
[box type=”bio”] Learning Points for this Article: [/box]
Follow a standard protocol while inserting and removing a drain and observe caution, so as to avoid an easily avoidable complication such as breakage and retention of drain fragment.
Case Report | Volume 7 | Issue 4 | JOCR July – August 2017 | Page 10-12| Ravi Gupta, Anubhav Malhotra, Munish Sood, Gladson David Masih. DOI: 10.13107/jocr.2250-0685.826
Authors: Ravi Gupta[1], Anubhav Malhotra[1], Munish Sood[2], Gladson David Masih[1]
[1] Department of Orthopaedics, Government Medical College and Hospital, Chandigarh, India.
[2] Department of Orthopaedics, Trained in Arthroscopy Command Hospital, Chandi Mandir, Panchkula, Haryana, India.
Address of Correspondence
Dr. Ravi Gupta
Department of Orthopaedics, Sports Injury Centre, Government Medical College and Hospital, Chandigarh, India.
E-mail: ravikgupta2000@yahoo.com
Abstract
Introduction: Breaking of surgical drain during the removal and retention of broken drain fragment is an avoidable complication. Such a complication brings disrepute to the operating team and causes psychological as well as further surgical trauma to the patient as a return to the operating room is required many a times to remove the retained drain fragment.
Case Report: We report a case of an undetected retained drain fragment inside the knee joint of a 24-year-old male international kabaddi player, who remained asymptomatic for 5 months, when the residual drain fragment was removed arthroscopically. No such case has been reported earlier in the literature after arthroscopic surgery.
Conclusion: Retained drain fragment after arthroscopic surgery can stay silent for months. Hence, a high index of suspicion should be maintained by surgeons to detect such a complication at the earliest. We suggest that every arthroscopic surgeon should follow a standard protocol while inserting and removing the drain to avoid this mistake.
Keywords: Retained drain, anterior cruciate ligament injury, sports player
Introduction
The use of surgical drains is associated with an avoidable complication of breaking of drain and retention of broken drain fragment [1].This can cause significant embarrassment to the surgical team and increased harassment to the patient as it usually requires a return to the operating room to extricate the retained drain fragment [2]. It is detrimental socially, economically, and functionally. Furthermore, it can cause limitation or delay of sportsperson’s return to pre-injury level of sports activity.The use of surgical drains is associated with an avoidable complication of breaking of drain and retention of broken drain fragment [1].This can cause significant embarrassment to the surgical team and increased harassment to the patient as it usually requires a return to the operating room to extricate the retained drain fragment [2]. It is detrimental socially, economically, and functionally. Furthermore, it can cause limitation or delay of sportsperson’s return to pre-injury level of sports activity.We present a case of breakage of surgical drain during the removal and retention of the broken drain fragment inside the knee joint of an international kabaddi player after arthroscopic anterior cruciate ligament (ACL) reconstruction. We were unable to find any such report in the literature.
Case Report
A 24-year-old male, international Kabaddi player, underwent arthroscopic ACL reconstruction using hamstring autograft with preserved tibial insertions with the help of endobutton (Smith and Nephew, Mumbai, India, Ltd.) along with partial meniscectomy for the flap tear of lateral meniscus. After the surgery, suction drain (Romovac suction drain, No. 12, Romsons International, Noida, India, Ltd.) was placed in the knee through the anterolateral arthroscopic portal without securing the drain with a skin suture. The drain was removed by a resident in the ward after a period of 24 h. The patient regained full range of motion at the knee joint and a good quadriceps control on the 3rd post-operative day when he was discharged. He was put on our standard aggressive ACL rehabilitation program. He was able to tolerate the program comfortably for 5 months, with complaints of mild intermittent pain in the joint on terminal flexion. At 5 months, when he was advised to start practice game of kabaddi, he started feeling discomfort in the operated knee. The discomfort restricted his progression in the game. With this complaint, he visited us in the outpatient department when an X-ray of the affected knee showed the shadow of a retained drain fragment inside the knee joint (Fig.1). 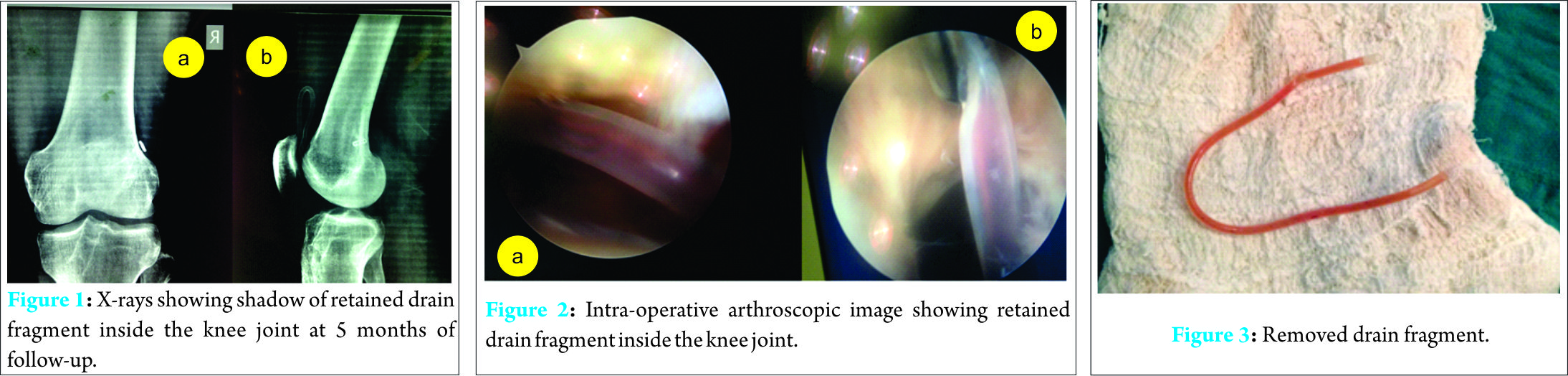 He was immediately taken to operation theatre, and the residual drain fragment was removed arthroscopically (Fig.2 and 3). At his latest follow-up (16-month post-ACL surgery and 11 months after removal of the drain), the patient had regained full function and was playing at the pre-injury level of 10 as per Tegner scale of sports activity [3].
He was immediately taken to operation theatre, and the residual drain fragment was removed arthroscopically (Fig.2 and 3). At his latest follow-up (16-month post-ACL surgery and 11 months after removal of the drain), the patient had regained full function and was playing at the pre-injury level of 10 as per Tegner scale of sports activity [3].
Discussion
The literature is divided on the use of surgical drains [4, 5, 6, 7, 8, 9].The use of drains is associated with certain advantages such as decreased hematoma formation, less chance of developing ecchymosis, and little need for the change of post-operative dressing [10]. However, wound healing and infection appear unaffected with or without the use of surgical drains [4, 5, 6, 7, 8, 9]. Since hematoma in the knee has the potential to delay/slow down the post-operative ACL rehabilitation protocol, we routinely use a surgical drain in our patients.The exact cause of breakage of the drain in the present case could not be ascertained in the hindsight due to late recognition of the complication. It may be due to the fact that the drain was inadvertently caught in the skin suture of the anterolateral portal through which the drain tubing was passed. The recognition of this complication was delayed primarily because the resident was unable to identify that the removed tubing of the drain was incomplete and also due to the fact that the patient was able to follow the rehabilitation protocol with minimal symptoms for 5 months. He reported to us only when he was not able to enhance his progress in the game. We feel fortunate that this complication was detected during the period of rehabilitation only, when he was not fit to play. Thus, his career was not affected, and he was able to join back the game with a Tegner scale score of 10 without wasting any time.A review of the literature indicates that drain entrapment and breakage is underreported and frequently requires additional interventions for drain removal [11, 12, 13]. We were successfully able to remove the retained drain fragment arthroscopically without causing much morbidity to the patient. Hence, we suggest that if such a situation arises, then arthroscopic removal of the residual drain fragment is an excellent option as it is technically easy and does not cause much surgical morbidity.In the literature, the retained drain fragments have resulted in lawsuits being filed against hospitals [14]. We were able to counsel the patient about this complication and a prompt action on our part for removal of the drain helped us to avoid a medico-legal situation.Several authors have outlined preventive and reactive measures to address this problem [11, 12, 13]. After this incident, we have developed a standard operating protocol (SOP) in our department so that such a complication is not repeatedagain. The SOP consists of the following. Preparation of drain1. If the drain is needed to be cut, it should be cut between the drain holes. The tubing will usually break at a weak point through a hole. Hence, if on the removal of drain, the end is through a hole, it is likely that the drain has broken.2. A habit should be developed to cut the same number of drain holes, whenever possible, in the drain tubing every time.3. A number of drain holes left inside the wound should always be documented. This helps in confirming the removal of the whole drain (not practically possible every time). 4. Care must be taken to leave drain tubing just inside the wound (the black marking dot that precedes the drain holes should not be visible). Once the skin closure is complete, the slack in the drain tubing is gently pulled back to bring the black marking dot to the skin surface. The ability of the drain to slide freely confirms that the drain is not accidentally sewn into the surgical wound. Removal of drain1. Check for the presence of a skin suture securing the drain before attempting its removal. If the drainis secured with a skin suture, the suture should be cut first.2. Only a gentle force should be applied to remove the drain. Attempts at drain removal should be abandoned when the patient becomes intolerant of the process.3. If there is any doubt regarding breakage of drain and retention of the residual drain pieces, X-rays can be helpful.
Conclusion
Retained drain fragment after arthroscopic surgery can stay silent for months. Hence, a high index of suspicion should be maintained by surgeons to detect such a complication at the earliest. We suggest that every arthroscopic surgeon should follow a standard protocol while inserting and removing the drain to avoid this mistake.
Clinical Message
Insert and remove drains with caution. A high index of suspicion should be maintained by surgeons to detect breakage and retention of broken drain fragment at the earliest. Arthroscopic retrieval of broken drain fragment is a viable option.
References
1. Zeide MS, Robbins H. Retained wound suction-drain fragment. Report of 7 cases. Bull Hosp Joint Dis 1975;36(2):163-169.1. Zeide MS, Robbins H. Retained wound suction-drain fragment. Report of 7 cases. Bull Hosp Joint Dis 1975;36(2):163-169.
2. Jaafar S, Vigdorchik J, Markel DC. Drain technique in elective total joint arthroplasty. Orthopedics 2014;37(1):37-39.
3. Lysholm J, Tegner Y. Knee injury rating scales. Acta Orthop 2007;78(4):445-453.
4. Willett KM, Simmons CD, Bentley G. The effect of suction drains after total hip replacement. J Bone Joint Surg Br 1988;70(4):607-610.
5. Adalberth G, Byström S, Kolstad K, Mallmin H, Milbrink J. Postoperative drainage of knee arthroplasty is not necessary: Arandomized study of 90 patients. Acta Orthop Scand 1998;69(5):475-478.
6. Ashraf T, Darmanis S, Krikler SJ. Effectiveness of suction drainage after primary or revision total hip and total knee arthroplasty. Orthopedics 2001;24(12):1158-1160.
7. Matsuda K, Nakamura S, Wakimoto N, Kobayashi M, Matsushita T. Drainage does not increase anemia after cementless total hip arthroplasty. Clin Orthop Relat Res 2007;458:101-105.
8. Clifton R, Haleem S, McKee A, Parker MJ. Closed suction surgical wound drainage after hip fracture surgery: A systematic review and meta-analysis of randomised controlled trials. Int Orthop 2008;32(6):723-727.
9. Gaines RJ, Dunbar RP. The use of surgical drains in orthopedics. Orthopedics 2008;31(7):702-705.
10. Kim YH, Cho SH, Kim RS. Drainage versus nondrainage in simultaneous bilateral total hip arthroplasties. J Arthroplasty 1998;13(2):156-161.
11. Hak DJ. Retained broken wound drains: A preventable complication. J Orthop Trauma 2000;14(3):212-213.
12. Lazarides S, Hussain A, Zafiropoulous G. Removal of surgically entangled drain: Anew original non-operative technique. Int J Curr Med Sci Pract2003;10(1):63-64.
13. Namyslowski J, Halin NJ, Greenfield AJ. Percutaneous retrieval of a retained Jackson-Pratt drain fragment. Cardiovasc Intervent Radiol 1996;19(6):446-448.
14. Tammelleo AD. Piece of Penrose drain left in patient: Accidentaland Intentional distinction. Regan Rep Med Law 1996;29:3.
 |
 |
 |
 |
| Dr. Ravi Gupta | Dr. Anubhav Malhotra | Dr. Munish Sood | Dr. Gladson David Masih |
| How to Cite This Article: Gupta R, Malhotra A, Sood M, Masih GD. Retained Drain after Anterior Cruciate Ligament Surgery: A Silent Threat to an Athlete’s Career: A Case Report. Journal of Orthopaedic Case Reports 2017 Jul-Aug;7(4):10-12 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


