
[box type=”bio”] Learning Point of the Article: [/box]
Bilateral congenital Femur absence is an extreme form from congenital femur deficiency.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 19-21 | Pamudji Utomo, Hendra Cahya Kumara, Anung Budi Satriadi, Dita Anggara Kusuma. DOI: 10.13107/jocr.2019.v09i04.1460
Authors: Pamudji Utomo[1], Hendra Cahya Kumara[1], Anung Budi Satriadi[1], Dita Anggara Kusuma[1]
[1]Department of Orthopaedic and Traumatology, Faculty of Medicine, Sebelas Maret University, Professor Dr. R Soeharso Orthopaedic Hospital, Surakarta, Central Java, Indonesia.
Address of Correspondence:
Dr. Hendra Cahya Kumara,
Dr. R. Soeharso Orthopaedic Hospital, Jenderal Ahmad Yani Street, Pabelan, Surakarta, Central Java 57162, Indonesia.
E-mail: hendrack@gmail.com
Abstract
Introduction: Bilateral congenital absence of femur is a rare congenital anomaly.
Case Report: We report a 2-year-old Indonesian female child, the third of the birth of diabetic mother. There is no congenital abnormality among her siblings. She has a normal mentality and normal upper limbs. She was brought to us with a complaint of the short lower limb. Examination revealed short lower limb with an absence of thigh, a full range of motion of the hip and ankle and left club foot. A detailed history was obtained and she was radiologically examined. The X-ray of the pelvis and lower limb shows shallow of the acetabulum, absence of bilateral femur, and uncommon form of tibia fibula. She was diagnosed with bilateral congenital absence of femur.
Conclusion: We report this case because it does not meet the existing classification criteria for congenital femur deficiency. Proper evaluation and management of this case can help the patient and the parents to accept her condition and be able to live a good social and economically productive life.
Keywords: Congenital deformities, pediatric, rare case.
Introduction
Fetal growth and development of the lower extremities are controlled by a complex cascade of a multitude of growth factors that are expressed in a particular sequence and at various concentrations during development. Embryogenesis of the extremities occurs between 4 and 8 weeks after fertilization. Most limb deficiencies occur in this period of time, especially during rapid proliferation and differentiation of cells and tissues, peak during the 5th and 6th weeks after fertilization [1, 2]. Congenital defects of the femur vary from simple hypoplasia of the bone to complete absence. The clinical distinction between the various types of the femoral defect is important as a guide to the prognosis of limb development [3].
Case Report
A 2-year-old girl present with a complaint of a short stature. She was born at term by cesarean section to a 38-year-old gravida 3, para 2, abort 0 mother after an uncomplicated pregnancy. The baby was vigorous and starts to cry immediately after birth. The mother has a history of type 2 diabetic condition; insulin injection continued throughout pregnancy and glycemic control was reported to be normal during pregnancy. The mother was not related by blood to the patient’s father. There was no history of exposure to other teratogens. There is no congenital abnormality among her siblings. Physical examination showed a normal mental status with normal structure and function of the upper extremity. The patient can stand by her own but walk with walking aid. The patient seems short when compared to children of the same age; there is no leg length discrepancy. Local physical examination revealed an absence of both thigh and knee joint. There is no limitation of movement in both of hip joint and ankle. Both feet are normal. We did not observe any other anomalies in the skeleton or internal organs (Fig. 1). Plain X-ray examination of the pelvis and femur shows shallow of both acetabula, absence of both femurs, and uncommon form of both tibia fibulas. The proximal tibia is forming a proximal femur-like shape directly connect to the acetabulum (Fig. 2).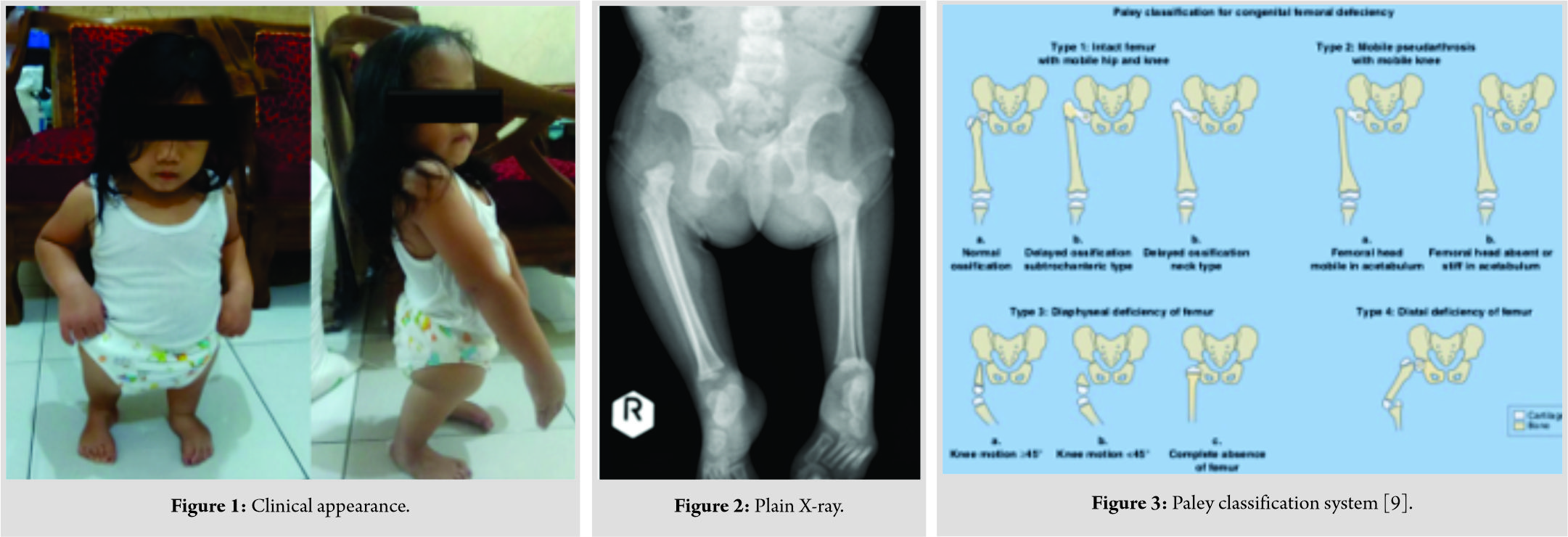
Discussion
Bilateral congenital absence of femur is a rare congenital anomaly and it is an extreme variant of congenital femur deficiency. These anomalies can occur singly or in associated with another anomaly such as fibular hemimelia (most common), clubfoot, an absence of lateral foot rays, congenital cardiac defects, or spinal dysplasia [4]. Other structure anomalies are often involved; these include the acetabulum, musculature, vessels, ligaments of the knee, tibia, fibula, and foot. Dysplasia of the acetabulum is progressive, whether initially present or not [1]. In our case, other anomalies associated with congenital femur absent are a shallow surface of both acetabulum and left club foot. Patient can standup straight and can walk with aid without hip pain. The specific cause of congenital femoral deficiencies or absence is unknown in most cases. Some of the abnormalities may cause by genetic base while others caused by an indirect effect of teratogen. This disorder is more common in females, same as our case [2, 5, 6]. Pregestational diabetic pregnancy, despite the improved metabolic control, is still a strong risk factor for alterations in fetal development, leading to fetal malformations [7]. The incidence of fetal structural defects caused by maternal pregestational diabetes is three- to four-fold higher than that caused by non-diabetic pregnancy [8]. Pregestational diabetic mother is identified as risk factor for the anomaly in our case. The classification by Aitken is widely used. This classification is based on the severity of the hip and femur radiographic findings. There are four classes in Aitken classification: Class A, short femur with most proximal ossified portion at or slightly above the acetabulum; Class B, more extensive defect or absence of the proximal femur, the acetabulum shows more signs of dysplasia than Class A; Class C, The acetabulum is severely dysplastic, femoral head is absent and not ossify with time. Femoral shaft is shorter than Class B; and Class D, the femoral shaft is essentially absent and the distal femoral condyles are seen at the level of where the acetabulum should be [5]. Aitken classification is descriptive but not helpful in treatment. Paley and Guardo [9] developed the classification system for congenital femur deficiency based on the factors that influence lengthening reconstruction (Fig. 3). The case presented here does not fulfill any classification above. There is a complete absence of femur with no sign of ossification and tibia-fibula complex is directly connected to the acetabulum. The proximal part of the tibia forms a proximal femur-like shape. The fact that the patient and her parents have no complaints other than her short stature makes further evaluation and management of this case can help the patient and the parents to accept her condition and be able to live a good social and economically productive life.
Conclusion
Congenital femur absence is an extreme form from congenital femur deficiency. This anomaly can occur singly or in associated with another anomaly such as fibular hemimelia (most common), clubfoot, an absence of lateral foot rays, congenital cardiac defects, or spinal dysplasia. There are several classifications for this anomaly, but nothing matches to our case. Further evaluation and management of this case can help the patient and the parents to accept her condition and be able to live a good social and economically productive life.
Clinical Message
Bilateral congenital femur absence is a rare congenital anomaly. We want to share this case because It does not meet the existing classification criteria for congenital femur deficiency. Proper evaluation and management based on clinical manifestation in essential to help the patients to get a good quality of life.
References
1. Paley D, Guardo F. Congenital femoral deficiency reconstruction and lengthening surgery. In: Sabharwal S, editor. Pediatric Lower Limb Deformities. Switzerland: Springer International Publishing; 2016. p. 361-425.
2. Herring JA. Limb deficiencies. In: Herring JA, editor. Tachdjian’s Pediatric Orthopaedics. 5th ed. Vol. 1. Philadelphia, PA: WB. Saunders; 2014. p. 951-74.
3. Ring PA. Congenital abnormalities of the femur. Arch Dis Child 1961;36:410-7.
4. Ukkali SB, Mahvish K.,Jeergal N., Congenital femoral deficiency: A rare case report. Int J Contemp Pediatr 2017;4:1118-21.
5. Bowen RE, Otsuka NY, Evans EL, Smith NR. The child with a limb deficiency. In: Weinstein SL, Flynn JM, editors. Lovell and Winter’s Pediatric Orthopaedics. 7th ed., Vol. 2. Philadelphia, PA: Lippincott Williams and Wilkins; 2014. p. 1526-95.
6. Omidi A, Sharifi N, Fazel A, Niazi A, Gharavian M. A case of bilateral agenesis of femur. Iran J Med Sci 2002;27:36-8.
7. Dodampahala SH, Wijerathne CN, Dodampahala RM, Gunathilaka WC. Prenatal detection of fetal anomalies and its prevalence by sonography in pregnancies complicated by pre-gestational diabetes mellitus. Acad Res J Biotechnol 2014;1:23-5.
8. Chen CP. Congenital malformations associated with maternal diabetes. Taiwan J Obstet Gynecol 2005;44:1-7.
9. Paley D, Guardo F. Lengthening reconstruction surgery for congenital femoral deficiency. In: Kocaoglu M, Tsuchiya H, Eralp L, editors. Advanced Techniques in Limb Reconstruction Surgery. Berlin: Springer Heidelberg; 2015. p. 245-99.
 |
 |
 |
 |
| Dr. Pamudji Utomo | Dr. Hendra Cahya Kumara | Dr. Anung Budi Satriadi | Dr. Dita Anggara Kusuma |
| How to Cite This Article: Utomo P, Kumara HC, Satriadi AB, Kusuma DA,. Bilateral Congenital Absence of Femur: A Rare Case Report. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 19-21. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


