
[box type=”bio”] Learning Point of the Article: [/box]
Congenital hypertrophy of the intrinsic muscles of the foot is a rare condition that can cause significant pain for patients and treatment with debulking procedures carries a significant risk of complications.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 34-37 | Justin E Hellwinkel, Philip J York, Jason T Leaseburg, Kenneth J Hunt. DOI: 10.13107/jocr.2250-0685.1358
Authors: Justin E Hellwinkel[1], Philip J York[1], Jason T Leaseburg[2], Kenneth J Hunt[1]
[1]Department of Orthopaedics, University of Colorado School of Medicine, Denver, CO, USA.
[2]Department of Orthopaedics, Houston Methodist Specialty Physician Group, Nassau Bay, TX, USA.
Address of Correspondence:
Dr. Justin E Hellwinkel,
AO1, Room 4501, Department of Orthopaedics,12631 E 17th AveAurora, CO 80045-2527, USA.
E-mail: justin.hellwinkel@ucdenver.edu
Abstract
Introduction: Congenital hypertrophy of the intrinsic muscles of the foot is a rare disorder of unknown incidence characterized by unilateral muscular hypertrophy of one or more of the intrinsic muscles. Few cases have been reported in literature, many presenting with hypertrophy of a single muscle.
Case Report: A 12-year-oldCaucasian female with hypertrophy of all intrinsic muscles of the right foot present since birth presented with muscle imbalance resulting in hammer toe deformities of the second and third toes with the second toe crossing over the hallux. Our treatment consisted of the correction of the toe deformities without muscle debulking or excision.
Conclusions: Isolated congenital hypertrophy of muscles poses a unique challenge, particularly involving musculature of the foot. Indications for intervention include pain or functional impairment. Specific treatments should aim to address patient complaints with the understanding that debulking procedures carry the risk of abundant scar formation, neurovascular injury, and functional deficits.
Keywords: Congenital hypertrophy, Foot hypertrophy, Foot intrinsics.
Introduction
Congenital hypertrophy of the intrinsic muscles of the foot is a rare condition with little understood about its etiology. In 1980, a multicenter review of 2720 lesions of the feet, not one case was of congenital hypertrophy [1]. Since the first documented case reported by Jahss in 1974, there have been only eight similar reported cases by our search of literature [2, 3, 4, 5, 6, 7, 8, 9, 10]. The condition is characterized by unilateral idiopathic hypertrophy of one or more intrinsic muscles of the foot without associated hypertrophy of bone or other soft tissues. These findings suggest that it is a distinct syndrome, separate from other forms of hypertrophy in which there is bilateral, progressive hypertrophy, or unilateral hypertrophy that develops later in life and that involves all structures of the foot [11]. Congenital hypertrophy poses a diagnostic challenge, as hypertrophy of single or multiple muscle groups can simulate soft tissue tumors [5]. In addition, there have been reports of anomalous and accessory muscle bellies of the foot that can present similarly [12]. In addition, other non-muscular causes of soft tissue enlargement must be ruled out including vascular malformation, plantar fibromatosis, ganglion, and focal gigantism [2, 13]. Herein, we present a rare case of congenital hypertrophy along with a summary of previous cases to provide a framework for diagnosis and treatment of the disorder.
Case Report
A 12-year-oldotherwise healthy female presented with enlarged right foot with crossing over of her second toe to her hallux with weight-bearing, as well as significant pain at her second and third proximal interphalangeal (PIP) joints of approximately 6-month duration. She reported a resting pain in the toes of three to six and pain with ambulation and exercise of eight to 10 on a visual analog scale (VAS). Pain was most pronounced with weight-bearing and running and becoming progressively less tolerable for the patient over time. The enlargement had been present since birth requiring a shoe size larger than the contralateral. Non-tender enlargement was noted on all aspects of her right mid and forefoot with the second and third hammer toe deformities (Fig. 1). In addition, the third PIP was subluxed with pain on range of motion. 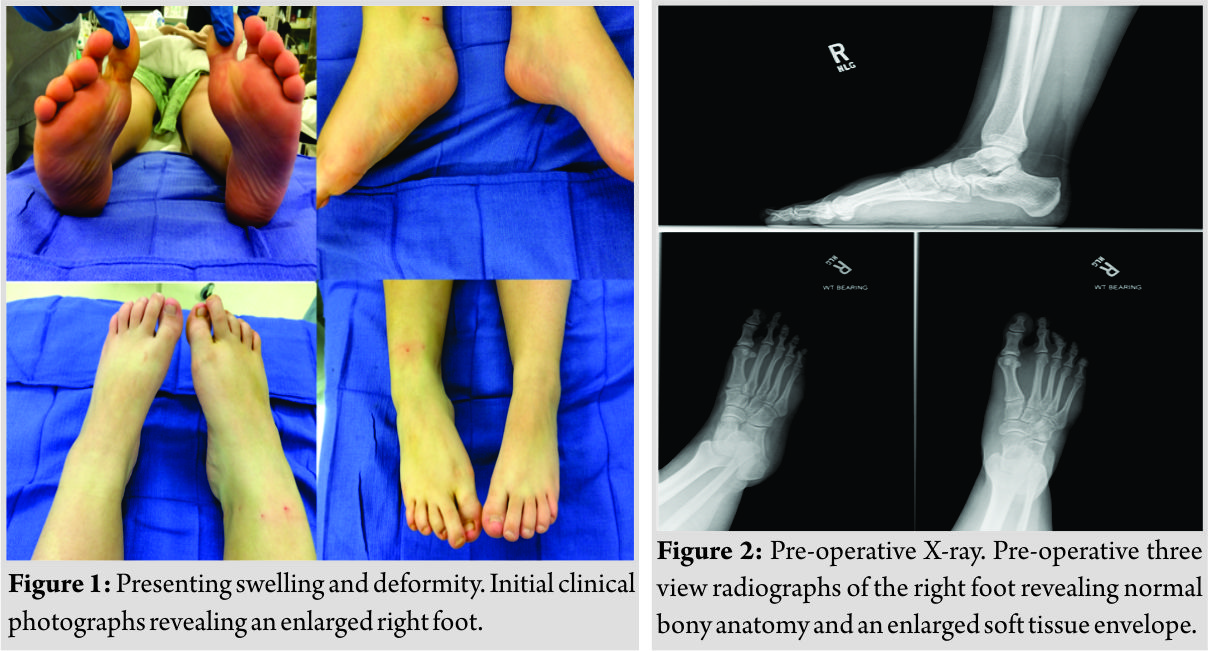 Radiographs revealed normal bony anatomy (Fig. 2). Amagnetic resonance imaging (MRI) was obtained revealing significant hypertrophy of all intrinsic muscles in the foot (Fig. 3).
Radiographs revealed normal bony anatomy (Fig. 2). Amagnetic resonance imaging (MRI) was obtained revealing significant hypertrophy of all intrinsic muscles in the foot (Fig. 3). 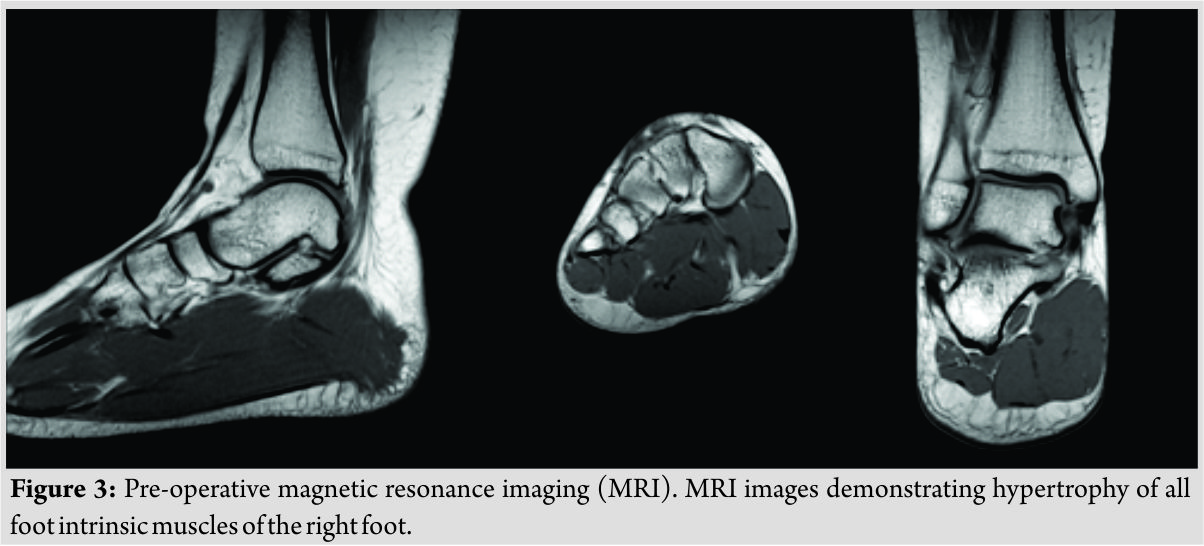 There was concern that a debulking procedure would have significant risk of nerve or vascular injury with substantial scar formation. As the hammer toe deformities and pain were the primary complaint, the attending surgeon suggested surgical management in the form of metatarsophalangeal joint release with extensor tendon lengthening and flexor to extensor tendon transfers without addressing the hypertrophy. In addition, the second and third PIP joint arthrodesis was performed to prevent deformity recurrence. The patient was made non-weight-bearing in a soft dressing. Sutures were removed at 2 weeks and pins removed at 6 weeks at which time the patient was allowed to weight bear as tolerated in a supportive shoe. At 4-month follow-up, the patient was pain free with no complaints and she was able to bear weight, ambulate, and complete her activities of daily living without issue (Fig. 4.). At 21-month follow-up, the patient was very satisfied with her toe positions and reported a decrease in pain on VAS to a resting level of zero and level of zero to three with prolonged activity, including running, which localized to the second and third digit (Fig. 5).
There was concern that a debulking procedure would have significant risk of nerve or vascular injury with substantial scar formation. As the hammer toe deformities and pain were the primary complaint, the attending surgeon suggested surgical management in the form of metatarsophalangeal joint release with extensor tendon lengthening and flexor to extensor tendon transfers without addressing the hypertrophy. In addition, the second and third PIP joint arthrodesis was performed to prevent deformity recurrence. The patient was made non-weight-bearing in a soft dressing. Sutures were removed at 2 weeks and pins removed at 6 weeks at which time the patient was allowed to weight bear as tolerated in a supportive shoe. At 4-month follow-up, the patient was pain free with no complaints and she was able to bear weight, ambulate, and complete her activities of daily living without issue (Fig. 4.). At 21-month follow-up, the patient was very satisfied with her toe positions and reported a decrease in pain on VAS to a resting level of zero and level of zero to three with prolonged activity, including running, which localized to the second and third digit (Fig. 5).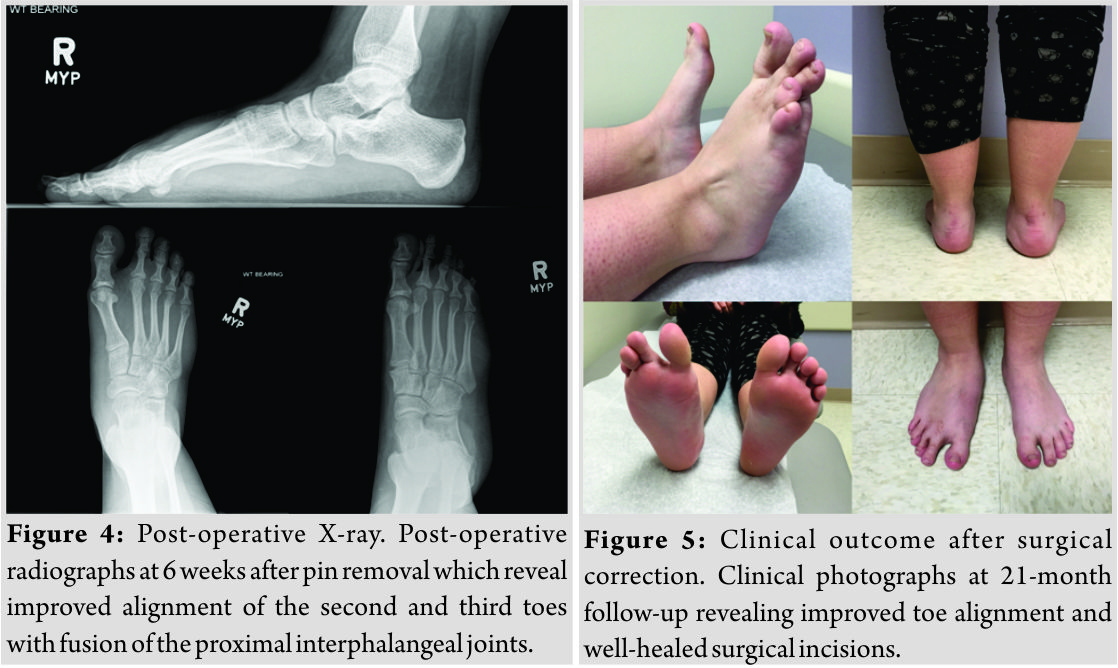
Discussion
Congenital hypertrophy is a rare disorder with nine previous cases reported in literature. Although these cases have similarities, it is impossible to know whether or not each of these cases represent the same pathology and some reports would tend to suggest some variation in presentation. There are, however, some common characteristics shared by most cases presented (Table 1).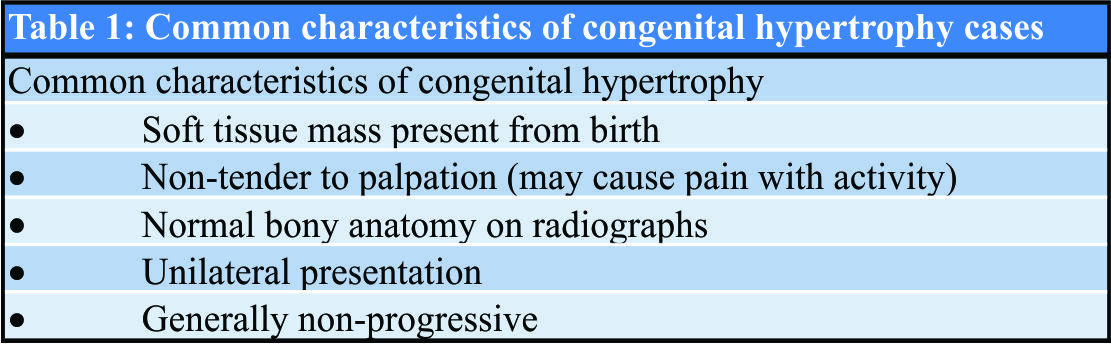
Presentation
The disorder has been documented in ages 4 months–33 years of age, has occurred in seven females and two males, and has occurred in equal rates in the left and right feet. Patients tend to present with foot asymmetry and varying degrees of pain or functional impairment, but the most common complaint has been difficulty with normal shoe wear. Each case has occurred in the absence of any other known congenital syndromes or disorders. Of the nine reported cases, five report hypertrophy of an isolated muscle belly (abductor hallucis in two cases [6, 10], abductor digiti minimi (ADM) in two cases [4, 5], and one case of isolated median head of the quadratus plantae [2]. The remaining four cases reported hypertrophy involving multiple muscle bellies. There is, uniformly, a visible, compressible soft tissue mass (Table 2). The youngest case reported by Shiraishi et al. of a 4-month-old boy was discovered due to an obvious size discrepancy between the child’s normal left foot and significantly larger right foot, although it was apparently asymptomatic [8]. Among the other reported cases, a majority reported that the soft tissue mass was non-tender to palpation (six of eight reports). Five cases reported that the mass had been present since birth [3, 4, 6, 8, 9], two reported that the mass had enlarged over a range of 7 months–10 years [7, 9], and the remainder did not specify.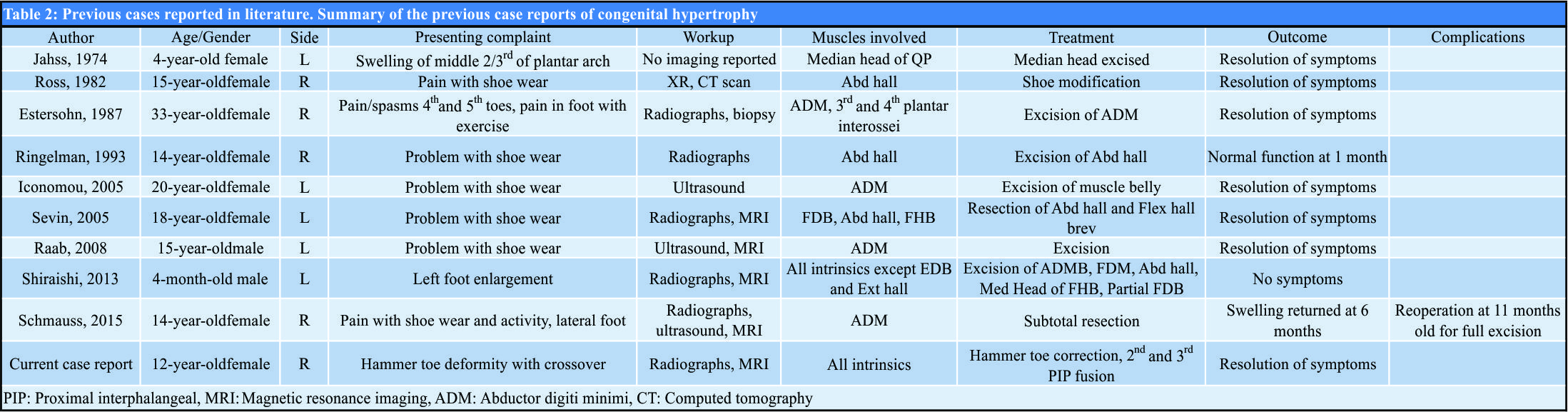
Workup
In the cases reported to date, the most common diagnostic pathway included physical examination, radiographic analysis, ultrasound, and, in most cases, MRI or computed tomography for confirmation. In the cases described, the muscle appeared completely normal both on ultrasound and MRI when obtained. However, it must be kept in mind that even if it is determined that the enlargement is due to hypertrophied muscle, there have been rare cases reported of the hypertrophy of muscles within a single extremity due to abnormal spontaneous electrical and mechanical activity -although this is appeared to be more generalized and progressive [14]. In general, it is felt that biopsy with histologic verification is not required in most cases [13],although if the diagnosis is not clear or if there is still concern for malignancy, then biopsy may be required. In five of the reported cases, intraoperative tissue samples were analyzed. The reports revealed muscle hypertrophy with focal areas of chronic myositis believed to be due to irritation in two cases [2, 5], hypertrophied muscle with areas of fibrosis, atrophy, and regeneration from stress in one case [6], and normal striated muscle tissue without abnormality in two cases [8, 9].
Treatment
Some have suggested that indications for intervention in cases of diagnosed congenital hypertrophy include functional impairment (including difficulty with shoe wear) or amelioration of pain and discomfort [4, 8]. While many would agree with the indication, the determination of how to intervene must take into account many variables. The condition clearly cannot be viewed as akin to other benign soft tissue masses for which excision or debulking might be relatively straightforward [15]. Removal of functional muscle tissue predisposes to potential motor imbalances or deficits and places the patient at risk of potential nerve injury resulting in local paralysis of muscle not excised in the procedure. In cases where a single or few muscles are involved, a reasonable treatment option may be excision or partial excision of the muscle of concern; however, the risk of significant scarring, nerve injury, and functional deficits needs to be considered. Clearly, as more muscles are involved this risk can increase to an unacceptable level and, in those cases, an alternative approach must be considered. Of the nine reported cases, eight patients underwent surgical excision of the involved muscle bellies, four of which were for excision of a single symptomatic muscle. However, each case requires careful thought and planning in relation to the presenting complaint. An alternative approach was successful in our case and in the case presented by Ross et al. reporting the successful treatment of a 15-year-old female athlete with hypertrophy of her right abductor hallucis with shoe modification alone [10].
Outcomes
In nearly all cases, patients reported satisfaction with the treatments described at follow-up ranging 1 month–3 years (mean = 13.1 months, two cases not specifying follow-up length). There were no reported complications in eight of the nine cases. The sole reported complication was by Schmauss et al. in which a 14-year-old female underwent subtotal resection of a hypertrophied ADM in an effort to maintain functionality of the muscle. Although at initial MRI this was the only muscle with noted hypertrophy, swelling comparable to her initial presentation returned by6-month post-operative which prompted a repeat MRI revealing persistent hypertrophy of ADM as well as the quadratus plantae and flexor digiti minimi brevis (FDMB). She underwent repeat operation to excise the remainder of ADM and partial excision of her FDMB. After the second procedure, she had resolution of her symptoms at 1 year with a normal-appearing MRI [7].
Conclusion
Congenital hypertrophy of the intrinsic muscles of the foot is a rare disorder of unknown prevalence but should be understood as a muscular hypertrophy that does not develop in response to some other disorder either of nerves, muscle, or extrinsic stimulus. While there has been no attempt to classify variations in the degree of muscular involvement, surgical excision of the involved muscles has been successful when a limited number of muscles were hypertrophied. We have presented a unique case of congenital hypertrophy in which all intrinsic muscles of the foot were involved and described a successful treatment strategy that targeted the patient’s unique complaints.
Clinical Message
Isolated congenital hypertrophy of the foot musculature is a unique disorder and treatment should be tailored to relieve specific patient symptoms rather than mass excision.
References
1. Berlin SJ. A review of 2,720 lesions of the foot. J Am Podiatry Assoc 1980;70:318-24.
2. Jahss MH. Pseudotumors of the foot. Orthop Clin North Am 1974;5:67-87.
3. Estersohn HS, Agins SW, Ridenour J. Congenital hypertrophy of an intrinsic muscle of the foot. J Foot Surg 1987;26:501-3.
4. Iconomou T, Tsoutsos D, Spyropoulou G, Gravvanis A, Ioannovich J.Congenital hypertrophy of the abductor digitiminimi muscle of the foot. Plast Reconstr Surg 2005;115:1223-5.
5. Raab P, Ettl V, Kozuch A, Nöth U. Hypertrophy of the abductor digitiminimi muscle simulating a localised soft tissue mass. Foot Ankle Surg 2008;14:43-6.
6. Ringelman PR, Goldberg NH. Hypertrophy of the abductor hallicus muscle: An unusual congenital foot mass. Foot Ankle 1993;14:366-9.
7. Schmauss D, Harder Y, Machens HG, Lohmeyer JA. Recurrence of hypertrophic abductor digitiminimi muscle of the foot after subtotal resection. J Foot Ankle Surg 2016;55:368-72.
8. Shiraishi T, Park S, Niu A, Hasegawa H. Congenital hypertrophy of multiple intrinsic muscles of the foot. J Plast Surg Hand Surg 2014;48:437-40.
9. Sevin AB, Deren O, Gençağa S, Adanali G, Erdoğan B, Kargi E, et al. Isolated unilateral hypertrophy of the plantar muscle: A case report. Foot Ankle Int 2005;26:767-70.
10. Ross JA, Lepow GM. The use of computerized tomography in the foot. J Foot Surg 1982;21:111-3.
11. Saunders N, Scheuller C. Progressive congenital hypertrophy of the feet. J Am Podiatr Med Assoc 1990;80:374-7.
12. Eberle CF, Moran B, Gleason T. The accessory flexor digitorum longus as a cause of flexor hallucis syndrome. Foot Ankle Int 2002;23:51-5.
13. Boothroyd AE, Carty H. The painless soft tissue mass in childhood-tumour or not? Postgrad Med J 1995;71:10-6.
14. Barron SA, Heffner RR Jr. Abnormal spontaneous electrical activity and gross enlargement of muscle. Arch Neurol 1983;40:515-8.
15. Simon MA, Finn HA. Diagnostic strategy for bone and soft-tissue tumors. J Bone Joint Surg Am 1993;75:622-31.
 |
 |
 |
 |
| Dr. Justin E Hellwinkel | Dr. Philip J York | Dr. Jason T Leaseburg | Dr. Kenneth J Hunt |
| How to Cite This Article: Hellwinkel J E, York P J, Leaseburg J T, Hunt K J. Congenital Unilateral Hypertrophy of the Foot Intrinsics: A Rare Case and Review of Literature. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 34-37. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


