
[box type=”bio”] What to Learn from this Article?[/box]
High index of suspicion for septic arthritis should be borne in mind especially in complex patients such as IV drug users presenting with vague history.
Case Report | Volume 7 | Issue 6 | JOCR November – December 2017 | Page 13-15| Anantha Krishnan Raghupathi, Avinash Joshi. DOI: 10.13107/jocr.2250-0685.928
Authors: Anantha Krishnan Raghupathi [1], Avinash Joshi [2]
[1] Department of Orthopaedics, Southend University Hospital, Southend – On-Sea, United Kingdom,
[2] Department of Orthopaedics, Princess Elizabeth Hospital, St Andrews, Guernsey, United Kingdom.
Address of Correspondence:
Dr. Anantha Krishnan Raghupathi,
Department of Orthopaedics, Southend University Hospital, Southend – On-Sea, United Kingdom.
E-mail: krishananth@hotmail.com
Abstract
Introduction: Septic arthritis of the hip is a rare entity in acute presentation of hip pain in adults. Even though hip is the second most commonly affected joint, adult patients with septic arthritis not related to a surgical procedure represent <0.00001% of total acute admissions.
Case Report: We present a 32-year-old female intravenous drug abuser, positive for Hepatitis B and C who had started to inject her femoral veins 2 years ago. She presented with a 10 weeks history of radiating pain in the leg which was full, constant and diffuse in nature with hip stiffness. She was treated for sciatica by her GP. She had later visited A and E twice (5 and 8 weeks) and was again treated symptomatically. She started to have increasing pain, hip stiffness, reduced mobility, and developed swelling of both legs extending upto groin medially. The patient was apyrexial throughout these visits. She did not have back/buttock pain. X-ray showed loss of joint space with evidence of articular surface destruction. Ultrasound showed no fluid collection inside the joint and deep vein thrombosis was ruled out. Hip joint was aspirated, and cultures grew Staphylococcus aureus from the aspirate. Flucloxacillin and fucidin were started as per hospital protocol. Skin traction was applied for pain relief with active hip movements as possible. Magnetic resonance imaging demonstrated complete joint destruction post-infective septic arthritis. After 8 weeks of antibiotics, inflammatory markers improved. Follow up X-ray showed complete ankylosis of hip joint, severe restriction of hip movements and was allowed weight bearing as possible.
Conclusion: Risk of septic arthritis should always be considered in mind when dealing with these cohorts of patients. Threshold for septic arthritis should be much lower especially in patients with complicated history, current or ex-drug abuser and presenting with vague symptoms. Early diagnosis, detection of organisms, specific targeted antibiotics, and joint wash out with a future consideration of total hip arthroplasty when the infection has settled will help patients resume their normal function.
Keywords: Septic arthritis, IV drug user, hip joint, ankylosis.
Introduction
Septic arthritis of the hip is a rare entity in acute presentation of hip pain in adults. Even though hip is the second most commonly affected joint, adult patients with septic arthritis not related to a surgical procedure represent <0.00001% of total acute admissions [1]. Intravenous drug abuse can cause a spectrum of hematogenous infections such as abscesses, phlebitis, endocarditis, and osteomyelitis. Most common organisms found in drug addict population are Staphylococcus aureus 41.5%, Pseudomonas aeruginosa36.8%, Streptococcus spp. 8.3%, Serratiamarcescens 5 %, and Gram-negative bacteria 2.3% [2, 3]. Bone and joint infections in patients with intravenous drug abusers are predominately caused by Gram-positive bacteria. S.aureus is the most common pathogen[4]. Drug addicts are at risk of developing epiphyseal aseptic bone necrosis, especially of the femoral head due to the obliteration of epiphyseal arteries secondary to hemolytic and thrombotic reasons. The first seems due to self-administration of distilled or saline water which is capable of inducing hemolysis. The second depends on the release of inert substances into the circulation such as talc, chalk, or marble dust used to cut the heroin[2, 5]. Drug abuse can cause hepatic disease which represents one of the possible etiological factors in the cause of osteonecrosis[6]. Other authors have later confirmed this connection between hepatic diseases and avascular necrosis of the femoral head [7, 8].
Case Report
We present a case report of an IV drug abuser who presented late with vague symptoms and later diagnosed to have septic arthritis of the hip. A 32-year-old female with a history of intravenous drug abuse for 17 years and who had started to inject her femoral veins 2 years ago was positive for Hepatitis B and C. She presented with a 10 weeks history of radiating pain in the leg which was dull, constant and diffuse in nature with hip stiffness. She was treated for sciatica by her GP. She had later visited A and E twice (5 and 8 weeks) and was again treated symptomatically. She started to have increasing pain, hip stiffness, reduce mobility and developed swelling of both legs extending upto groin medially. The patient was apyrexial throughout these visits. She did not have back/buttock pain.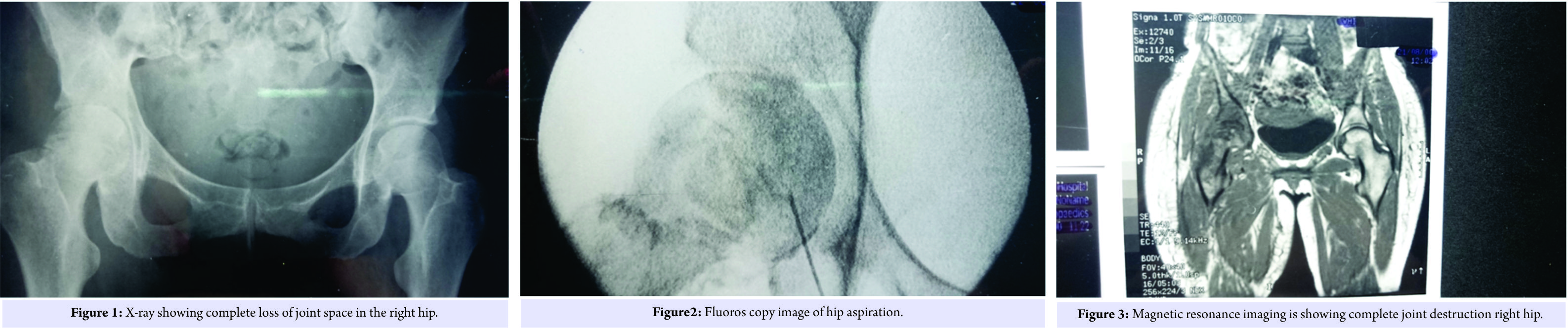
X-ray showed loss of joint space with evidence of articular surface destruction(Fig. 1). Ultrasound showed no fluid collection inside the joint and deep vein thrombosis was ruled out. Hip joint was aspirated with a small amount of fluid (Fig. 2). Cultures grew S. aureus from the aspirate. Flucloxacillin and fucidin were started as per hospital protocol. Skin traction was applied for pain relief with active hip movements as possible. Magnetic resonance imaging (MRI) demonstrated complete joint destruction post-infective septic arthritis (Fig. 3). After 8 weeks of antibiotics, inflammatory markers,i.e.,CRP reduced from 102 to 10 and ESR from 114 to 84. Follow-up X-ray showed complete ankylosis of hip joint, severe restriction of hip movements and patient was allowed weight bearing as possible.
Discussion
This patient being an IV drug abuser presented to her GP with vague symptoms quite late. Despite being presented to A and E twice, she did not have any investigations such as bloods or X-ray and was discharged. She developed hip ankylosis at a very young age due to late presentation and also delay in diagnosis due to non-specific symptoms. In this case, patient injected in her groin area thus creating a nidus for infection to attack periarticular soft tissue followed by hip joint leading to aseptic necrosis. A literature review using PubMed and medline between 1993 and 2017 gave a list of few articles which detailed the etiology, pathogenesis and treatment of septic arthritis in IV drug abusers but none had this peculiar vague presentation. Septic arthritis of the adult hip not associated with prior surgery is a rare but serious cause of acute hip pain which can lead to rapid joint destruction if diagnosis and treatment are delayed [9]. Munoz-Fernandez in 1993 studied about the incidence of septic arthritis in various joints in IV drug abusers. He found that there were 482 HIV positive and 85 HIV negative patients in his cohort of 567 patients. Osteoarticular infections were at the level of the hip (26%), sacroiliac (22%), sternocostal (19%), and knee (13%) [10]. Septic arthritis is treated with specific antibiotic therapy according to culture results and sensitivity to antibiotics. Drug users are generally hepatopathic immunocompromised patients and have a certain susceptibility to pathogenic infections that are multi-antibiotic resistant [2]. For patients with radiological signs of osteochondral involvement, extra-articular dissemination of infection or when the option for arthroscopic surgery is not available, open surgery with arthrotomy remains the treatment of choice. When severe destruction of hip is already present, joint preserving therapies are seldom successful, and Girdlestone’s procedure with two-step total hip arthroplasty is indicated [11, 12].
Conclusion
Therefore, we propose that high index of suspicion is necessary in complex patient’s, especially intravenous drug users. Risk of septic arthritis should always be considered in mind when dealing with these patients. Early diagnosis, detection of organisms, specific targeted antibiotics, and joint wash out with a future consideration of total hip arthroplasty when the infection has completely settled will help patients to resume their normal function sooner.
Clinical Message
Diagnosis can be difficult to reach in patients presenting with vague and complex history. Infection from superficial to deep including septic arthritis of the associated joint should be in our differential diagnosis. Detailed examination and early investigations can help to avoid complications and disability.
References
1. Schröder JH, Krüger D, Perka C, Hufeland M. Arthroscopic treatment for primary septic arthritis of the hip in adults. AdvOrthop 2016;2016:8713037.
2. Persiani P, Ranaldi FM, Mazza O, Calistri A, Bove M, Crostelli M, et al. Assessment and therapeutic choice in septic arthritis of the hip in an intravenous drug abuser: Case report at 14 years follow-up and review of literature. ClinTer 2017;168:e8-13.
3. Peterson TC, Pearson C, Zekaj M, Hudson I, Fakhouri G, Vaidya R, et al. Septic arthritis in intravenous drug abusers: A historical comparison of habits and pathogens. J Emerg Med 2014;47:723-8.
4. Allison DC, Holtom PD, Patzakis MJ, Zalavras CG. Microbiology of bone and joint infections in injecting drug abusers. ClinOrthopRelat Res 2010;468:2107-12.
5. Ozkunt O, Sarıyılmaz K, Sungur M, Ilen F, Dikici F. Bilateral avascular necrosis of the femoral head due to the use of heroin: A case report. Int J Surg Case Rep 2015;17:100-2.
6. Gómez-Mont Landerreche JG, Gil-Orbezo F, Morales-Dominguez H, Navarrete-Álvarez M, Trueba-Davalillo C, Capuano-Tripp P, et al.Nontraumatic causes of bilateral avascular necrosis of the femoral head: Link between hepatitis C and pegylated interferon. ActaOrtopMex 2015;29:172-5.
7. Seamon J, Keller T, Saleh J, Cui Q. The pathogenesis of non traumatic osteonecrosis. Arthritis 2012; 601763. Published online 2012 Nov 8 doi: 10.1155/2012/601763
8. Sameer MN, Edward YC. Epidemniology of osteonecrosis in USA. In: Osteonecrosis. Berlin Heidelberg: Springer; 2014. p. 39-45.
9. Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis? J Am Med Assoc 2007;297:1478-88.
10. Muñoz-Fernández S, Maciá MA, Pantoja L, Cardenal A, Peña JM, Martín Mola E, et al. Osteoarticular infection in intravenous drug abusers: Influence of HIV infection and differences with non drug abusers. Ann Rheum Dis 1993;52:570-4.
11. Rohde G, Klein W, Arinir U, Hagedorn M, Duerig N, T Bauer T, et al. Association of the ASP299GLY TLR4 polymorphism with COPD. Respir Med 2006;100:892-6.
12. Chen CE, Wang JW, Juhn RJ. Total hip arthroplasty for primary septic arthritis of the hip in adults. IntOrthop 2008;32:573-80.
 |
 |
| Dr. Anantha Krishnan Raghupathi |
Dr. Avinash Joshi |
| How to Cite This Article: Raghupathi AK, Joshi A. Late and Vague Presentation of Septic Arthritis of Hip in a IV Drug Abuser. Journal of Orthopaedic Case Reports 2017 Nov-Dec; 7(6): 13-15. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


