
[box type=”bio”] What to Learn from this Article?[/box]
Curettage using a bent and looped soft-wire through the small fenestration is a minimally invasive procedure for enchondroma in the phalanx.
Case Report | Volume 7 | Issue 3 | JOCR May – June 2017 | Page 67-70| Akio Sakamoto, Shuichi Matsuda. DOI: 10.13107/jocr.2250-0685.810
Authors: Akio Sakamoto[1], Shuichi Matsuda[1]
[1] Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Address of Correspondence:
Dr. Akio Sakamoto,
Department of Orthopaedic Surgery, Graduate School of Medicine,
Kyoto University, Shogoin, Kawahara-cho 54, Sakyo-ku,
Kyoto 606-8507, Japan.
E-mail: akiosaka@kuhp.kyoto-u.ac.jp
Abstract
Introduction: Enchondromas are benign bone cartilaginous lesions predominantly seen in the hand, possibly leading to a pathological fracture. When the lesion expands to the whole phalanx, curettage through a small fenestration is difficult. To overcome the problem, soft-wire (cerclage wire) was used as a curette. Soft-wire is commonly used for a tension band wiring method for patellar or olecranon fractures.
Technique: Two representative cases are presented: one is a 43-year-old male with enchondroma in the middle phalanx of the left index finger, and the other is a 28-year-old female with enchondroma in the distal phalanx of the right thumb. Surgery was performed in both cases under general anesthesia. The cortex adjacent to the lesion was approached dorsally, splitting the extensor tendon (the index finger case), or laterally (the thumb case). Fenestration of the cortex was performed with a 3.2-4 mm diameter surgical air drill. A bent and looped soft-wire of 0.7 or 0.9 mm diameter was threaded through the fenestration and used as a curette. Consequently, β-tricalcium phosphate particles were implanted. Bone incorporation was observed.
Conclusion: This easy technique of curettage is a minimally invasive procedure for enchondroma. Moreover, the length of the skin incision and the size of the cortical fenestration are the same regardless of the size of the lesion.
Keywords: Enchondroma, phalanx, curettage, soft-wire.
Introduction
Enchondromas are benign cartilaginous lesions predominantly seen in the skeleton of the hand [1, 2]. The majority of enchondromas remain asymptomatic. However, a large lesion can lead to a pathological fracture. Enchondromas of the hand are typically discovered by chance or because of a fracture [3]. Curettage with/without bone grafting is the advisable treatment [4]. Soft-wire, or cerclage wire, is commonly used in tension band wiring, which is one of the most common treatment methods for a transverse patellar fracture [5] or transverse olecranon fracture [6]. The principle of tension band wiring is based on the premise of conversion from distraction force to compression force at the fracture site. In this report, a new technique using soft-wire as a curette through a small fenestration is reported. In the current article, two representative cases are presented.
Technique
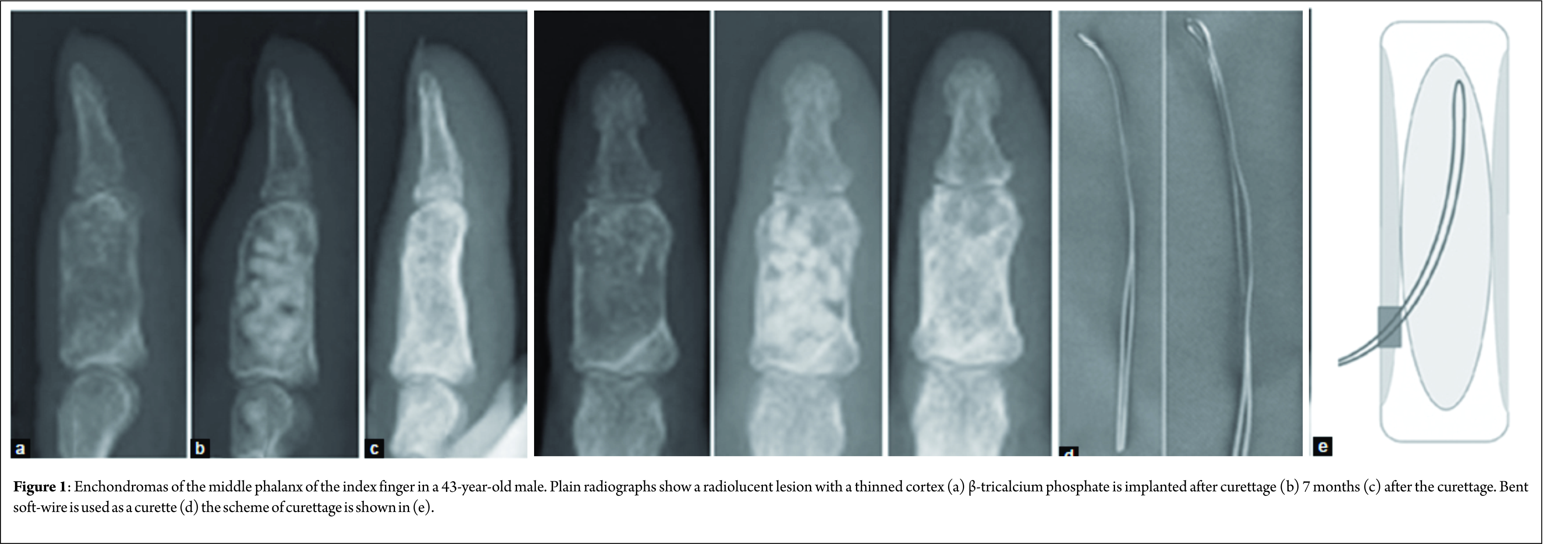
In the current article, two representative cases are presented. One is a 43-year-old male with enchondroma in the middle phalanx of the left index finger (Fig. 1), and the other is a 28-year-old female with enchondroma in the distal phalanx of the right thumb (Fig. 2). In both cases, the plain radiographs showed a radiolucent lesion with a thinned but expanded cortex. Both lesions have expanded to the whole bone. These features of the plain radiographs are typical of enchondroma. Surgery was performed in both cases under general anesthesia. The cortex adjacent to the lesion was approached dorsally, splitting the extensor tendon (the index finger case), or laterally (the thumb case). Fenestration of the cortex was performed with a 3.2-4 mm diameter surgical air drill. A bent and looped soft-wire of 0.7 or 0.9 mm diameter was threaded through the fenestration and used as a curette (Fig. 2). Complete access of the soft-wire within the whole lesion was assessed and confirmed with a fluoroscopic image during the operation. Residual fragmented enchondroma tissue was washed away by saline using a syringe with a plastic needle. Consequently, β-tricalcium phosphate (TCP) particles were implanted (Fig. 1 and 2). The diagnosis of enchondroma was confirmed on the resected lesion. There were no complications associated with the operation. The range of motion in the adjacent joint was not restricted.
Discussion
The curettage tools for a bone tumor are solid metal. Since these tools lack flexibility, the size of the fenestration at the adjacent cortical bone depends on the size of the lesion. Therefore, when the enchondroma extends to the whole bone, the fenestration should be extended to the whole lesion. Moreover, an extension of the fenestration is difficult in the small finger bones. To overcome this problem, a bent and looped soft-wire of 0.7 or 0.9 mm diameter was threaded through the fenestration and used as a curette. With this method, regardless of the size of the enchondroma, one small fenestration of 3.2-4 mm diameter created by a surgical air drill is sufficient for curettage. In the current case, the cavity was filled with β-TCP after curettage. In the previous report, bone grafting after curettage is reported to be unnecessary in the treatment of enchondromas because there is no difference in midterm clinical results with and without bone grafting [7]. For the treatment of enchondroma in the phalanx, implantation of β-TCP seems optional, while curettage is important. Curettage is a standard surgical method for enchondroma [4] and sometimes is performed using interosseous endoscopy-guided surgery [8]. After the curettage, cancellous bone (autograft or allograft), polymethyl methacrylate, and hydroxyapatite, as well as β-TCP, are used as fillers [4, 9, 10, 11]. Filling the cavity with cancellous bone or other non-structural bone substitutes does not enhance the strength of the construct [12]. Therefore, a small fenestration of the cortex is required to avoid a possible fracture after the operation.
Conclusion
The method is simple, and the skin incision and the size of the cortical fenestration are also the same regardless of the size of the lesion. Consequently, surgical time is minimized, which facilitates planning.
Clinical Message
Enchondromas are benign bone cartilaginous lesions predominantly seen in the hand, possibly leading to a pathological fracture. When the lesion expands to the whole phalanx, curettage through a small fenestration is difficult. To overcome the problem, soft-wire was used as a curette with a small fenestration. The method is simple. Moreover, the length of the skin incision and the size of the cortical fenestration are the same regardless of the size of the lesion.
References
1. Dorfman HD, Czerniak B. Bone Tumors. St Louis: Mosby; 1998.1. Dorfman HD, Czerniak B. Bone Tumors. St Louis: Mosby; 1998.
2. Raducu L, Anghel A, Vermesan S, Sinescu RD. Finger enchondroma treated with bone substituents-A case presentation. J Med Life 2014;7(2):223-225.
3. Rajeh MA, Diaz JJ, Facca S, Matheron AS, Gouzou S, Liverneaux P. Treatment of hand enchondroma with injectable calcium phosphate cement: A series of eight cases. Eur J Orthop Surg Traumatol 2017;27(2):251-254.
4. Lubahn JD, Bachoura A. Enchondroma of the hand: Evaluation and management. J Am Acad Orthop Surg 2016;24(9):625-633.
5. Schnabel B, Scharf M, Schwieger K, Windolf M, Pol Bv, Braunstein V, et al. Biomechanical comparison of a new staple technique with tension band wiring for transverse patella fractures. Clin Biomech (Bristol, Avon) 2009;24(10):855-859.
6. Schneider MM, Nowak TE, Bastian L, Katthagen JC, Isenberg J, Rommens PM, et al. Tension band wiring in olecranon fractures: The myth of technical simplicity and osteosynthetical perfection. Int Orthop 2014;38(4):847-855.
7. Schaller P, Baer W. Operative treatment of enchondromas of the hand: Is cancellous bone grafting necessary? Scand J Plast Reconstr Surg Hand Surg 2009;43(5):279-285.
8. Taleb C, Gouzou S, Mantovani G, Liverneaux P. Treatment of benign bone tumours of the hand using osteoscopy. Chir Main 2010;29(2):78-81.
9. Uchida A, Araki N, Shinto Y, Yoshikawa H, Kurisaki E, Ono K. The use of calcium hydroxyapatite ceramic in bone tumour surgery. J Bone Joint Surg Br 1990;72(2):298-302.
10. Kim JK, Kim NK. Curettage and calcium phosphate bone cement injection for the treatment of enchondroma of the finger. Hand Surg 2012;17(1):65-70.
11. Yasuda M, Masada K, Takeuchi E. Treatment of enchondroma of the hand with injectable calcium phosphate bone cement. J Hand Surg Am 2006;31(1):98-102.
12. Pianta TJ, Baldwin PS, Obopilwe E, Mazzocca AD, Rodner CM, Silverstein EA. A biomechanical analysis of treatment options for enchondromas of the hand. Hand (N Y) 2013;8(1):86-91.
 |
 |
| Dr. Akio Sakamoto | Dr. Shuichi Matsuda |
| How to Cite This Article: Sakamoto A, Matsuda S. Curettage Using Soft-wire for Enchondroma in the Hand: A Technical Note. Journal of Orthopaedic Case Reports 2017 May-June;7(3):67-70 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


