
[box type=”bio”] What to Learn from this Article?[/box]
Median nerve entrapment following elbow dislocation is a rare entity. A high index of suspicion is necessary to arrive at a diagnosis. Ultrasonography (USG) is very helpful in localizing, the position of entrapped median nerve and hence guiding the treatment.
Case Report | Volume 7 | Issue 3 | JOCR May – June 2017 | Page 21-24| Vivek Dubey, Ali Saify, Ashwin Samant, Sunil Shahane DOI: 10.13107/jocr.2250-0685.788
Authors:
Vivek Dubey[1], Ali Saify[1], Ashwin Samant[1], Sunil Shahane[1]
[1]Department of Orthopaedics, H.B.T. Medical College and Dr. R.N. Cooper Hospital, Mumbai. Maharashtra. India.
Address of Correspondence:
Dr. Vivek Dubey,
Room No. 305, RMO Quarters, Dr. R.N. Cooper Municipal General Hospital,
N.S. Road no.1, Vile Parle (W), Mumbai – 400 056, Maharashtra, India,
E-mail: vvk7878@gmail.com
Abstract
Introduction: Median nerve entrapment in the cases of posterior dislocation of elbow is a rare entity. The diagnosis is usually delayed. We describe here a case of median nerve entrapment in the posteromedial dislocation of elbow in a 10-year-old male child and the role of ultrasonography (USG) in localizing the median nerve in the elbow. The nerve release was done by osteotomy of medial epicondyle. USG thus proved to be a useful tool in the management of nerve injury.
Case Report: The authors present here a case of 10-year-old child with a history of dislocation of right elbow that was reduced elsewhere and the child presented to us with stiffness and restriction of movements at the elbow with the features of high median nerve injury. On further evaluation with ultrasound, the median nerve was found to be entrapped in the elbow behind the medial epicondyle. Medial condyle osteotomy was done to release the median nerve and to provide the relief of symptoms.
Conclusion: Median nerve entrapment after the elbow dislocation is a very rare entity. High index of suspicion and the ultrasound are quite helpful in arriving at the diagnosis of this rare clinical entity. Timed surgical release of the nerve and can provide good function.
Keywords: Median nerve, elbow dislocation, ultrasonography, Matev sign.
Introduction
Entrapment of the median nerve in the elbow is a rare yet severe complication of elbow dislocation and reduction. Primarily a problem that occurs in children, its incidence is approximately 3% of all elbow dislocations [1]. In this case report, we attempt to highlight the role of ultrasonography (USG) in the localizing the nerve injury and hence its proper management.
Case Report
A 10-year-old right-hand dominant male child presented to us with a history of posteromedial dislocation of the right elbow which was reduced elsewhere 2 months ago. On clinical examination, the child had pain, stiffness, 30° of fixed flexion deformity (Fig. 1), and features of high median nerve injury with weakness in the long flexors of index finger and thumb, and hypoesthesia on the tip of index finger. However, the joint was well reduced with no myositis (Fig. 2). Electromyography (EMG) and nerve conduction velocity (NCV) confirmed the axonal injury at the level of elbow (Fig. 3). USG reported the nerve being trapped in the elbow behind the medial epicondyle and further pinching in extension (Fig. 4). Review of literature has only four such reports of this rare injury with a Matev sign to predict this on X-ray. Nerve exploration corroborated this precise descriptiond a medial epicondyle osteotomy was needed to release entrapped nerve as advised in the literature.
In our case, we took anterior approach curvilinear across the cubital fossa. Nerve exploration was done tracing the median nerve distally and proximally. Entrapped nerve was released after medial epicondyle osteotomy and the nerve was placed in front of the elbow in its normal site. Nerve badly contused but intact (Fig. 5).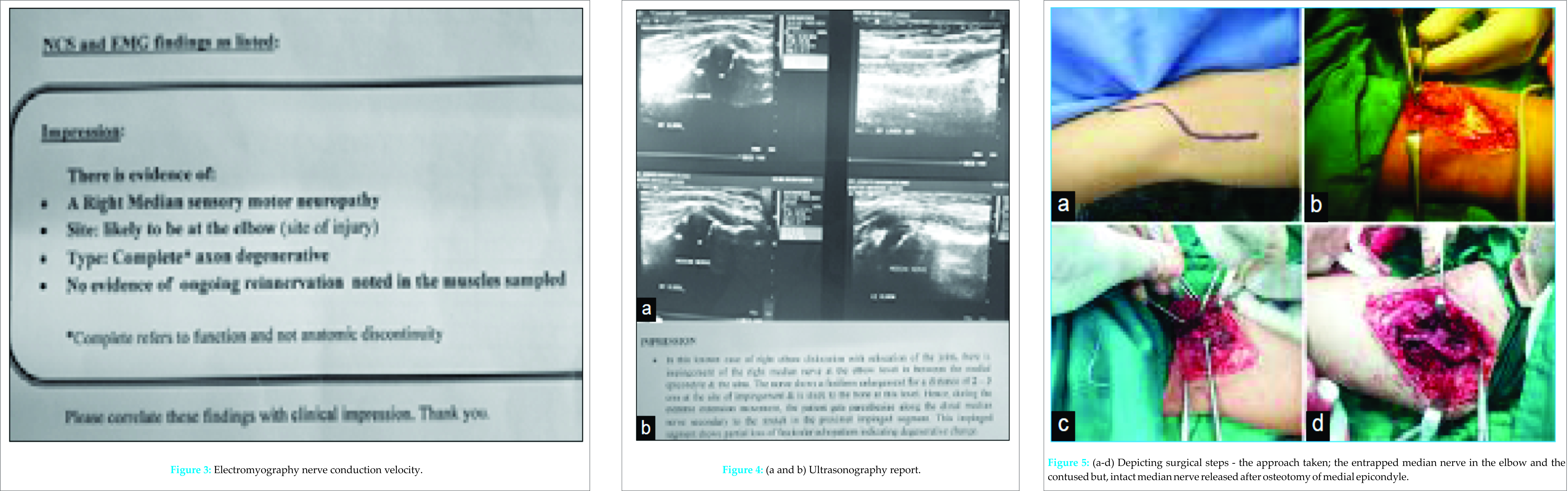
Discussion
Four types of entrapment have been described: Types I-III by Hallet [2] and Type IV by Al-Qattan et al. [3]. Type I consists of the median nerve slipping posteriorly behind a torn medial collateral ligament and adhering to the posterior surface of the humerus. Type II is defined when a median nerve becomes entrapped by healed bone after running through a fractured epicondyle. In Type III, the nerve becomes entrapped in the humeroulnar joint [2]. Type IV is a combination of Types I and II [3]. Despite the different methods of entrapment there is one common end point: Compression leading to ischemia of the nerve. Chronic compression and ischemia in neural tissue can lead to intraneural fibrosis and eventual Wallerian degeneration [4]. In addition, median nerve entrapment is often diagnosed late (3 months to 2.5 years post-injury), which contributes to the extent of median nerve injury [5]. The late diagnosis is not uncommon because the presence of a transient neuropraxia created by contusions or stretching at the time of injury can mimic the signs of an early entrapment [5]. Furthermore, children often have difficulty vocalizing their symptoms, making any deficit less apparent [5]. Diagnosis has generally consisted of recognizing any non-resolving deficits over time and surgical exploration of the elbow. Radiological changes described by Matev [6] can often be found in cases presenting late due to chronic force applied to the cortex of the bone. Treatment of median nerve entrapment has ranged from simple release and neurolysis to excision and end-to-end anastomosis or nerve grafting. If entrapment does occur, early diagnosis can lead to restoration using less invasive measures. Both simple nerve release and neurolysis have demonstrated positive results when the entrapment is caught early, and the nerve is not extensively damaged [7, 8, 9, 10, 11, 12, 13, 14]. USG is a powerful tool to aid in diagnosis pre-operatively. USG shows the course of the median nerve and can also serve as an adjunct to electromyography in evaluation of muscle denervation through assessment of muscle atrophy. Early diagnosis and treatment will favor a normal result. In a case described by Korus et al., Type III pattern of median nerve entrapment was found in a 7-year-old girl, who presented with fixed flexion deformity of 20° and anterior interosseous nerve palsy 10 months after the initial injury. On clinical evaluation, there was inability to use flexor digitorum superficialis in digits 2-5, and flexor digitorum superficialis to index finger and no function in flexor pollicis longus. Numbness of index finger and thumb and wasting of thenar muscle mass was noticed. EMG showed right median nerve neuropathy. On surgical exploration, the nerve was found to be encased in the elbow joined, the proximal and distal ends of the nerve were isolated and sural nerve grafting was done. At 3-month follow-up, nerve regeneration was present as demonstrated by Tinel’s sign [15]. Lars G. Danielson described a similar condition in an 11-year-old boy which was diagnosed 11 months after posterior dislocation of elbow with medial epicondyle humerus fracture. Median nerve was explored proximally and distally, bone encircling the median nerve was nibbled. Flexor muscles and ligaments were released subperiosteally from the epicondyle. Median nerve was then embedded in a fat and placed in its normal location in front of the elbow joint. Post-operatively, the boy gradually improved after 10 months [11]. Mannerfelt described a case of median nerve entrapment soon after the reduction of posterior dislocation of the right elbow in a 9-year-old boy. Soon after the effect of anesthesia, clinical symptoms in the hand were suggestive of median nerve injury. On surgical exploration,the tendon of biceps was found to be intact but, the tendon of brachialis was torn off. Median was traced and was found to be in the joint between humerus and ulna. With traction and joint manipulation, the median nerve was freed and was found to be in continuity. Nerve was decompressed by splitting the sublimis ridge. The boy gradually regained full function after surgery [14]. In our case, patient presented 2 months after the injury with pain, stiffness, deformity, and features of high median nerve injury. The type of nerve injury was evaluated with EMG NCV study and the nerve was localized with USG. USG helped in exactly localizing the nerve where it was entrapped behind the medial epicondyle in the elbow. Intraoperatively, the nerve was found to be in the same location as revealed by USG. The nerve was released by osteotomy of medial epicondyle; hence, the patient is expected to have a good outcome post-operatively.
Conclusion
Median nerve entrapment following the elbow dislocation is a rare entity, and the diagnosis of the nerve injury is frequently delayed. However, prompt clinical suspicion, diagnostic tools such as USG can lead to accurate diagnosis, and then provide the exact situation of trapped median nerve. After the localization of nerve, nerve release can be done which usually ensures a good functional outcome in terms of regaining of median nerve function.
Clinical Message
Median nerve entrapment following the elbow dislocation and its reduction is a rare occurrence. The authors believe that high clinical suspicion is necessary, to make the diagnosis and at the same time the appropriate surgery to be performed to provide a good recovery. Ultrasound is an effective and economically affordable tool to confirm the clinical diagnosis.
References
1. Ogden JA. Skeletal Injury in the Child. Berlin: Springer-Verlag; 2000. p. 550-551.1. Ogden JA. Skeletal Injury in the Child. Berlin: Springer-Verlag; 2000. p. 550-551.
2. Hallett J. Entrapment of the median nerve after dislocation of the elbow. A case report. J Bone Joint Surg Br 1981;63-B(3):408-412.
3. al-Qattan MM, Zuker RM, Weinberg MJ. Type 4 median nerve entrapment after elbow dislocation. J Hand Surg Br 1994;19(5):613-615.
4. Mackinnon SE, Lee Dellon A. Surgery of the Peripheral Nerve. New York: Thieme Medical Publishers; 1988.
5. Noonan KJ, Blair WF. Chronic median-nerve entrapment after posterior fracture-dislocation of the elbow. A case report. J Bone Joint Surg Am 1995;77(10):1572-1575.
6. Matev I. A radiological sign of entrapment of the median nerve in the elbow joint after posterior dislocation. A report of two cases. J Bone Joint Surg Br 1976;58(3):353-355.
7. Rao SB, Crawford AH. Median nerve entrapment after dislocation of the elbow in children. A report of 2 cases and review of literature. Clin Orthop Relat Res 1995;312:232-237.
8. Thorleifsson R, Karlsson J, Thorsteinsson T. Median nerve entrapment in bone after supracondylar fracture of the humerus. Case report. Arch Orthop Trauma Surg 1988;107(3):183-185.
9. Floyd WE 3rd, Gebhardt MC, Emans JB. Intra-articular entrapment of the median nerve after elbow dislocation in children. J Hand Surg Am 1987;12:704-707.
10. Kietsiriroje N, Thepchatri A. Median nerve entrapment after an unusual fracture dislocation of the elbow: A case report. J Med Assoc Thai 1987;70(4):234-237.
11. Danielsson LG. Median nerve entrapment in elbow dislocation. A case report. Acta Orthop Scand 1986;57(5):450-452.
12. Pritchett JW. Entrapment of the median nerve after dislocation of the elbow. J Pediatr Orthop 1984;4(6):752-753.
13. St Clair Strange FG. Entrapment of the median nerve after dislocation of the elbow. J Bone Joint Surg Br 1982;64(2):224-225.
14. Mannerfelt L. Median nerve entrapment after dislocation of the elbow. Report of a case. J Bone Joint Surg Br 1968;50(1):152-155.
15. Korus L, Morhart M, Jarman A, Olson J. Median nerve reconstruction after entrapment in the elbow. Can J Plast Surg 2009;17(4):130-132.
 |
 |
 |
 |
| Dr. Vivek Dubey | Dr. Ali Saify | Dr. Ashwin Samant | Dr. Sunil Shahane |
| How to Cite This Article: Dubey V, Saify A, Samant A, Shahane S. Median Nerve Entrapment after Elbow Dislocation and the Role of Ultrasonography – A Case Report. Journal of Orthopaedic Case Reports 2017 May-Jun;7(3):21-24 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


