
[box type=”bio”] Learning Point of the Article: [/box]
Superior dislocation of patella is a rare entity which must be distinguished from patellar tendon rupture and most cases can be managed with closed reduction using intramuscular analgesia.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 42-44 | Vivek Dubey, Pradeep A Sangnod, Ashwin Samant, Sunil M Shahane. DOI: 10.13107/jocr.2250-0685.1362
Authors: Vivek Dubey[1], Pradeep A Sangnod[2], Ashwin Samant[1], Sunil M Shahane[1]
[1]Department of Orthopaedics, HBT Medical College and Dr. R.N. Cooper Municipal General Hospital, Mumbai, Maharashtra, India,
[2]Department of Orthopaedics, ESIC Hospital, Andheri, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Vivek Dubey,
Room No. 305, RMO Quarters, Dr. R.N. Cooper Hospital, Mumbai–400 056, Maharashtra, India.
E-mail: vvk7878@gmail.com
Abstract
Introduction: Superior dislocation of patella is a rare injury. Patient usually presents with painful locking of the knee. The authors describe here a case of 54-year-male, who bumped his right knee on the edge of the bed. The patient was unable to extend his right knee. This was diagnosed as superior dislocation of patella and then managed with closed reduction with intramuscular analgesia.
Case Report: A 54-year-old male presented with acute painful locking of knee after his knee struck on the edge of the bed while trying to attain a kneeling position on the bed. On clinical examination, the superior pole of patella protruded anteriorly and was very tender. The patellar tendon was found to be intact. Radiographs confirmed the diagnosis of superior dislocation of patella. The dislocation was reduced by closed method using intramuscular analgesia. The knee was immobilized for three weeks in a posterior long knee brace.
Conclusion: Superior dislocation of patella is quite uncommon. High index of suspicion, mechanism of injury, clinical examination, and radiographs are helpful to arrive at the diagnosis. Immediate closed reduction provides pain relief and a good knee range of movements.
Keywords: Patellar dislocation, interlocking osteophyte, painful locking.
Introduction
Superior dislocation of the patella is a rare entity. The average age of these patients is 58 years (range 43–81 years) and the ratio of male-to-female cases is equal. The frequency of this condition is increasing given the degenerative nature of the underlying cause and the increasing elderly population in our society [1]. Superior dislocation of patella needs to be distinguished from ruptured patellar tendon. The mechanism of injury, clinical examination, and radiographs are vital to arrive at the diagnosis. Most of such cases are managed with closed manipulation under intramuscular analgesia.
Case Report
A 54-year-old man attended the emergency department of the hospital with a painful locking of the right knee. He was trying to attain a kneeling position on the bed when his knee struck on the edge of the bed. Clinical examination (Fig.1) revealed no palpable gap in the patellar tendon. The superior pole of the patella was projecting anteriorly and there was a prominent dimple below the patella. The patient was not able to perform straight leg raising. Plain radiographs (Fig. 2) confirmed a superior dislocation of the patella, which was manipulated by passing fingers under the prominent surface of patella, lower pole of patella was pushed posteriorly, and upper pole was pushed distally, gently flexing and then extending the knee which provided immediate pain relief. This procedure was done under the effect of intramuscular analgesia. The knee was then immobilized in a posterior long knee brace for three weeks. After three weeks, patient was active with pain-free range of movements and a stable right knee.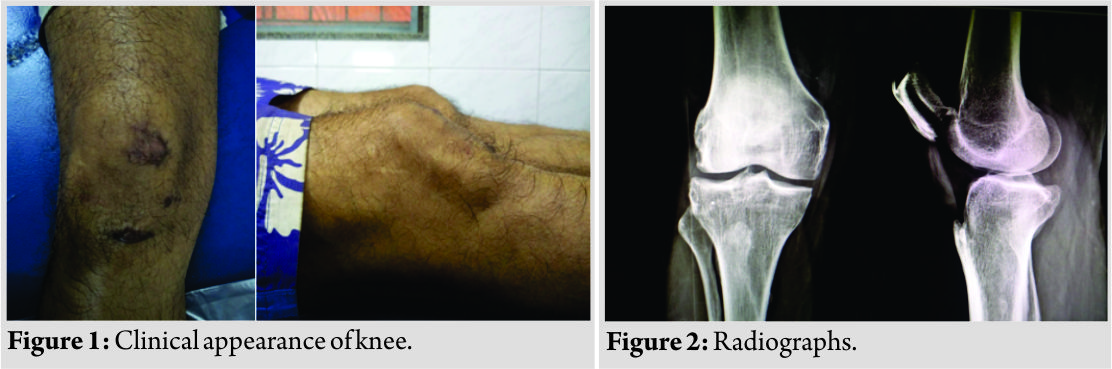
Discussion
Superior dislocation of the patella needs to be distinguished from patellar tendon rupture [2]. Both conditions cause an inability to perform straight leg raise. However, in the case of superior dislocation, the patellar tendon is intact. Also, the patella is invariably tilted anteriorly due to the locking osteophyte in superior dislocation of the patella with a characteristic dimple below the patella. The superior dislocation of the patella is a rare injury. It was first described by Watson Jones, in 1956. Since then, excluding this case, only 15 cases have been reported. The usual mechanisms of injury include direct impact on the patella, hyper extension of the knee joint, or a combination of the both [3, 4, 5, 6]. A characteristic of this condition is that the interlocking osteophytes prevent the spontaneous reduction of the proximally displaced patella [3, 7]. Hence, it is not uncommon to find marked osteoarthritic changes in the patellofemoral joint. Osteophytes over the inferior pole of the patella and the anterior femoral condyle are seen. These indicate knee osteoarthritis, which explains why the usual age presentation is between 50 and 60 years. Most patients with this injury can be treated non-operatively and surgical intervention is rarely indicated. Several methods of closed reduction have been proposed, including initial hyper extension of the knee joint followed by passive flexion or upward pressure over the patella and manipulation [8]. After the reduction, immobilisation is generally not required unless there are associated theoretical risk factors for recurrent dislocation. These include patella alta, ligamentous laxity, paralytic disorders, and preexisting genu recurvatum deformity [9]. After closed manipulation, it is safe to start mobilisation of the knee joint under the supervision of a physiotherapist. Our case, sustained the injury when he fell down while getting onto bed with direct impact on his right knee. He presented to us with painful locking. Closed reduction was performed under intramuscular analgesia which provided prompt pain relief. After immobilization for three weeks, patient had a stable knee and a good range of movements.
Conclusion
This case report highlights a rare injury of superior dislocation of the patella. The mechanism of which involves hyper extension or direct contusion onto the patella. It is important to distinguish this condition from patellar tendon rupture, which can be done by careful clinical assessment. After diagnosis, superior dislocation of the patella can be reduced closed with simple analgesia or sedation in most cases.
Clinical Message
Superior dislocation of patella without patellar ligament injury is a rare clinical condition. It needs to be distinguished from patellar tendon rupture. This injury on most of the occasions is managed with closed reduction using intramuscular analgesia.
References
1. Bassi RS, Kumar BA. Superior dislocation of the patella; a case report and review of the literature. Emerg Med J 2003;20:97-8.
2. Rao JP, Meese MA. Irreducible superior dislocation of the patella requiring open reduction. Am J Orthop (Belle Mead NJ) 1997;26:486-8.
3. Bartlett DH, Gilula LA, Murphy WA. Superior dislocation of the patella fixed by interlocked osteophytes. A case report and review of the literature. J Bone Joint Surg Am 1976;58:883-4.
4. Wimsatt MH, Carey EJ Jr. Superior dislocation of the patella. J Trauma 1977;17:77-80.
5. Hanspal RS. Superior dislocation of the patella. Injury 1985;16:487-8.
6. Friden T. A case of superior dislocation of the patella. Acta Orthop Scand 1987;58:429-30.
7. Teuscher DD, Goletz TH. Recurrent atraumatic superior dislocation of the patella: Case report and review of the literature. Arthroscopy 1992;8:541-3.
8. McWilliams TG, Binns MS. A locked knee in extension: A complication of a degenerate knee with patella Alta. J Bone Joint Surg Br 2000;82:890.
9. Takai S, Yoshino N, Hirasawa Y. Arthroscopic treatment of voluntary superior dislocation of the patella. Arthroscopy 1998;14:753-6.
 |
 |
 |
 |
| Dr. Vivek Dubey | Dr. Pradeep A Sangnod | Dr. Ashwin Samant | Dr. Sunil M Shahane |
| How to Cite This Article: Dubey V, Sangnod PA, Samant A, Shahane SM. Superior Dislocation of Patella – A RareClinicalEntity. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 42-44. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


