
[box type=”bio”] What to Learn from this Article?[/box]
All patients of thalassemia major should also be screened for the complication of Avascular necrosis of the femur for early diagnosis and management.
Case Report | Volume 7 | Issue 3 | JOCR May – June 2017 | Page 38-40| Geeta Mandhani, Manas Kalra, Ramani Narasimhan, V K Khanna, Amita Mahajan. DOI: 10.13107/jocr.2250-0685.796
Authors:
Geeta Mandhani[1], Manas Kalra[1], Ramani Narasimhan[1], V K Khanna[2], Amita Mahajan[1]
[1] Department of Pediatric Hematology-Oncology, Indraprastha Apollo Hospital, New Delhi, India.
[2] Department of Pediatrics, Sir Gangaram Hospital, New Delhi, India.
Address of Correspondence
Dr. Amita Mahajan,
Department of Pediatric Hematology-Oncology,
Indraprastha Apollo hospital, New Delhi, India.
E-mail: mahajanamita1@gmail.com
Abstract
Introduction: Avascular necrosis of the head of femur (AVNF) has frequently been reported with sickle cell anemia but is not commonly associated with beta thalassemia.
Case Report: We report a case of 14-year-old male with transfusion-dependent thalassemia (TDT) and hepatitis C, who developed bilateral atraumatic AVNF requiring surgical correction. The likely etiopathogenesis and the review of literature for this uncommon finding are discussed.
Conclusion: AVNF should be considered as a possibility in a patient with TDT presenting with hip pain. Multiple disease and treatment related factors are likely to play a key role in its causation.
Keywords: Avascular necrosis of femur, transfusion dependent thalassemia, interferon.
Introduction
Transfusion-dependent thalassemia (TDT) patients are known to develop a number of osseous abnormalities. However, avascular necrosis of the head of the femur (AVNF) has been very rarely reported in this population despite the wide prevalence of TDT in our part of the world.
Case Report
A 14-year-old young boy with TDT on regular chelation presented with progressively worsening pain in both hip joints associated with limp for 6 months. Plain radiographs were unremarkable. The bone mineral density evaluation showed mild osteopenia. Magnetic resonance imaging revealed bilateral AVNF, with the right side being more severely affected (Fig. 1). He had been optimally transfused. He had received deferiprone in the past, but this had been discontinued over 2 years ago due to arthralgias. He was currently receiving deferasirox chelation therapy at 40 mg/kg/day, and the most recent serum ferritin was 2600 ng/ml. He had been detected to be seropositive for hepatitis C 2 years ago and had been commenced on treatment with interferon alpha. The hip pain first became evident in the past month of interferon therapy.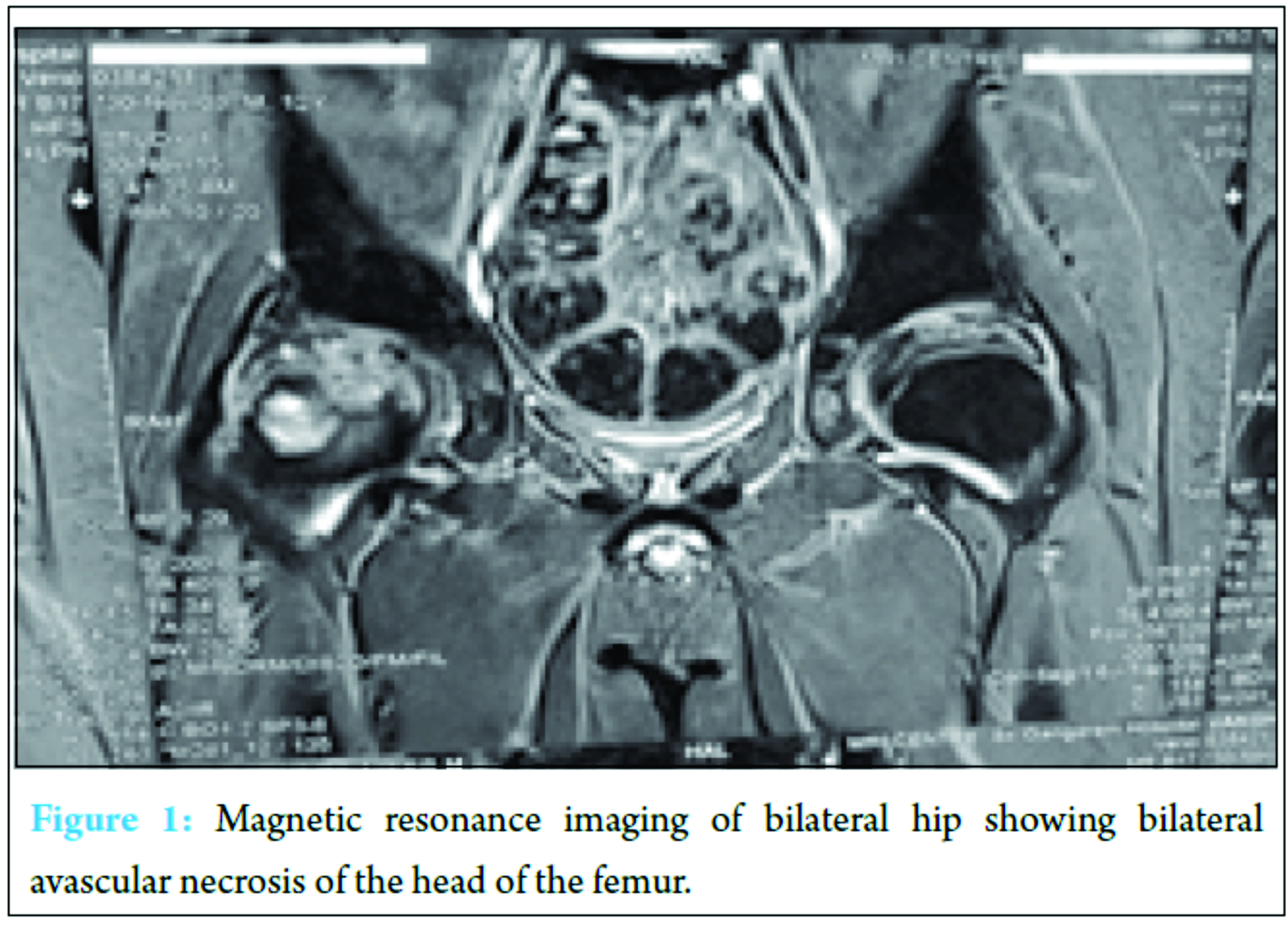
He was initially managed conservatively with bed rest and analgesia. However, in view of poor response to conservative management and worsening symptomatology, it was decided to take him up for orthopedic surgical correction with varus derotation osteotomy of the right hip and fixation and core decompression of the left hip. On 9 months post-surgery, he is asymptomatic and fully ambulatory.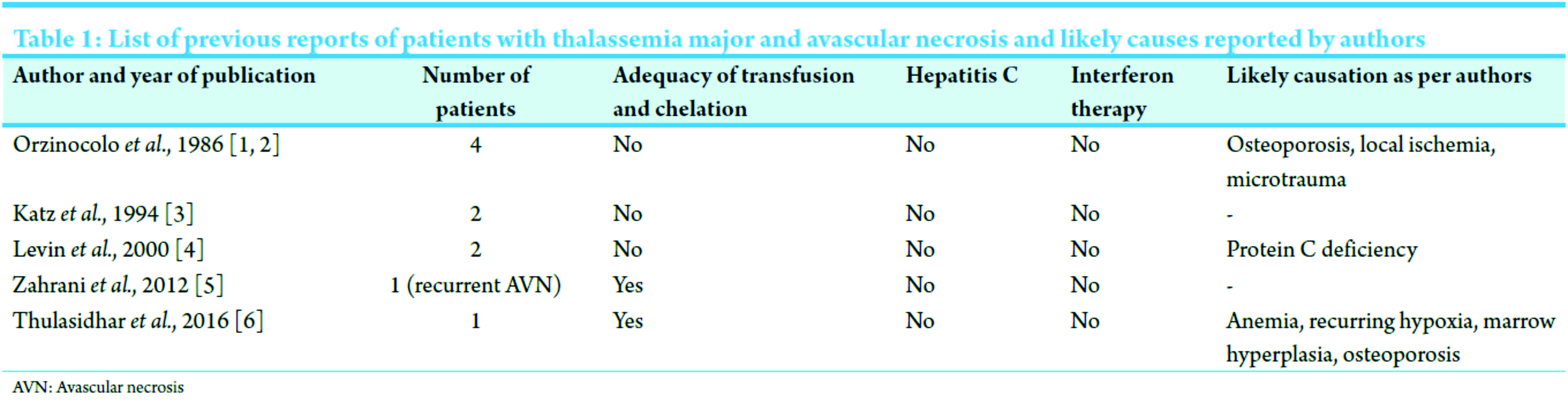
Discussion
AVNF is a pathological process that results from interruption of the blood supply to a segment of the femoral head, which subsequently undergoes necrosis and collapse. Both traumatic and atraumatic etiologies for this condition have been described. Common causes include long-term steroid treatment, fracture and dislocation of hip joints, and vascular diseases such as systemic lupus erythematosus, sickle cell disease and conditions associated with hypercoagulability such as polycythemia and malignancies. TDT patients are known to develop a number of bone complications like arthralgias, osteopenia, osteoporosis, bone pain, increased fracture risk and deforming bony changes. The underlying etiology for above is multifactorial and commonly attributed to ineffective erythropoiesis, iron overload, chelation with desferrioxamine and deferiprone, Vitamin D deficiency, endocrinopathies such as hypogonadism and growth hormone deficiency, and the thalassemia genotype. However, its association with AVNF has not been commonly reported. Extensive review of literature shows only a few case reports of avascular necrosis complicating thalassemia major. It was first described in 1986 in four patients in a series of 280 thalassemics [1, 2]. The authors speculated the predisposing factors to be anemic hypoxia and/or osteopenia. Katz et al. in 1994 while studying the pattern of bone diseases in TDT reported two cases of AVNF [3]. In another anecdotal report by Levin et al. in 2000, two cases were reported in a cohort of 79 patients of thalassemia major, but both of them had severe hemosiderosis and one had chronic hepatitis C [4]. The author in the above case report speculated protein C deficiency secondary to liver hemosiderosis as an additional risk factor for AVNF in TDT. Two more recent case reports describe AVNF in TDT patients [5, 6]. Table 1 summarizes the cases of AVNF in TDT reported to date. AVNF has also been reported in patients with hepatitis C who have received interferon therapy. Landerreche et al. reported five patients of AVNF with hepatitis C infection treated with pegylated interferon [7]. Lauer and Walker hypothesized that viral infections itself involve an autoimmune process and may result in transient vasculitis [8]. In a study by Galli et al., thrombotic tendencies have been reported with viral hepatitis [9]. Interferon alpha in itself is known to have anti-angiogenic properties and may affect vascularization of the femoral head leading to AVNF [10].
Conclusion
AVNF in patients with TDT may have a multifactorial etiology and it may be difficult to identify one key factor. Even in our patient, there may have been interplay of multiple factors, important ones being.
Clinical Message
Any patient with Thalassemia major who complains of persistent hip pain should be evaluated for a vascular necrosis of head of femur especially if receiving interferon therapy.
References
1. Orzincolo C, Scutellari PN, Bariani L, Pinca A, Beccari G, Castaldi G. Aseptic necrosis of the head of the femur in Cooley’s disease. Radiol Med 1986;72(3):102-104.1. Orzincolo C, Scutellari PN, Bariani L, Pinca A, Beccari G, Castaldi G. Aseptic necrosis of the head of the femur in Cooley’s disease. Radiol Med 1986;72(3):102-104.
2. Orzincolo C, Castaldi G, Scutellari PN, Bariani L, Pinca A. Aseptic necrosis of femoral head complicating thalassemia. Skeletal Radiol 1986;15(7):541-544.
3. Katz K, Horev G, Goshen J, Tamary H. The pattern of bone disease in transfusion-dependent thalassemia major patients. Isr J Med Sci 1994;30(8):577-580.
4. Levin C, Zalman L, Shalev S, Mader R, Koren A. Legg-Calvé-Perthes disease, protein C deficiency, and beta-thalassemia major: Report of two cases. J Pediatr Orthop 2000;20(1):129-131.
5. Zahrani H, Malhan H, Al-Shaalan M. Recurrent avascular necrosis of the femoral head and intramedullary bone infarcts in thalassemia major. J Appl Hematol 2012;3(3):127-128.
6. Thulasidhar AN, Kumar S, Aroor S, Mundkur S. Avascular necrosis of femoral head in a child with beta thalassaemia major. J Clin Diagn Res 2016;10(9):SL03.
7. Landerreche JG, Orbezo FG, Domínguez HM, Álvarez N, Davalillo T, Tripp C. Non-traumatic causes of bilateral avascular necrosis of the femoral head: relationship hepatitis C-pegylated interferon. Acta Ortop Mex 2015;29(3):172-175.
8. Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med 2001;345(1):41-52.
9. Galli L, Gerdes VE, Guasti L, Squizzato A. Thrombosis associated with viral hepatitis. J Clin Transl Hepatol 2014;2(4):234-239.
10. Kozuch P, Talpaz M, Faderl S, O’Brien S, Freireich EJ, Kantarjian H. Avascular necrosis of the femoral head in chronic myeloid leukemia patients treated with interferon-alpha: A synergistic correlation? Cancer 2000;89:1482-1489.
 |
 |
 |
 |
 |
| Dr. Geeta Mandhani | Dr. Manas Kalra | Dr. Ramani Narasimhan | Dr. V K Khanna | Dr. Amita Mahajan |
| How to Cite This Article: Mandhani G, Kalra M, Narasimhan R, Khanna VK, Mahajan A. A Case of Non-Traumatic Avascular Necrosis of Femur in Case of Transfusion-Dependent Thalassemia. Journal of Orthopaedic Case Reports 2017 May-June;7(3):38-40 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


