syndrome is a disorder caused by abnormal scapulothoracic motion of variable etiology. This syndrome may be a clinical manifestation of a subscapular osteochondroma with or without history of trauma. Surgical resection of the tumor is a reliable treatment which results in resolution of the crepitus and pain.
Clinical message
The message is that snapping scapula is a syndrome of variable etiology. It is important to differentiate between idiopathic and anatomical causes as conservative treatment is less likely to be successful if a clear anatomical cause can be found. Long-term follow-up is advised to identify rare event of local recurrence or appearance of lesions in other sites.
References
1. Mohsen MS, Moosa NK, Kumar P. Osteochondroma of the scapula associated with winging and large bursa formation. Med Princ Pract 2006;15(5):387-390.
2. Okada K, Terada K, Sashi R, Hoshi N. Large bursa formation associated with osteochondroma of the scapula: A case report and review of the literature. Jpn J Clin Oncol 1999;29(7):356-360.
3. Pongkripetch M, Sirikulchayanonta V. Analysis of bone tumors in Ramathibodi Hospital, Thailand, during 1977-1986: Study of 652 cases. J Med Assoc Thai 1989;72(11):621-628.
4. Aalderink K, Wolf B. Scapular osteochondroma treated with arthroscopic excision using prone positioning. Am J Orthop (Belle Mead NJ) 2010;39(2):E11-E14.
5. Dobelle M. An unusual location of an osteochondroma: Report of a case. J Bone Joint Surg Am 1939;21:781-784.
6. Reit RP, Glabbeek FV. Arthroscopic resection of a symptomatic snapping subscapular osteochondroma. Acta Orthop Belg 2007;73(2):252-254.
7. Tomo H, Ito Y, Aono M, Takoaka K. Chest-wall deformity associated with osteochondroma of the scapula: A case report and review of the literature. J Shoulder Elbow Surg 2005;14(1):103-106.
8. El-Khoury GY, Bassett GS. Symptomatic bursa formation with osteochondromas. AJR Am J Roentgenol 1979;133(5):895-898.
9. Wright JM, Matayoshi E, Goldstein AP. Bursal osteochondromatosis overlyong an osteochondroma of a rib: A case report. J Bone Joint Surg Am 1997;79(7):1085-1088.
10. Ogawa K, Yoshida A, Ui M. Symptomatic osteochondroma of the clavicle. A report of two cases. J Bone Joint Surg Am 1999;81(3):404-408.
11. Prakash U, Court-Brown CM. Fracture through an osteochondroma. Injury 1996;27(5):357-358.
12. Greenway G, Resnick D, Bookstein JJ. Popliteal pseudoaneurysm as a complication of an adjacent osteochondroma: Angiographic diagnosis. AJR Am J Roentgenol 1979;132(2):294-296.
13. Hershey SL, Lansden FT. Osteochondromas as a cause of false popliteal aneurysms: Review of the literature and report of two cases. J Bone Joint Surg Am 1972;54(8):1765-1768.
14. Twersky J, Kassner EG, Tenner MS, Camera A. Vertebral and costal ostoechondromas causing spinal cord compression. Am J Roentgenol Radium Ther Nucl Med 1975;124(1):124-128.
15. Bloch AM, Nevo Y, Ben-Sira L, Harel S, Shahar E. Winging of the scapula in a child with hereditary multiple exostoses. Pediatr Neurol 2002;26(1):74-76.
16. Danielsson LG, el-Haddad I. Winged scapula due to osteochondroma. Report of 3 children. Acta Orthop Scand 1989;60(6):728-729.
17. Fiddian NJ, King RJ. The winged scapula. Clin Orthop Relat Res 1984;185:228-236.
18. Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58(2):195-201.
19. Frost NL, Parada SA, Manoso MW, Arrington E, Benfanti P. Scapular osteochondroma treated with surgical excision. Orthopedics 2010;33(11):804.
20. Kumar N, Ramakrishnan V, Johnson GV, Southern S. Endoscopically-assisted excision of scapular osteochondroma. Acta Orthop Scand 1999;70(4):394-396.
21. Fukunaga S, Futani H, Yoshiya S. Endoscopically assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J Surg Oncol 2007;5:37.
22. Fageir MM, Edwards MR, Addison AK. The surgical management of osteochondroma on the ventral surface of the scapula. J Pediatr Orthop B 2009;18(6):304-307.
23. Ogawa S, Watanabe A, Ogawa K. A twelveyear-old male, large osteochondroma of the scapula. The idea of an approach: A case report. Shoulder Joint 2004;28(3):637-640.
24. Salini V, De Amicis D, Guerra G, Iarussi T, Sacco R, Orso CA. Osteochondroma of the scapula: A case report. J Orthopaed Traumatol 2007;8(1):33-35.
25. Yoo W, Kim JR, Jang KY, Lee SY, Park JH. Rapidly developed huge bursitis associated with scapular osteochondroma of the multiple exostosis: A case report. Rheumatol Int 2009;29(3):317-319.
26. Carlson HL, Haig AJ, Stewart DC. Snapping scapula syndrome: Three case reports and analysis of the literature. Arch Phys Med Rehabil 1997;78(5):506-511.
27. Milch H. Partial scapulectomy for snapping of the scapula. J Bone Joint Surg Am 1950;32-A(3):561-566.
28. Parsons TA. The snapping scapula and subscapular exostoses. J Bone Joint Surg Br 1973;55(2):345-349.
29. Strizak AM, Cowen MH. The snapping scapula syndrome. A case report. J Bone Joint Surg Am 1982;64(6):941-942.
30. Cooley LH, Torg JS. “Pseudo winging” of thescapula secondary to sub scapularosteochondroma. Clin Orighthop 1982;162:119-124.
| How to Cite This Article: Rameez R, Ul-Hassan M, Kotwal HA, Kangoo KAH, Nazir A. Painful Pseudowinging and Snapping of Scapula due to Subscapular Osteochondroma: A Case Report. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):96-99. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-652-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


