
[box type=”bio”] Learning Point of the Article: [/box]
Special reconstruoction techniques to face challenging Femoral Head Impaction fractures
Case Report | Volume 9 | Issue 1 | JOCR January – February 2019 | Page 65-69| Mauro Maniglio, Henrik Bäcker, Paolo Fornaciari, Peter Wahl, Emanuel Gautier. DOI: 10.13107/jocr.2250-0685.1312
Authors: Mauro Maniglio[1], Henrik Bäcker[2], Paolo Fornaciari[3], Peter Wahl[4], Emanuel Gautier[1]
[1]Department of Orthopaedics and Traumatology, HFR Fribourg Hopital cantonal, Fribourg, CH-1708, Switzerland,
[2]Department of Orthopaedics, Inselspital Universitatsspital Bern, Bern CH-3010, Switzerland,
[3]Department of Orthopaedics, Uniklinik Balgrist, Orthopedics, Zürich CH-8008,. Switzerland,
[4]Department of Orthopaedics, Kantonsspital Winterthur CH-8401 Winterthur, Switzerland.
Address of Correspondence:
Dr. Mauro Maniglio,
Department of Orthopaedics and Traumatology, HFR Fribourg Hopital cantonal, Chemin des pensionnats, Fribourg, CH-1708, Switzerland.
E-mail: maniglio.mauro@gmail.com
Abstract
Introduction: The combination of traumatic obturator dislocations and a femoral head impaction is rare and the treatment challenging. This report describes the successful management of this rare injury in a young patient.
Case Report: A 22-year-old truck driver involved in a ski accident sustained an obturator dislocation of the right hip associated with a femoral head impaction in the weight-bearing zone and a medial wall fracture of the acetabulum. After an initial closed reduction within 6 hours after the accident, for the definitive treatment, the hip joint was exposed through a Kocher-Langenbeck approach with trochanter flip osteotomy and surgical hip dislocation. A closing wedge intertrochanteric osteotomy was performed aiming to turn the head impaction out of the weight-bearing zone and the large head defect filled with the bone block removed from the osteotomy. The medial wall fragment was fixed, and the graft and osteotomies were stabilized with screws and a blade plate. The patient was mobilized with partial weight-bearing for 3 months then he progressively started full weight-bearing and normal daily activities. 5 years after the injury, the patient was completely asymptomatic, and radiographs demonstrated union of all osteotomies, osseous integration and remodeling of the bone graft as well as correct congruity of the hip joint.
Conclusion: The intertrochanteric osteotomy aims to turn the impacted zone out of the weight-bearing area. Bone grafting of the defect helps to restore congruence and containment of the hip and additionally reinforces the femoral neck. To manage all the lesions present, a trochanteric flip approach with surgical hip dislocation is mandatory.
Keywords: Femur head fracture-dislocation, obturator dislocation, Pipkin fracture, intertrochanteric osteotomy, trochanteric flip.
Introduction
Traumatic hip dislocation occurs as a result of high energy injuries. In 12% of the patients, the dislocation is combined with a femoral head fracture (complex dislocations) [1, 2] which could result in severe complications such as avascular necrosis (AVN) and subsequent early secondary osteoarthritis. Approximately 11% of all hip dislocations are anterior; of these, approximately 70% are obturator dislocations, comprising no more than 7% of all traumatic hip dislocations [3]. Indentation fractures of the femoral head have been reported to occur in 35%–55% of patients after traumatic obturator dislocation [3, 4, 5]. In general, the treatment of complex hip dislocations depends on the associated fracture (e.g., femoral head fracture, femoral neck fracture, and acetabular fracture). An obturator hip dislocation with a femoral head and a medial wall acetabular fracture is a very rare combination. Here, we report the long-term outcome of a young man treated with open reduction and internal fixation (ORIF) of the medial wall fracture, a valgus osteotomy of the femur and a restock of the impaction with autologous bone graft.
Case Report
A 22-year-old male truck driver was involved in a high-velocity ski accident. He sustained an obturator dislocation of the right hip associated with a severe femoral head impaction fracture in the weight-bearing zone and a medial wall fracture of the acetabulum (Fig. 1, 2, 3). 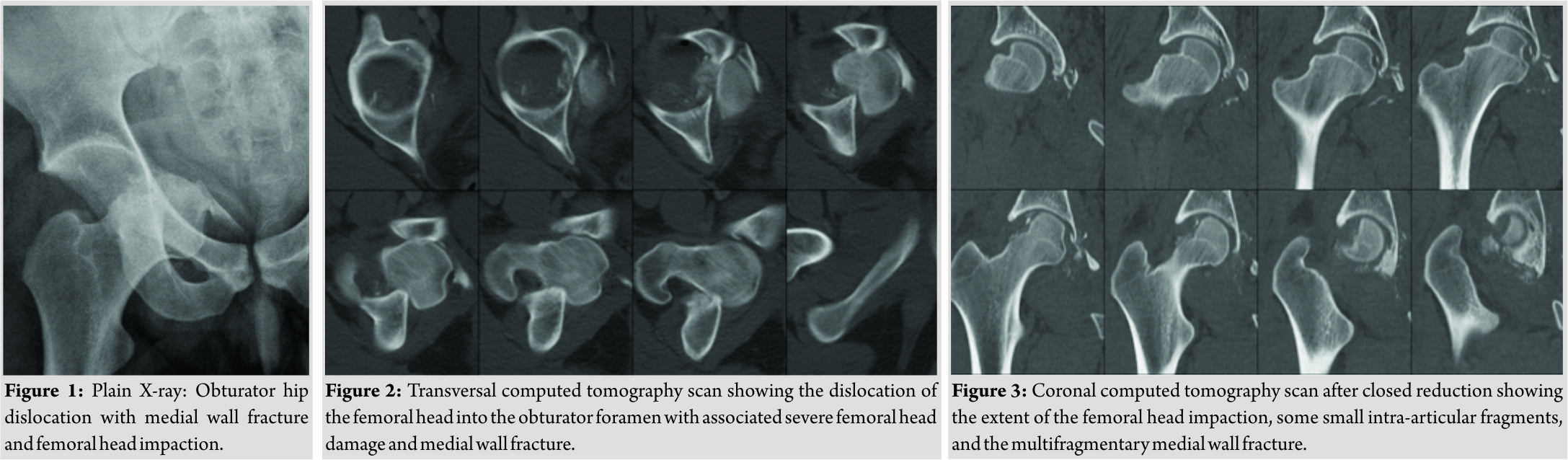 He was first transported to a regional hospital in a mountain region, the primary survey was done. Patient’s injuries include fractures of the spine (unstable Type B3 of the 5th and 6th thoracic (T) segments); the right scapula and an II° open comminuted fracture of the right olecranon. Concerning the right hip, the patient complained about right hip pain and an obvious deformity of the lower limb was present. A closed reduction of the right hip and an ORIF of the olecranon fracture were performed under general anesthesia within the 6 hours after the accident. The patient was referred to our hospital at the 4th day after the accident for further treatment of the spine and hip fractures. Due to the general status of the patient and the spine lesions needed to be treated reconstructive hip surgery was performed 17 days after injury in a lateral decubitus position under general anesthesia. The hip joint was exposed through a Kocher-Langenbeck approach with trochanter flip osteotomy [6, 7] and subsequent surgical hip dislocation [8, 9].
He was first transported to a regional hospital in a mountain region, the primary survey was done. Patient’s injuries include fractures of the spine (unstable Type B3 of the 5th and 6th thoracic (T) segments); the right scapula and an II° open comminuted fracture of the right olecranon. Concerning the right hip, the patient complained about right hip pain and an obvious deformity of the lower limb was present. A closed reduction of the right hip and an ORIF of the olecranon fracture were performed under general anesthesia within the 6 hours after the accident. The patient was referred to our hospital at the 4th day after the accident for further treatment of the spine and hip fractures. Due to the general status of the patient and the spine lesions needed to be treated reconstructive hip surgery was performed 17 days after injury in a lateral decubitus position under general anesthesia. The hip joint was exposed through a Kocher-Langenbeck approach with trochanter flip osteotomy [6, 7] and subsequent surgical hip dislocation [8, 9]. 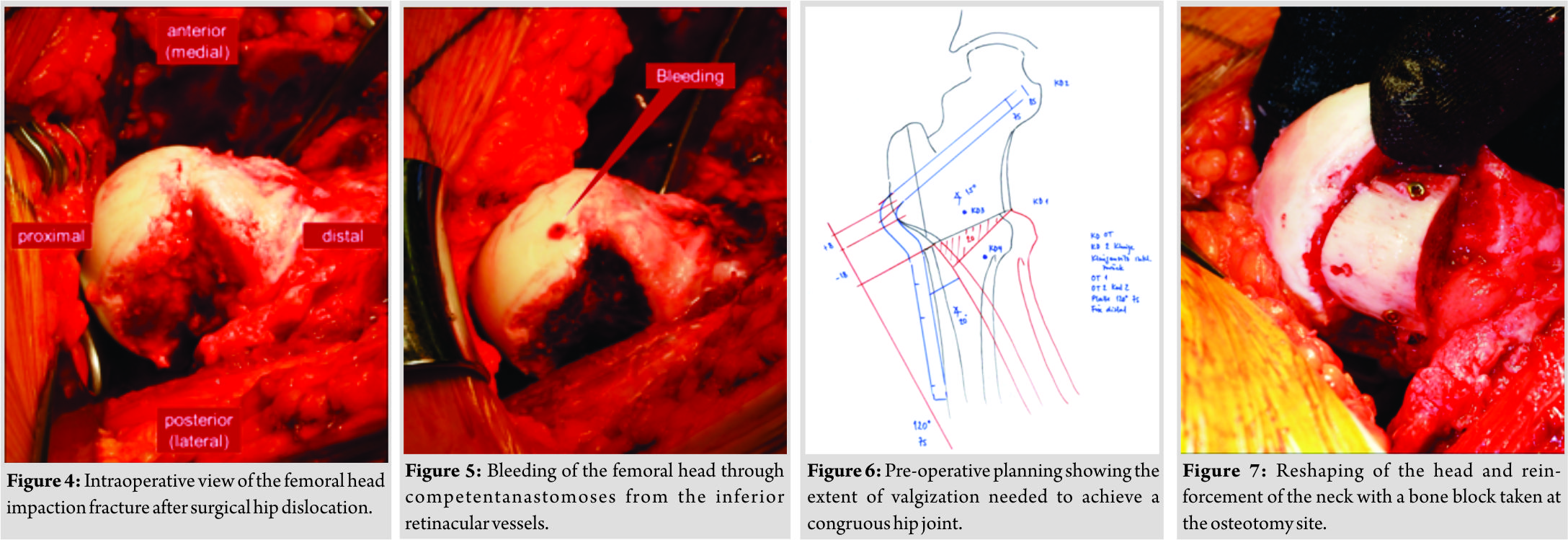 The local bone situation was assessed afterward: A large (2 cm × 2 cm × 1 cm) osseous head defect was present at the superior junction from head to neck, extending from anterior to posterior (Fig. 4) and the capital head ligament was still intact. Despite the complete destruction of the superior retinacular vessels due to the severe impaction at the head-neck junction active bleeding through intraosseous anastomoses from the inferior retinacular vessels was present after a hole of 1.5 mm was drilled in the femoral head (Fig. 5). A fracture of the medial wall with an associated labrum lesion was also present. After resection of the capital head ligament, the medial wall fragment with its adjacent labral avulsion was fixed with transosseous sutures and 3 bone anchors (Mitek, Depuy Synthes; 4528 Zuchwil Switzerland). Then, according to the pre-operative plan (Fig. 6) a 25° closing wedge intertrochanteric osteotomy was performed aiming to turn the head impaction out of the weight-bearing zone. The large head defect was filled with the reshaped bone block removed at the osteotomy site and stabilized with two 2 mm cortical screws (Fig. 7).
The local bone situation was assessed afterward: A large (2 cm × 2 cm × 1 cm) osseous head defect was present at the superior junction from head to neck, extending from anterior to posterior (Fig. 4) and the capital head ligament was still intact. Despite the complete destruction of the superior retinacular vessels due to the severe impaction at the head-neck junction active bleeding through intraosseous anastomoses from the inferior retinacular vessels was present after a hole of 1.5 mm was drilled in the femoral head (Fig. 5). A fracture of the medial wall with an associated labrum lesion was also present. After resection of the capital head ligament, the medial wall fragment with its adjacent labral avulsion was fixed with transosseous sutures and 3 bone anchors (Mitek, Depuy Synthes; 4528 Zuchwil Switzerland). Then, according to the pre-operative plan (Fig. 6) a 25° closing wedge intertrochanteric osteotomy was performed aiming to turn the head impaction out of the weight-bearing zone. The large head defect was filled with the reshaped bone block removed at the osteotomy site and stabilized with two 2 mm cortical screws (Fig. 7). 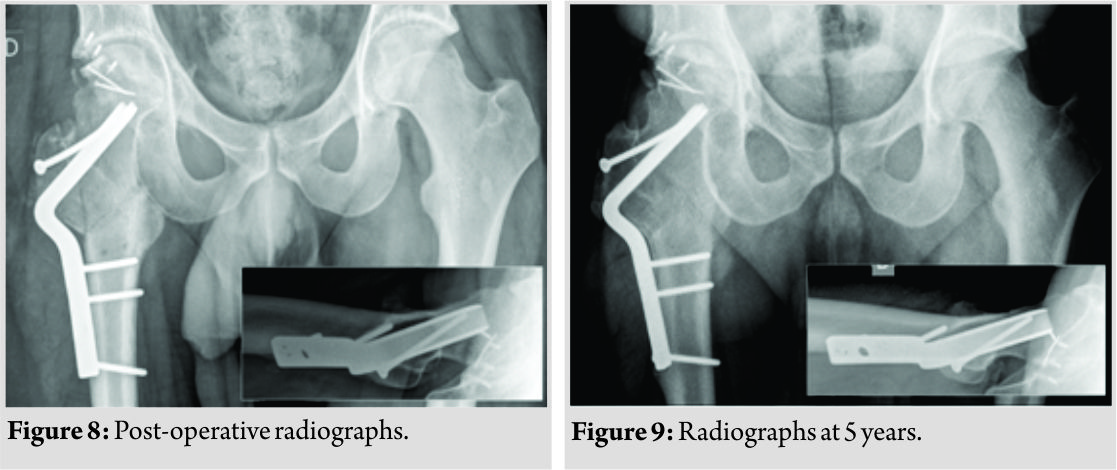 After head reduction, the intertrochanteric osteotomy was stabilized with a 120° blade plate (Depuy Synthes; 4528 Zuchwil Switzerland) and the trochanteric osteotomy with additional 4.5 mm lag screws (Fig. 8). For the first 3 post-operative months, the patient was mobilized on crutches with partial weight-bearing and active assisted mobilization of the hip in a lateral position under supervision by a physiotherapist. Radiographically, all osteotomies and fractures had united at 3 months, and the patient progressively started full weight-bearing and normal daily activities. At 5 months he was back to initial work as a truck driver. Asymptomatic, heterotopic ossification around the femoral head (Brooker Grade I) was seen. All his daily and recreational activities (Ski and Squash) could be restarted without any limitations. Satisfaction with the treatment was reported from the patient since the beginning. The hip mobility became a normal range after 6 months. At his most recent follow-up visit, 5 years after injury, the patient was very satisfied and completely asymptomatic. He had a symmetric range of motion of his hips and no limitations in daily and recreational activities. Radiographs demonstrated union of all osteotomies; osseous integration and remodeling of the bone graft as well as correct congruity and containment of the hip joint, without signs of osteoarthritis (Fig. 9, 10, 11). He was able to work 100% in his original profession. The Harris hip score was 98 points.
After head reduction, the intertrochanteric osteotomy was stabilized with a 120° blade plate (Depuy Synthes; 4528 Zuchwil Switzerland) and the trochanteric osteotomy with additional 4.5 mm lag screws (Fig. 8). For the first 3 post-operative months, the patient was mobilized on crutches with partial weight-bearing and active assisted mobilization of the hip in a lateral position under supervision by a physiotherapist. Radiographically, all osteotomies and fractures had united at 3 months, and the patient progressively started full weight-bearing and normal daily activities. At 5 months he was back to initial work as a truck driver. Asymptomatic, heterotopic ossification around the femoral head (Brooker Grade I) was seen. All his daily and recreational activities (Ski and Squash) could be restarted without any limitations. Satisfaction with the treatment was reported from the patient since the beginning. The hip mobility became a normal range after 6 months. At his most recent follow-up visit, 5 years after injury, the patient was very satisfied and completely asymptomatic. He had a symmetric range of motion of his hips and no limitations in daily and recreational activities. Radiographs demonstrated union of all osteotomies; osseous integration and remodeling of the bone graft as well as correct congruity and containment of the hip joint, without signs of osteoarthritis (Fig. 9, 10, 11). He was able to work 100% in his original profession. The Harris hip score was 98 points.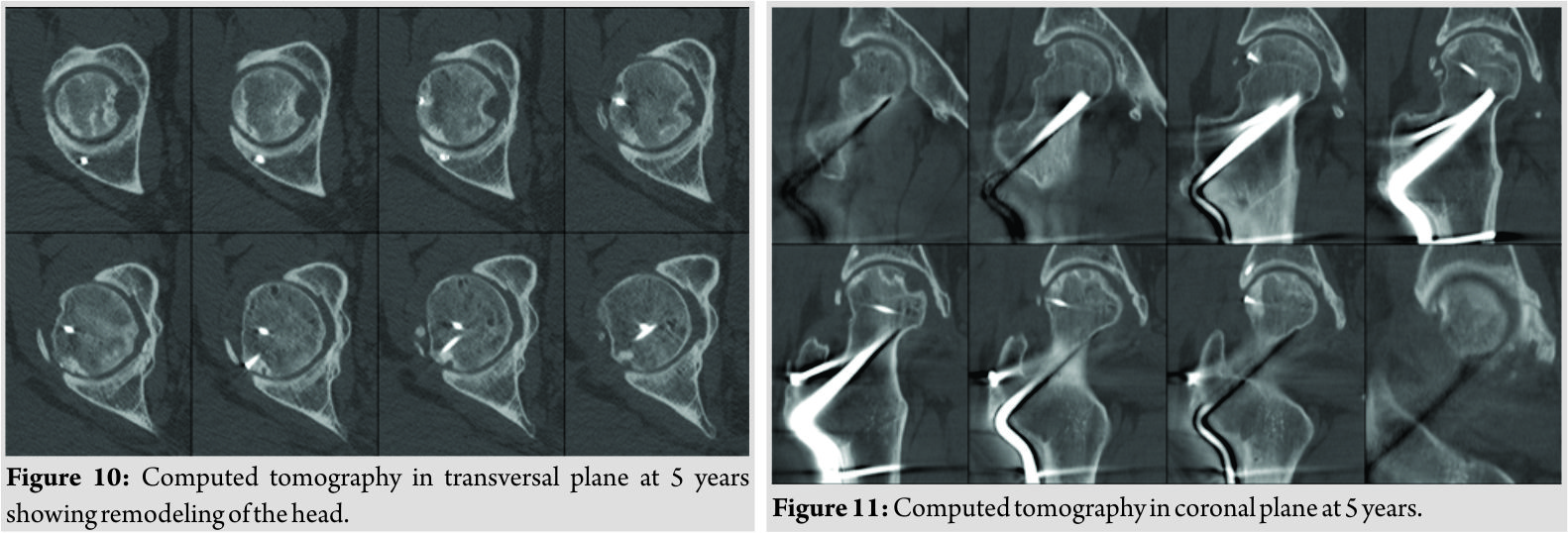
Discussion
The fracture dislocation presented here probably was provoked by a lateral force with impaction of the femoral head and medial wall fracture, followed by external rotation and an axial load resulting in the hip dislocation [10]. The incidence of a Type IV fracture, according to Pipkin [11] defined as combined femoral head and acetabular fracture is 7–14% of all traumatic hip dislocations in adults [11-13]. Only a few cases of indentation fracture of the femoral head [14] or neck [5, 15, 16] in a combination of an anterior hip dislocation have been described. To the best of our knowledge, this is the first case described combined with a medial wall acetabular fracture. Articular defects of the femoral head are often associated with early degenerative osteoarthritis and have serious consequences for the patient [17]. Especially, if it is combined with anterior hip dislocation, as AVN of the femoral head can appear due to disruption of the retinacular arteries that come from the medial circumflex artery [18]. Therefore, an emergency treatment is needed [12, 19]. To avoid some iatrogenic fractures, a gentle reposition (avoiding multiple attempts) has to be executed. If closed reduction fails, an open reduction of fracture-dislocations is needed. Depending on the extent and classification of the present injuries, both anterior and posterior approaches are recommended [12, 14]. We used a posterior Kocher-Langenbeck approach with a trochanteric flip osteotomy. Based on detailed anatomic studies of the blood supply [8], this approach provides complete visualization of the acetabulum and the femoral head, as well as a reduced risk of AVN. The external rotator muscles are not divided, and the medial femoral circumflex artery is protected by the intact external obturator. Due to the rare incidence of Type 4 Pipkin fractures, many aspects of the treatment are still controversial appreciated and different treatment options have to be evaluated on an individual basis [18, 20, 21]. Impacted femoral head fractures associated with obturator hip dislocation are usually treated non-operatively. In 5–27% of them, an ORIF may be performed [14, 20, 21, 22]. Large fragments cephalad to the fovea are involved in weight-bearing; therefore, a rigid fixation is needed to restore the articular congruence with the acetabulum. Numerous implants such as headless screws [22], countersunk lag screws [14, 23], suture anchors [22], and bio-absorbable pins [18] are available for this purpose. Even though prostetic is an excellent option for elderly patients having fractures with the large fragment of the weight-bearing surface [12], which cannot be satisfactorily fixed or for patients with neglected obturator hip dislocation [24], it is not recommended in young patients in whom joint preserving surgery is preferred. Therefore, we performed a closing wedge, valgus osteotomy to turn the involved impression zone out of the main weight-bearing articular surface and fill up the bone defect with autologous bone graft. We fixed the osteotomy with a blade plate. The wedge was used as a structural graft for the bone defect, avoiding donor site pain, or expensive artificial bone grafts costs. The medial wall was reconstructed using bone anchors and sutures. The osteotomy side and the fractures healed and the young patient recovered very well. He was completely asymptomatic in the last follow-up at 10 years post-surgery and resumed his daily and sports activities without any problem. This report describes the successful management of a rare injury to the femoral head combined with a medial wall fracture after obturator dislocation of the hip, in a young and active patient. In conclusion, the reader should keep in mind that, patients with a big impression fracture of the femoral head in the weight-bearing zone of the articulation, an osteotomy combined with an autogenous bone graft restock, could be a reliable treatment.
Conclusion
This report describes the successful management of a rare injury in a young and active patient. The intertrochanteric osteotomy aims to turn the impacted zone out of the weight-bearing area. Bone grafting of the defect helps to restore congruence and containment of the hip and additionally reinforces the femoral neck.
Clinical Message
To manage all the lesions present a trochanteric flip approach with surgical hip dislocation is mandatory.
References
1. Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C, et al. Management, complications and clinical results of femoral head fractures. Injury 2009;40:1245-51.
2. Laorr A, Greenspan A, Anderson MW, Moehring HD, McKinley T. Traumatic hip dislocation: Early MRI findings. Skeletal Radiol 1995;24:239-45.
3. Erb RE, Steele JR, Nance EP Jr., Edwards JR. Traumatic anterior dislocation of the hip: Spectrum of plain film and CT findings. AJR Am J Roentgenol 1995;165:1215-9.
4. DeLee JC, Evans JA, Thomas J. Anterior dislocation of the hip and associated femoral-head fractures. J Bone Joint Surg Am 1980;62:960-4.
5. Rancan M, Esser MP, Kossmann T. Irreducible traumatic obturator hip dislocation with subcapital indentation fracture of the femoral neck: A case report. J Trauma 2007;62:E4-6.
6. Siebenrock KA, Gautier E, Ziran BH, Ganz R. Trochanteric flip osteotomy for cranial extension and muscle protection in acetabular fracture fixation using a Kocher-Langenbeck approach. J Orthop Trauma 1998;12:387-91.
7. Siebenrock KA, Gautier E, Ziran BH, Ganz R. Trochanteric flip osteotomy for cranial extension and muscle protection in acetabular fracture fixation using a Kocher-Langenbeck approach. J Orthop Trauma 2006;20:S52-6.
8. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U, et al. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-24.
9. Siebenrock KA, Gautier E, Woo AK, Ganz R. Surgical dislocation of the femoral head for joint debridement and accurate reduction of fractures of the acetabulum. J Orthop Trauma 2002;16:543-52.
10. Phillips AM, Konchwalla A. The pathologic features and mechanism of traumatic dislocation of the hip. Clin Orthop Relat Res 2000;123:7-10.
11. PIPKIN G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39-A:1027-42 passim.
12. Epstein HC, Wiss DA. Traumatic anterior dislocation of the hip. Orthopedics 1985;8:130, 132-4.
13. Marchetti ME, Steinberg GG, Coumas JM. Intermediate-term experience of pipkin fracture-dislocations of the hip. J Orthop Trauma 1996;10:455-61.
14. Richards BS, Howe DJ. Anterior perineal dislocation of the hip with fracture of the femoral head. A case report. Clin Orthop Relat Res 1988;228:194-201.
15. Esenkaya I, Görgeç M. Traumatic anterior dislocation of the hip associated with ipsilateral femoral neck fracture: A case report. Acta Orthop Traumatol Turc 2002;36:366-8.
16. Sadler AH, DiStefano M. Anterior dislocation of the hip with ipsilateral basicervical fracture. A case report. J Bone Joint Surg Am 1985;67:326-9.
17. Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: An integrated mechanical concept. Clin Orthop Relat Res 2008;466:264-72.
18. Hermus JP, Laan CA, Hogervorst M, Rhemrev SJ. Fixation of a pipkin fracture with bio-absorbable screws. Case report and a review of the literature. Injury 2005;36:458-61.
19. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip 1987;1987:181-206.
20. Chiron P, Lafontan V, Reina N. Fracture-dislocations of the femoral head. Orthop Traumatol Surg Res 2013;99:S53-66.
21. Tonetti J, Ruatti S, Lafontan V, Loubignac F, Chiron P, Sari-Ali H, et al. Is femoral head fracture-dislocation management improvable: A retrospective study in 110 cases. Orthop Traumatol Surg Res 2010;96:623-31.
22. Lim BH, Jang SW, Park YS, Lim SJ. Open repair and arthroscopic follow-up of severely delaminated femoral head cartilage associated with traumatic obturator fracture-dislocation of the hip. Orthopedics 2011;34:199.
23. Droll KP, Broekhuyse H, O’Brien P. Fracture of the femoral head. J Am Acad Orthop Surg 2007;15:716-27.
24. Pankaj A, Sharma M, Kochar V, Naik VA. Neglected, locked, obturator type of inferior hip dislocation treated by total hip arthroplasty. Arch Orthop Trauma Surg 2011;131:443-6.
 |
 |
 |
 |
 |
| Dr. Mauro Maniglio | Dr. Henrik Bäcker | Dr. Paolo Fornaciari | Dr. Peter Wahl | Dr. Emanuel Gautier |
| How to Cite This Article: Maniglio M, Bäcker H, Fornaciari P, Wahl P, Gautier E. Obturator Dislocation of the Hip with Associated Femoral Head Impaction and Medial Wall Fracture of the Acetabulum. Journal of Orthopaedic Case Reports 2019 Jan-Feb; 9(1): 65-69. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


