
[box type=”bio”] Learning Point for the Article: [/box]
Giant Cell Tumors should be kept in mind as a differential diagnosis for any lytic lesion even in uncommon places also the recurrence rate of efficiently curated lesions is very less.
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 29-31| Ashutosh R Mohapatra, Priyam Choudhury, Pranav S Patel, Rohit S Malhotra, Ankur B Patil. DOI: 10.13107/jocr.2250-0685.1144
Authors: Ashutosh R Mohapatra[1], Priyam Choudhury[2], Pranav S Patel[3], Rohit S Malhotra[4], Ankur B Patil[5]
[1]Department of Orthopedics, NMMC Hospital, Vashi, Mumbai, Maharashtra, India.
[2]Department of Radiology, Dr. D. Y. Patil Medical College, Pimpri, Pune, Maharashtra, India.
[3]Department of Orthopedics, Anand Multispeciality Hospital, Vadodara, Gujarat, India.
[4]Department of Orthopedics, ESIC Model Hospital, Baddi, Himachal Pradesh, India.
[5]Department of Orthopedics, Epping Tristar Medical Centre, Australia.
Address of Correspondence:
Dr. Dr. Pranav Patel,
A-4, Darpan Vatika, Laxmipura Road, Gorwa, Vadodara – 390 023, Gujarat, India.
E-mail: pranav.patel53@gmail.com
Abstract
Introduction: Giant cell tumors are common in proximal tibia and distal end radius and have a low tendency to recur. They have been treated successfully with excision and cementing or sandwich bone grafting without recurrence. Here, we present a rare case of giant cell tumor (GCT) of the distal tibia treated successfully with no recurrence at the end of 2 years.
Case Report: A 28-year-old female presented with complaints of pain and restricted movement of the right ankle joint since 1 month. There was no history of trauma. On examination, tenderness on the anterior aspect of the right ankle joint with restricted range of motion was found. X-rays revealed a well-defined expansile predominantly lytic lesion in the distal epi-metaphyseal region of the right tibia with minimal periosteal reaction seen along the medial margin. Magnetic resonance imaging revealed an ill-defined expansile lesion involving the epi-metaphyseal end of the lower end of tibia causing cortical breach and having extra-osseous tissue component with the abnormal signal in flexor and extensor group of muscles with the possibility of GCT. Surgery by excision, curettage, and cementation was performed to fill the defect. Histopathology of the tissue showed multinucleated giant cells with a uniform vesicular nucleus and mononuclear cells which were spindle shaped with uniform vesicular nucleus suggestive of GCT.
Conclusion: The patient at 2-year follow-up is doing well, walking without any pain, comfortably and with a full range of motion of the ankle joint with no signs of recurrence.
Keywords: Giant cell tumor distal tibia, giant cell tumor, curettage for giant cell tumor.
Introduction
Cooper in 1818 first described giant cell tumors (GCT) of the bone [1]. GCT represents approximately 5% of all primary bone tumors [2, 3]. More than half of these lesions occur in the third and fourth decades of life [3]. GCTs are benign tumors with potential for aggressive behavior and capacity to metastasize. Although considered to be benign tumors of bone, GCT has a relatively high recurrence rate. Metastases occur in 1–9% of patients with GCT and some earlier studies have correlated the incidence of metastases with aggressive growth and local recurrence [4, 5]. 90% of GCT exhibits the typical epiphyseal location [6, 7]. The most common locations, in decreasing order, are the distal femur, the proximal tibia, the distal radius, and the sacrum [8]. Involvement of the foot and ankle is rare and comprises <4% of all giant cell tumors (GCT) [9]. We present this case to highlight the rare location of GCT in the distal tibia which was treated successfully with no signs of recurrence.
Case Report
A 28-year-old female presented to us in July 2015 with complaints of pain and restricted movement of the right ankle joint since 1 month. The pain aggravated on walking. There was no history of trauma and was not associated with fever, loss of weight, or any other constitutional symptoms. History and family history were non-contributory. Clinical examination revealed no inspectory findings. Palpation revealed tenderness over the anterior aspect of the distal tibia with no local rise of temperature. Range of motion of the right ankle joint was painful and restricted. X-rays revealed a well-defined expansile predominantly lytic lesion in the distal epi-metaphyseal region of the right tibia with minimal periosteal reaction seen along the medial margin suggestive of malignant tumor of the bone (Fig. 1). Magnetic resonance imaging (MRI) of the right ankle joint suggested an ill-defined eccentric expansile lesion measuring 4.3 (CC) × 3.0 (transverse) × 2.9 (anteroposterior) involving epi-metaphyseal end of the lower end of tibia causing cortical breach and having extra-osseous tissue component with the abnormal signal in flexor and extensor group of muscles with the possibility of GCT (Fig. 2).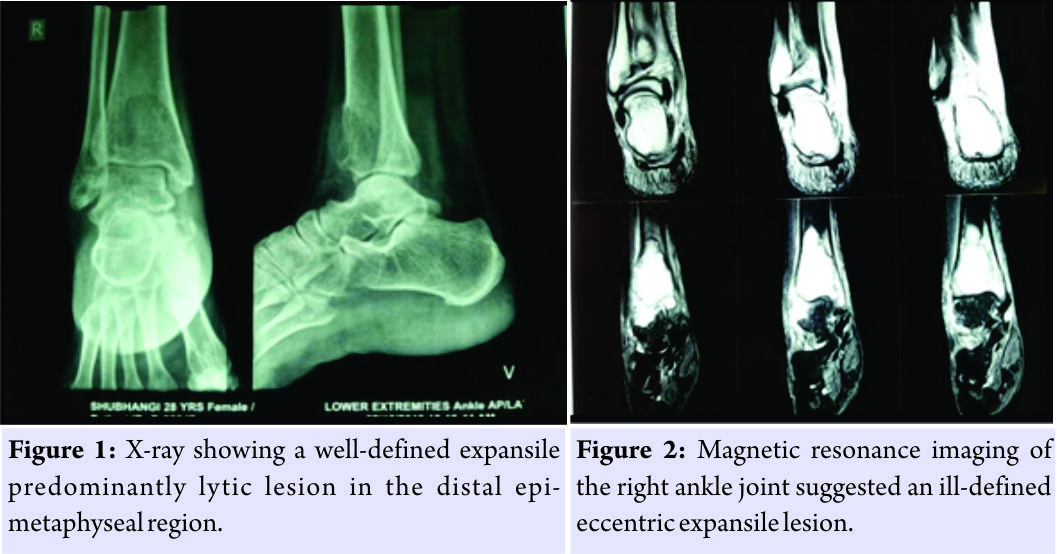 According to the radiological classification of campanacci the tumor was classified as a grade 3 lesions [1]. Laboratory investigations were within normal limits and surgery in the form of intralesional curettage with bone cement was planned. Anterior incision was taken over the distal end of the tibia. Bone was exposed, a cortical window of 3 cm × 2 cm was made (Fig. 3), the tumor was excised (Fig. 4), and curettage was done. The specimen was sent to histopathology for further examination. A thorough wash was given, and the defect was treated with 5% phenol. The cavity was filled with three layers consisting of bone graft, gel foam, and cement mixed with vancomycin, respectively (Fig. 5).
According to the radiological classification of campanacci the tumor was classified as a grade 3 lesions [1]. Laboratory investigations were within normal limits and surgery in the form of intralesional curettage with bone cement was planned. Anterior incision was taken over the distal end of the tibia. Bone was exposed, a cortical window of 3 cm × 2 cm was made (Fig. 3), the tumor was excised (Fig. 4), and curettage was done. The specimen was sent to histopathology for further examination. A thorough wash was given, and the defect was treated with 5% phenol. The cavity was filled with three layers consisting of bone graft, gel foam, and cement mixed with vancomycin, respectively (Fig. 5).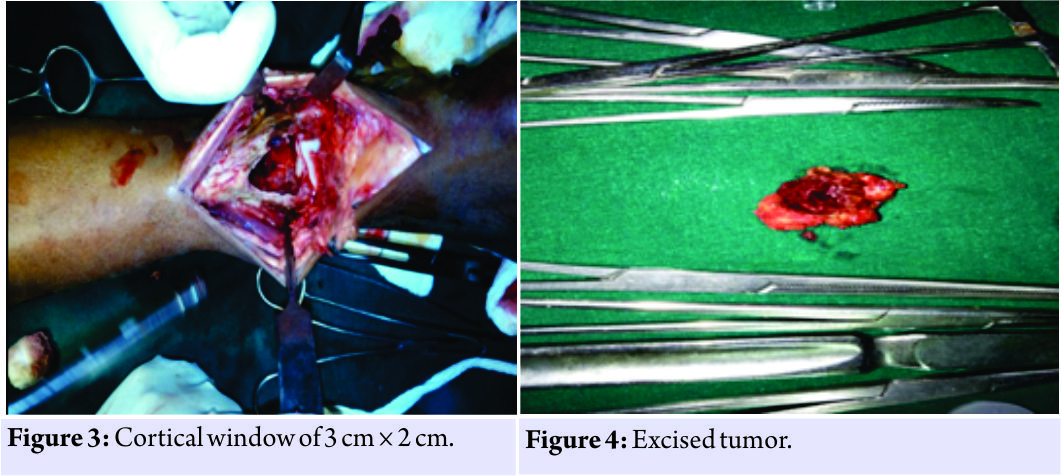 The tumor was sent for histopathological examination which confirmed the diagnosis of GCT (Fig. 6). X-rays were taken at regular follow-up to confirm the union and the cast was removed after 3 months postoperatively, and weight-bearing was started. The patient was followed up regularly with no signs of recurrence.
The tumor was sent for histopathological examination which confirmed the diagnosis of GCT (Fig. 6). X-rays were taken at regular follow-up to confirm the union and the cast was removed after 3 months postoperatively, and weight-bearing was started. The patient was followed up regularly with no signs of recurrence.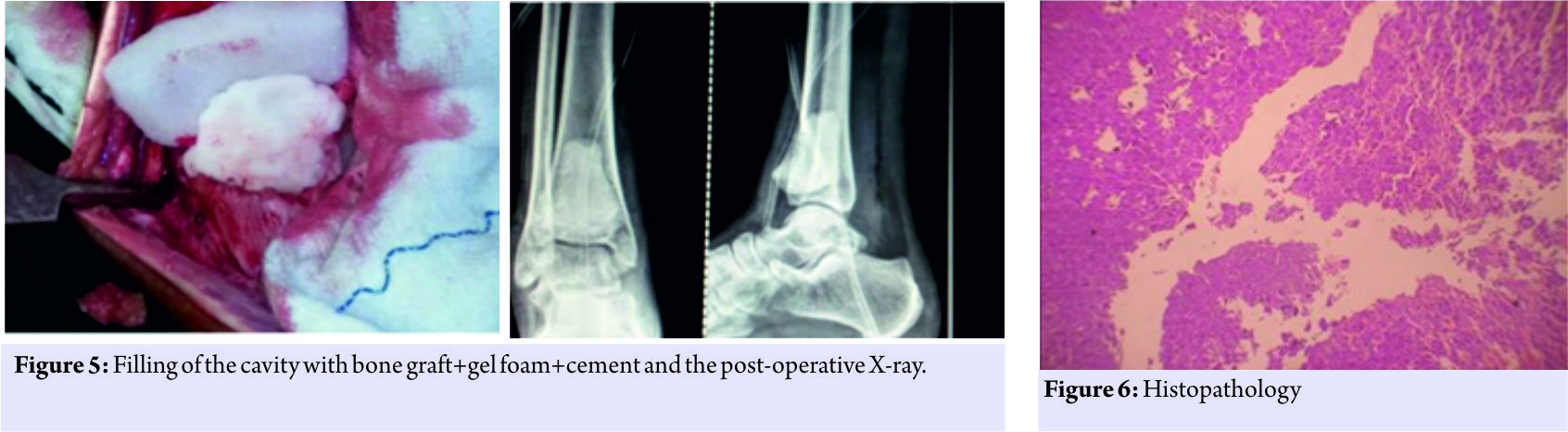
Discussion
Radiographic findings often are diagnostic [10]. As with any suspicious bone lesion, full staging with MRI, and computed tomography (CT) should be done [11]. The treatment of GCT is directed toward local control without sacrificing joint function. This has traditionally been achieved by intralesional curettage with autograft reconstruction by packing the cavity of the excised tumor with morsellized iliac corticocancellous bone. However, there are concerns regarding donor site morbidity (autograft), risk of disease transmission (allograft), and difficulty in visualizing (in X-rays) recurrence with grafts occupying the cavity. Regardless of how thoroughly performed, intralesional excision leaves microscopic disease in the bone, and hence, has a reported recurrence rate as high as 60% [12]. Cementation using methyl methacrylate has shown encouraging results and has the following advantages – methyl methacrylate monomer is cytotoxic, thermal effect – hyperthermia may help extend the boundary of tumor kill, radiographic detection of recurrence is easier, immediate structural support, and rapid weight-bearing ambulation [13]. Our patient belonged from a lower socioeconomic background and was the sole bread earner of her family. Returning to work was of utmost importance to her; hence, surgery in the form intralesional curettage with cementation was performed which yielded the desired results. Similar to our case, Madi et al. [14] and Bami et al. [15] too have reported good results with bone cement in the treatment of GCT of the distal tibia.
Conclusion
Hence, we conclude that a patient of GCT of distal tibia was successfully treated with intralesional excision+ curettage and bone cement with no signs of recurrence after 2 years.
Clinical Message
Giant cell tumors should be kept in mind as a differential diagnosis of all lytic lesions. Although they are known to occur in the distal femur, the proximal tibia, the distal radius, and the sacrum, GCTs can also occur in a rare location like distal tibia as seen in our patient. Furthermore, excision, curettage, treatment of the lesion with phenol and finally filling with bone grafting and cementing gives excellent results and reduces the chances of recurrence.
References
1. Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am 2006;37:35-51.
2. Eckardt JJ, Grogan TJ. Giant cell tumor of bone. Clin Orthop Relat Res 1986;204:45-58.
3. McGrath PJ. Giant-cell tumour of bone: An analysis of fifty-two cases. J Bone Joint Surg Br 1972;54:216-29.
4. Bertoni F, Present D, Sudanese A, Baldini N, Bacchini P, Campanacci M, et al. Giant-cell tumor of bone with pulmonary metastases. Six case reports and a review of the literature. Clin Orthop Relat Res 1988;237:275-85.
5. Siebenrock KA, Unni KK, Rock MG. Giant-cell tumour of bone metastasising to the lungs. A long-term follow-up. J Bone Joint Surg Br 1998;80:43-7.
6. Hoeffel JC, Galloy MA, Grignon Y, Chastagner P, Floquet J, Mainard L, et al. Giant cell tumor of bone in children and adolescents. Rev Rhum Engl Ed 1996;63:618-23.
7. Shih HN, Hsu RW, Sim FH. Excision curettage and allografting of giant cell tumor. World J Surg 1998;22:432-7.
8. Osaka S, Toriyama S. Surgical treatment of giant cell tumors of the pelvis. Clin Orthop Relat Res 1987;222:123-31.
9. Cribb GL, Cool P, Hill SO, Mangham DC. Distal tibial giant cell tumour treated with curettage and stabilisation with an ilizarov frame. Foot Ankle Surg 2009;15:28-32.
10. Canale TS, editor. Campbell’s Operative Orthopaedics. 11th ed., Vol. 1. Ch. 21. New York, NY, USA: Mosby, Benign/Aggressive Tumors of Bone; 2007. p. 883-6.
11. Murphey MD, Nomikos GC, Flemming DJ, Gannon FH, Temple HT, Kransdorf MJ, et al. From the archives of AFIP. Imaging of giant cell tumor and giant cell reparative granuloma of bone: Radiologic-pathologic correlation. Radiographics 2001;21:1283-309.
12. Carrasco CH, Murray JA. Giant cell tumors. Orthop Clin North Am 1989;20:395-405.
13. Puri A, Agarwal M. Treatment of giant cell tumor of bone: Current concepts. Indian J Orthop 2007;41:101-8.
14. Sandesh M, Sandeep V, Monappa N, Sharath R. Recurrent giant cell tumour of distal Tibia: Case report and review of the literature. Ann Med Biomed Sci 2015;1:4-7.
15. Bami M, Nayak AR, Shreepad K, Kulkarni A, Gupta R. Giant cell tumor of lower end of tibia. Case Rep Orthop 2013;2013:429615.
 |
 |
 |
 |
 |
| Dr. Ashutosh R Mohapatra | Dr. Priyam Choudhury | Dr. Priyam Choudhury | Dr. Rohit S Malhotra | Dr. Rohit S Malhotra |
| How to Cite This Article: Mohapatra A R, Choudhury P, Patel P S, Malhotra R S, Patil A B. An Unusual Case of Giant Cell Tumor of the Distal Tibia. Journal of Orthopaedic Case Reports 2018. Jul-Aug ; 8(4): 29-31. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


