
[box type=”bio”] Learning Point of the Article: [/box]
The MRI is mandatory in diagnosing traumatic cervical disc herniation without bony involvement.
Case Report | Volume 9 | Issue 1 | JOCR January – February 2019 | Page 19-22 | Jean Marie Vianney Hope, Jean Claude Sane, Souleymane Diao, Mouhamadou Habib Sy. DOI: 10.13107/jocr.2250-0685.1290
Authors: Jean Marie Vianney Hope[1], Jean Claude Sane[2], Souleymane Diao[2], Mouhamadou Habib Sy[2]
[1]Department of Orthopedics and Trauma Surgery, Rwanda Military Hospital, University of Rwanda, East Africa.
[2]Department of Orthopedics and Trauma Surgery, Grand-Yoff General Hospital, Cheikh Anta Diop University of Dakar, Senegal.
Address of Correspondence:
Dr. Jean Marie Vianney Hope,
Orthopedic and Trauma Surgeon, Fellow West African College of Surgeons (FWACS), Rwanda Military Hospital, P.O. Box: 3377 Kigali, Rwanda.
E-mail: hopejmv@gmail.com
Abstract
Introduction: Many cases of cervical spinal disc herniation caused by sporting injury have been reported. Those cases generally accompanied high-energy trauma such as fractures and/or dislocations. The purpose is to present the case of spinal cord injury (SCI) due to cervical disc herniation without bony involvement caused by wrestling.
Case Report: We report a case of a 23-year-old man who sustained a cervical SCI during the wrestling competition. He was quadriplegic with no sensory or motor function preserved in sacral segments S4-S5. Conventional radiographs and computed tomography did not reveal bony abnormalities. Magnetic resonance imaging (MRI) showed a free herniated cervical disc severely compressing the spinal cord from central at C3/4 level. He underwent anterior cervical discectomy and interbody fusion using autologous iliac crest bone graft and fixation with the cervical plate. He made an eventful recovery, and 5 years later, he was playing at high competitive level.
Conclusion: Competitive wrestling-related injuries are quite high. Fortunately, the incidence of SCI among wrestlers is extremely low. Although rare, SCI due to cervical disc herniation without bony involvement is a serious debilitating injury that exerts a devastating effect on a wrestler from a physical, psychological, and socioeconomic point of view, and places an immense burden on society from a public health perspective. The MRI is the golden examination in diagnosing such lesion. The management comprises surgical decompression of neural elements, stabilization, and fusion to provide a higher recovery rate from cord damage to return to play. Wrestler who is completely pain free with full range of motion and strength may be eligible for return to play.
Keywords: Cervical disc herniation, discectomy, spinal cord injury, wrestling.
Introduction
Wrestling has been referred to as the most intense and physically demanding combat sport in which the risk of injury is quite high [1]. In our environment, wrestling is now a national sport, exceeding even football in popularity. Wrestling-related injuries most commonly affect the head, shoulders, knees, and skin. Cervical spine injuries usually occur when the head is forcibly moved from one position to another, the “whiplash” type injury. Many cases of cervical spinal disc herniation caused by sporting injury have been reported. Those cases generally accompanied high-energy trauma such as fractures and/or dislocations [2]. However, cervical spinal cord injuries (SCIs) rarely happen in the absence of bony involvement. In this study, we report the case of a 23-year-old man with SCI due to cervical disc herniation without bony involvement caused by wrestling.
Case Report
A 23-year-old wrestler sustained a cervical spine injury during the wrestling competition on March 15, 2008. He suddenly became paralyzed and was immediately taken to the hospital emergency department. He had no previous burners and stingers syndrome history or any significant medical history. On neurological examination, the neck was stiff. Deep tendon reflexes of both upper (bicipital and tricipital) and lower (patellar and Achilles) extremities were absent. Pathologic reflexes (Hoffman, Wartenberg, and Babinski) were negative. Bulbocavernosus reflex was negative. Anesthesia below C4 dermatome was present in bilateral upper and lower extremities. He was quadriplegic with no sensory or motor function preserved in sacral segments S4-S5. He showed Grade 0 muscle weakness of bilateral legs and below top of the shoulders. Pre-operative conventional radiographs (Fig. 1a) and computed tomography (CT) (Fig. 1b) of the cervical spine revealed no spinal canal stenosis and no fracture dislocations. Sagittal (Fig. 2a) and transversal (Fig. 2b) T1- and T2-weighted magnetic resonance images showed a free herniated cervical disc severely compressing the spinal cord from central at C3/4 level and no bleeding of the retropharyngeal space. Urgent surgery was performed. He underwent anterior cervical discectomy, interbody fusion using autologous iliac crest graft (AICG), and ventral stabilization using cervical plate (Fig. 3a). The patient was operated5 h post-injury. Adjuvant pre- and post-operative steroid was administered; he was put on methylprednisolone sodium succinate (Solumedrol 40 mg/2 ml) injection 2 times a day for 10 days. The patient was immobilized postoperatively with a rigid cervical collar for 3 weeks. The incision was with primary healing. Rehabilitation was systematic thereafter for 12 months. Radiographs of the cervical spine 3 years after surgery showed satisfactory bone healing (Fig. 3b). His neurological palsy gradually improved postoperatively. 6 months after surgery, he could walk without crutches. 5 years later, he was competing at high level.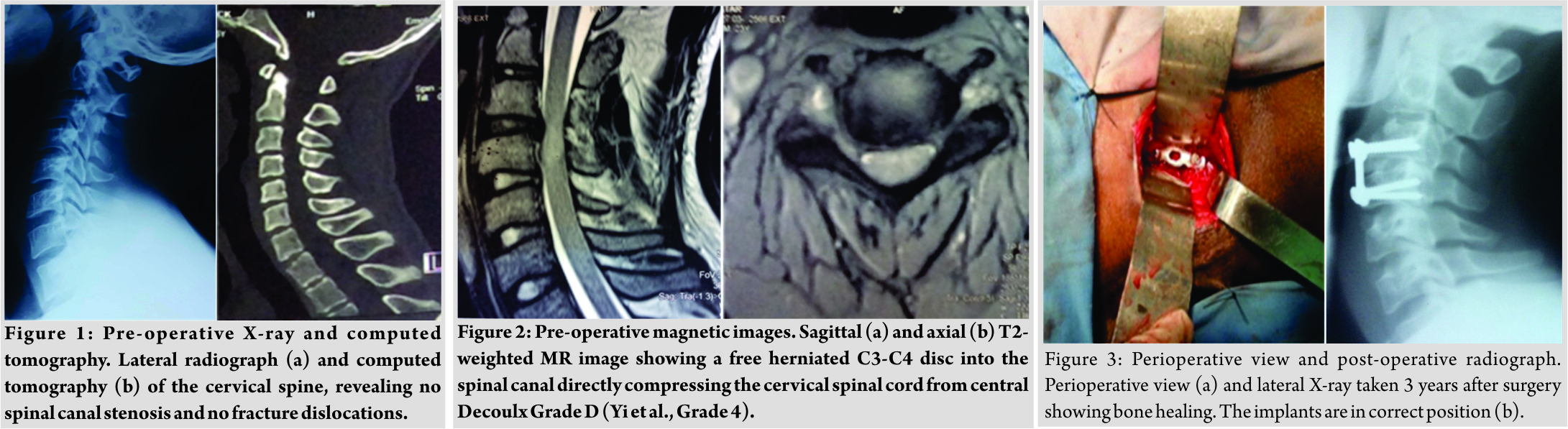
Discussion
Wrestling has been referred to as the most intense and physically demanding combat sport in which the risk of injury is quite high. Fortunately, the incidence of catastrophic injuries among wrestlers is extremely low. However, the great majority of severe injuries involve head and neck, and it is troubling to note the unusually high number of cervical spine injuries resulting from participation in wrestling. The vast majority of these are minor in nature[3, 4]. The current literature on sports injuries and health problems of wrestlers are mainly based on researches on high school and college wrestlers in the US [5, 6, 7, 8, 9]. We report a wrestler with a severe SCI due to cervical disc herniation. Many cases of cervical SCI due to disc herniation caused by sporting injury have been reported. Those cases generally accompanied high-energy trauma such as fractures and/or dislocations. However, cases of cervical SCI without bony involvement are caused by low-energy trauma like falls from standing height in the elderly. Suetsuna et al. [2] reported a case of SCI without bone lesion due to cervical disc herniation caused by bench pressing. Many factors have been identified as risk factors for SCI without spinal fractures such as spondylotic cervical spinal canal stenosis and ossification of posterior common vertebral ligament [10]. Our case is different from other cases previously reported. He is a young wrestler. He was previously healthy without history of burns and stingers syndrome. He has no risk factors, neither canal stenosis nor osteoarthritis of the cervical spine. The cervical SCI was the consequence of high-energy trauma without adjacent bony involvement. The sport involved is wrestling, and the mechanism of injury associated hyperextension to forced flexion, the “whiplash” injury. Plain X-rays and non-contrast CT scans are of little diagnostic value in isolated non-skeletal injuries of the cervical spine. Magnetic resonance imaging (MRI) is the golden modality for evaluation of cervical disc herniation [9]. In accordance with these findings, the value of MRI proved most useful in our case as conventional radiographs and CT were without abnormalities. In 1966, Decoulx has drawn up the anatomicoclinical classification of various stages of disc herniation without adjacent bone lesion. This classification distinguishes between four anatomical types. The Grade A is the disc prominence with permanent bulging. The Grade B is the non-exteriorized herniated disc. The Grade C is the exteriorized herniated disc. It is said to be of the “shirt button” type. The Grade D is the free herniated disc into the cervical canal [10]. Newly in 2015, Yi et al. [11] have described a four-grade system: Grade 1: Normal, Grade 2: Bulging, Grade 3: Protrusion, and Grade 4: Extrusion. Our case is graded Decoulxor Yi et al., Grade 4. Anterior cervical discectomy and interbody fusion (ACDF) have been proven to be an effective procedure for the treatment of patient with spinal cord compression due to herniated nucleus pulposus. However, the choice of fusion materials remains controversial. Some authors suggest discectomy, insertion of an intersomatic polyetheretherketone (PEEK) cage filled with synthetic bone [12]. Others prefer the use of AICG [13]. Chu et al. [14] have demonstrated that interbody cage fusion without plate fixation has a good fusion rate and neurological outcome. Lied et al. [15] evaluated the clinical outcome of ACDF in patient with cervical disc degeneration between fusions with an AICG versus fusion with an artificial cage made of PEEK. Due to similar clinical outcomes, the advantage of simplifying the surgery with a shorter duration of the procedure and lack of donor site morbidity when using PEEK, they suggested to prefer fusion with PEEK cage to AICG. In our context, as we did not dispose artificial cage made of PEEK, we have performed ACDF with AICG and stabilization with cervical plate.
Conclusion
Competitive wrestling-related injuries are quite high. Fortunately, the incidence of SCI among wrestlers is extremely low. Although rare, SCI due to cervical disc herniation without bony involvement is a serious debilitating injury that exerts a devastating effect on a wrestler from a physical, psychological, and socioeconomic point of view, and places an immense burden on society from a public health perspective. The MRI is the golden examination in diagnosing such lesion. The management comprises surgical decompression of neural elements, stabilization, and fusion to provide a higher recovery rate from cord damage to return to play. Wrestler who is completely pain free with full range of motion and strength may be eligible for return to play.
Clinical Message
All patients suffering from neurological symptoms after physically demanding combat sport accident such as wrestling, who have no evidence of a fracture and/or luxation on routine radiological examinations, should also be examined by MRI to detect cervical disc herniation.
References
1. Kordi R, Akbarnejad A, Wallace WA. Catastrophic injuries in the Olympic styles of wrestling in Iran. Br J Sports Med 2010;44:168-74.
2. Suetsuna F, Okudera Y, Tanaka T, Tamura T. Spinal cord injury due to cervical disc herniation caused by bench pressing. J Spine 2014;3:154.
3. Hutton MJ, McGuire RA, Dunn R, Williams R, Robertson P, Twaddle B, et al. Catastrophic cervical spine injuries in contact sports. Global Spine J 2016;6:721-34.
4. Perri BR, Lynch SA. Common injuries in the skilled wrestler. Curr Opin Orthop 2003;14:109-13.
5. Myers RJ, Linakis SW, Mello MJ, Linakis JG. Competitive wrestling-related injuries in school aged athletes in U.S. Emergency departments. West J Emerg Med 2010;11:442-9.
6. Rihn JA, Anderson DT, Lamb K, Deluca PF, Bata A, Marchetto PA, et al. Cervical spine injuries in American football. Sports Med 2009;39:697-708.
7. Hakkaku T, Nakazato K, Koyama K, Kouzaki K, Hiranuma K. Cervical intervertebral disc degeneration and low cervical extension independently associated with a history of stinger syndrome. Orthop J Sports Med 2017;5:2325967117735830.
8. Clark AJ, Auguste KI, Sun PP. Cervical spinal stenosis and sports-related cervical cord neurapraxia. Neurosurg Focus 2011;31:E7.
9. Hisato T, Takaki K, Nanae A. MRI findings of traumatic cervical disc herniation. Orthop Traumatol 2011;60:424-8.
10. Jomin M, Lesoin F, Lozes G, Thomas CE 3rd, Rousseaux M, Clarisse J, et al. Herniated cervical discs. Analysis of a series of 230 cases. Acta Neurochir (Wien) 1986;79:107-13.
11. Yi JS, Cha JG, Han JK, Kim HJ. Imaging of herniated discs of the cervical spine: Inter-modality differences between 64-slice multidetector CT and 1.5-T MRI. Korean J Radiol 2015;16:881-8.
12. Hattou L, Morandi X, Lefebvre J, Le Reste PJ, Riffaud L, Hénaux PL, et al. Anterior cervical interbody fusion using polyetheretherketone cage filled with synthetic bone graft in acute cervical spine injury. Orthop Traumatol Surg Res 2017;103:61-6.
13. Joaquim AF, Hsu WK, Patel AA. Cervical spine surgery in professional athletes: A systematic review. Neurosurg Focus 2016;40:E10.
14. Chu CW, Kung SS, Tsai TH, Huang TY, Hwang SL. Anterior discectomies and interbody cage fusion without plate fixation for 5-level cervical degenerative disc disease: A 5-year follow-up. Kaohsiung J Med Sci 2011;27:524-7.
15. Lied B, Roenning PA, Sundseth J, Helseth E. Anterior cervical discectomy with fusion in patients with cervical disc degeneration: A prospective outcome study of 258 patients (181 fused with autologous bone graft and 77 fused with a PEEK cage). BMC Surg 2010;10:10.
 |
 |
 |
 |
| Dr. Jean Marie Vianney Hope | Dr. Jean Claude Sane | Dr. Souleymane Diao | Dr. Mouhamadou Habib Sy |
| How to Cite This Article: Hope J M V, Sane J C, Diao S, Sy M H. Spinal Cord Injury Due to Cervical Disc Herniation without Bony Involvement Caused by Wrestling – A Case Report. Journal of Orthopaedic Case Reports 2019 Jan-Feb; 9(1): 19-22. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


