
[box type=”bio”] Learning Point of the Article: [/box]
Triceps tendon is an uncommon injury that severely limits functional use of the arm, and requires a strong anatomic repair of the tendon as demonstrated in the technique presented in this report.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 35-39 | Dylan Homen, E L Domingo-Johnson, J Matthew Helm, Melinda Schalow, Mimi Zumwalt. DOI: 10.13107/jocr.2020.v10.i02.1686
Authors: Dylan Homen[1], E L Domingo-Johnson[1], J Matthew Helm[2], Melinda Schalow[3], Mimi Zumwalt[1]
[1]Department of Orthopaedic Surgery, Texas Tech University Health Sciences Center (TTUHSC), 3601 4th St. Stop 9436, Lubbock, Texas 79430-9436, United States,
[2]Department of Medicine, Texas Tech University Health Sciences Center School of Medicine, 3601 4th St. Stop 9436, Lubbock, Texas 79430-9436, United States,
[3]Department of Orthopaedic Surgery, Medical Office Bldg. 4102 24th St. Suite 407, Lubbock, Texas 79410, United States.
Address of Correspondence:
Dr. Mimi Zumwalt,
Department of Orthopaedic Surgery, LbkGenl, 3601 4th St. Stop 9436, Lubbock, Texas 79430-9436, United States.
E-mail: mimi.zumwalt@ttuhsc.edu
Abstract
Introduction: Triceps tendon rupture is a rare injury accounting for <1% of all tendon injuries with varying repair techniques described. We present this novel repair to supplement available literature and help optimize the clinical outcomes for affected patients. We report this technique because it is unique in that we augmented our surgical fixation with a subtle variation in the described technique by repairing the deep portion of the triceps tendon as a separate step, maximizing the recreation of the anatomic footprint of the triceps.
Case Report: The patient is a 70-year-old Caucasian male presenting with pain, swelling, and ecchymosis around the elbow after the episode of injury. He also complained of a painful popping sensation whenever he ranged the elbow and an inability to extend, with pain and weakness any time he attempted elbow extension. Radiographs reviewed at his initial visit revealed a small osseous fragment approximately 5 cm proximal to the olecranon tip. Subsequent MR imaging confirmed our suspicion, showing a complete tear of the triceps tendon with hematoma at its insertion site and tendon retraction approximately 3 cm proximally. With the diagnosis of triceps tendon rupture conformed, we took the patient for primary tendon repair using suture with bone bridge and suture anchor, using elements from described techniques. Our technique was unique in that we performed repair of the deep and superficial triceps attachments as separate steps, in an endeavor to improve the anatomic reconstruction of the footprint and biomechanical strength.
Conclusions: We combined findings from our review of the available literature with novel surgical techniques and suture design to maximize the patient outcome and minimize complications. The patient went on to have a very satisfactory functional recovery. We hope that this case report will complement the evidence-based care of these patients by orthopedic surgeons and lead to the best results possible.
Keywords: Triceps tendon, triceps rupture, suture repair.
Introduction
Rupture of the triceps tendon is a relatively uncommon occurrence, with much of the current literature placing its incidence at <1% of all tendon injuries [1,2,3]. When these triceps injuries are encountered, there has been a wide variety of repair methods utilized [4, 5, 6, 7, 8, 9]. Furthermore, while direct suture repair is the most widely used technique [7], multiple variations exist in suture techniques in both the way that the suture is secured to the distal tendon and manner by which the tendon is then anchored to its insertion site on the olecranon tip. Due to this large extent of variation, there is a need for more literature exploring outcomes of the more commonly adopted repair techniques to identify fixation methods that lead to the best overall functional outcome of these patients. In line with that endeavor, we present a patient with a complete triceps tendon rupture after direct trauma that was treated with a relatively novel repair technique that has shown promising results. Furthermore, we augmented our fixation with a subtle variation in the described technique by repairing/reattaching the deep portion of the triceps tendon as a separate step. It is our hope that this case report will serve to augment available literature, demonstrating/leading to optimal clinical outcomes for these patients.
Case Report
Our patient is a 70-year-old Caucasian male who presented to the Orthopedic Hand Clinic for the evaluation of his right dominant elbow. He was building a deer hunting blind when the platform fell and landed on the posterior aspect of his right arm. He noted immediate pain, swelling, and ecchymosis about the elbow at the time of the injury. He also complained of a painful popping sensation whenever he ranged the elbow and an inability to extend, with pain and weakness any time he attempted elbow extension. At the time of our first encounter with him, he was approximately 8 weeks out from the date of injury. His only significant medical history was osteoarthritis in his hands and a former smoker, quitting in 2010 after smoking for 30 years. He had no history of pain or trauma at the site before the injury and denied any history of exogenous corticosteroid use.
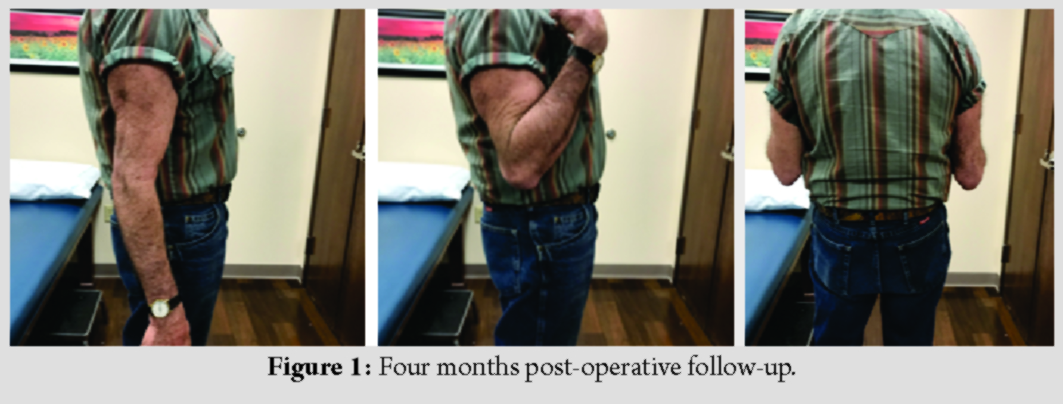
On physical examination, he was found to have tenderness to palpation just proximal to his olecranon (Fig. 1). He also had pain with range of motion of the elbow and he was unable to maintain active elbow extension against gravity or resistance. His passive range of motion was intact with no blocks to motion and functional arc of 0–140°with full pronation and supination. He was neurovascularly intact distally at the hand with no other pertinent findings on examination of the upper extremity.
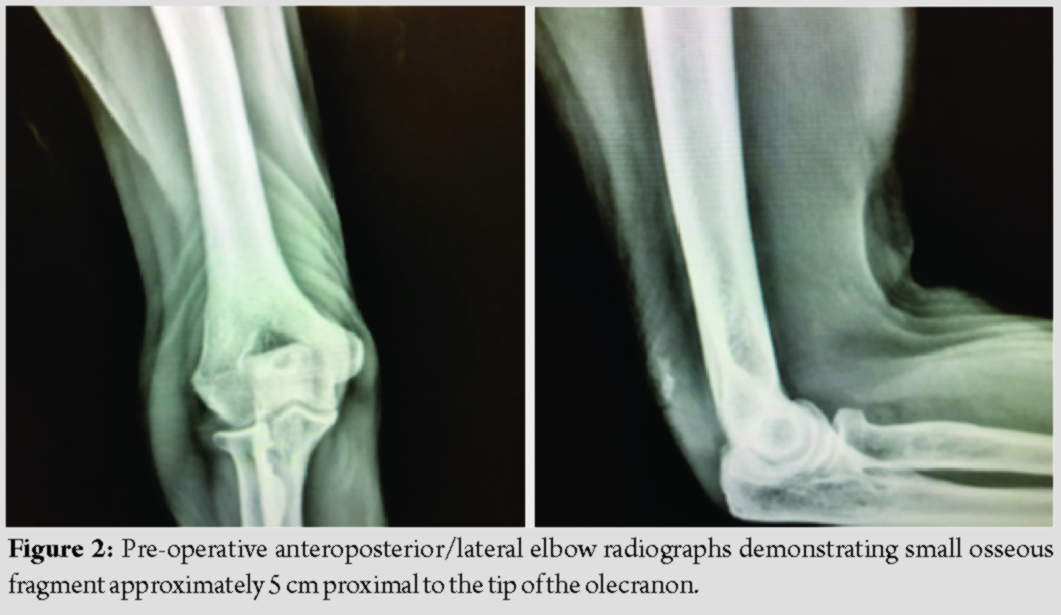
Elbow radiographs reviewed at his initial visit revealed a small osseous fragment approximately 5 cm proximal to the tip of the olecranon (Fig. 2). No other fractures, dislocations, or other bony abnormalities were appreciated. Our patient’s history, clinical examination, and radiographic findings were strongly indicative of a ruptured triceps tendon. He was to obtain advanced imaging studies and follow-up was scheduled to discuss magnetic resonance imaging (MRI) findings. The MRI confirmed our clinical suspicion by showing a complete tear of the triceps tendon with hematoma at its insertion site and retraction of the tendon approximately 3 cm proximally. Based on the degree of tear and functional impairment, it was determined that his injury would best be managed by surgical repair/reattachment of the triceps tendon to which he was amenable.

Summary of procedure
A longitudinal incision was made posteriorly just lateral to the olecranon. It was carefully taken down through subcutaneous tissues taking care to raise thick skin flaps. The ulnar nerve was identified and protected medially in the cubital tunnel. The olecranon was further dissected and as expected, the triceps was found to be completely avulsed from its footprint on the olecranon. The dissection was continued proximally to identify the retracted end of the triceps tendon. It was released and carefully advanced distally, gaining enough length so that the tendon could reach its insertion site with the elbow flexed at 90°. Thus, it was determined that the tendon could be primarily repaired without excessive tension at the attachment site. Furthermore, we planned for re-attachment of both the deep and superficial portions of the tendon using separate repair techniques in an effort to augment fixation into bone as described below.
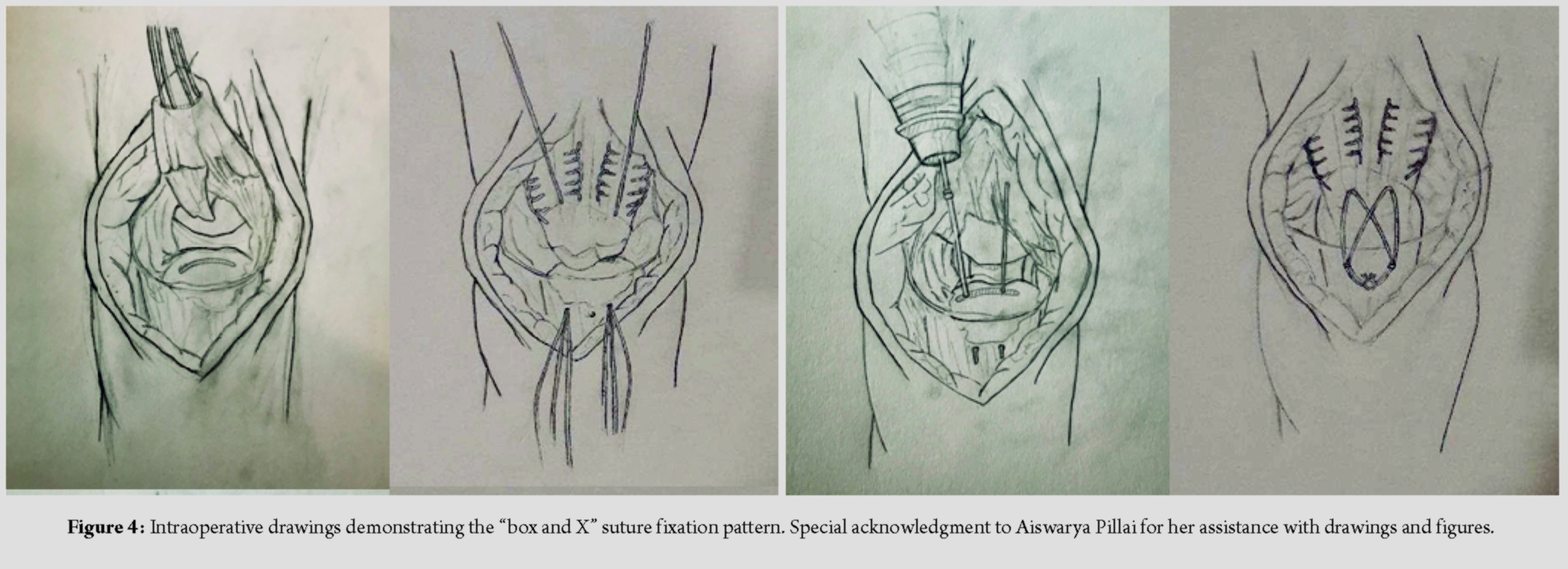
We began our repair with drilling two bone tunnels at the medial and lateral aspect of the footprint of the triceps insertion on the olecranon. We then used Fiber Wire suture to perform a standard Krackow type stitch up and down the lateral aspect of the tendon with suture strands exiting the under surface of the tendon at the level of the proximal aspect of the triceps footprint. This process was repeated for the medial aspect of the tendon using Tiger Wire suture. A Fiber Loop and Tiger Loop were inserted at the medial and lateral tendon, respectively, at the level of the existing strands of our prior suture ends. Before proceeding with final fixation, we turned our attention to repair of the deep aspect of the triceps tendon. This repair was accomplished using Arthrex 1.3 mm Suture Tape and suture anchors. The suture anchors were drilled and inserted alongside our initial bone tunnels medially and laterally. The deep tendon was then repaired using the Suture Tape with horizontal mattress sutures. We then turned our attention back to our prior sutures. We then passed and repassed the sutures through the bone tunnels in such a manner to create the classic “box and X” pattern of suture fixation across the triceps tendon insertion, adding compression of our fixation site (Fig. 3 and 4). Finally, a 4.75 mm suture anchor was drilled, tapped, and placed between our two bone tunnels distally, with all suture strands tightened and anchored appropriately. The elbow was then taken through a gentle arc of motion from 0 to 90° and the repair was found to be stable without appreciable gapping at the re-attachment site. The wound was irrigated and closed in layers, and arm placed in a posterior splint at 60–70° of elbow flexion for the protection of our repair. The patient returned for his first follow-up appointment after 12 days. He was able to range the elbow, achieving full active extension and hold it with the aid of gravity. His wound was found to be healing appropriately and his staples were removed. He was transitioned out of the splint to a hinged elbow brace, locked at 0–90°. He was then followed every 4 weeks, during which time we decreased the limitations of his elbow brace and maintained a weightlifting restriction of 5 lbs. Throughout this course, he also underwent formal physical and occupational therapy. At approximately 12 weeks out from surgery, he was found to have a well-healed surgical scar with no pain at the triceps insertion and elbow range of motion of 0–130°. At the time of writing this report, his most recent clinic visit was 4 months out from his index procedure. At that point, his weightlifting restrictions were lifted. He was discharged from physical therapy with instructions to continue a home exercise program. He was doing very well at this visit with no complications or concerns noted. He was then allowed to follow up on an as-needed basis.
Discussion
As mentioned previously, the rupture of the distal triceps tendon comprises <1% of all tendinous injuries [1, 2, 3]. Commonly occurring following a powerful eccentric contraction of the triceps musculature, these injuries are generally encountered in weight lifters and athletes [1, 10, 11, 12]. They also, as in our case, can occur following direct trauma/strike to the posterior arm [1]. These injuries are most common in patients 30–50 years of age and are more prevalent in the male population [4]. Several additional factors and medical comorbidities have been identified in the literature that have been shown to increase the rate of occurrence of triceps rupture. These include uncontrolled diabetes mellitus, chronic kidney disease, rheumatoid arthritis, and hyper parathyroidism [2, 13, 14]. As with other tendinous pathology, triceps rupture has been linked to the use of exogenous corticosteroids – both with systemic use and local steroid injections for olecranon bursitis [10, 11, 14]. Patients with triceps rupture typically present with discomfort about the distal arm and elbow, as well as decreased strength with active elbow extension. There is commonly a palpable defect at the distal triceps and a positive T. Campbell Thompson squeeze test that has been previously described [4]. The small fleck of an osseous fragment noted on lateral radiographs has been described as the Dunn-Kusnezovor “flake” sign [14], as was present in our case. If clinical examination suggests the rupture of the tendon, both MRI and ultrasound have proven to be useful adjuncts in confirming the diagnosis. Once the diagnosis of triceps rupture has been confirmed, there have been multiple treatment algorithms proposed with major determinants of treatment being length of time passed at presentation and the degree of tear. Tears are conventionally referred to as partial if <75% of the tendon is involved and if greater than referred to as complete or full-thickness tears [1]. Partial acute tears have been shown to be effectively treated with immobilization in 30° of flexion for 4–6 weeks followed by bracing with progressively increasing elbow flexion and weight-bearing/lifting allowances [4, 6, 8]. However, non-operative treatment does not take into consideration physical demands of the patient involved in sports [2]. Conversely, complete tears are typically treated with surgical repair and have good functional outcomes reported in multiple studies–Strauch [14] recommended surgical repair for ruptures involving more than 50% of the tendon. In these cases, the most widely adopted surgical method of re-attachment is direct repair with suture fixation, with some subtle to significant differences in different specific techniques. For our re-attachment, we elected to proceed with knotless repair through bone tunnels with specific attention to both the deep and superficial layers of the tendon, as well as recreating the anatomic footprint of the triceps insertion. We chose this technique for multiple reasons. First, Clark et al. [9] reported their findings that anatomic footprint repair with knotless technique had less tendon displacement on stress after re-attachment when compared to transosseous cruciate knot repair. The utilization of one suture anchor is desirable as the use of multiple suture anchors or knots increases the risk of inadvertent joint penetration as well as more bulk in the area of the olecranon, which has a notoriously tenuous soft-tissue envelope. Second, we took care to recreate the anatomic footprint of the triceps tendon. The footprint is a dome-shaped area of the olecranon that measures an average of 466 mm2, with width ranging from 1.9 to 4.2 cm based on cadaveric studies [8]. Recreating this footprint was achieved by having our sutures exit at the most proximal aspect of the insertion site and then adding compression across the footprint with the second pass of our sutures in a box and X fashion. We postulate that by doing it in this fashion helps to restore the normal anatomy and biomechanical advantage of the triceps tendon insertion, leading to improved functional outcome and more secure fixation as previously mentioned above.
Conclusion
Our case is noteworthy in that we performed repair of the deep aspect of the triceps tendon as a separate step. In a cadaveric study by Madsen et al. [15], they reported that the medial head of the triceps has a tendinous insertion that is deeper than the primary footprint. It has been proposed that failure to adequately repair this portion can lead to partial weakness in active extension, a particularly undesirable outcome in a young, active patient. Our repair was achieved with Arthrex 1.3 mm Suture Tape, a flat suture that has shown increased strength and load at failure when compared to the already robust Fiber Wire suture. Our reasoning for this technique is that it maximizes the likelihood of return to normal levels of elbow function and triceps strength. In addition, we aimed to minimize the risk of rerupture, which has an incidence that has been reported from 6to as high as 20% [5, 14].
In summary, triceps tendon ruptures are relatively uncommon injuries that may be regularly encountered in clinical orthopedic practice. When properly treated, the literature shows that these injuries can have good outcomes. We combined findings from review of the available literature with more novel surgical techniques and suture design in an effort to maximize the patient outcome and minimize complications, and our patient went on to have a very satisfactory recovery course. We hope that this case report will complement the evidence-based care of similar patients with triceps ruptures and lead to the best results possible.
Clinical Message
Triceps tendon rupture is an uncommon but debilitating injury that usually necessitates surgical repair. When surgery is indicated, anatomic reconstruction of the triceps footprint with biomechanically stable repair techniques can lead to good functional outcomes.
References
1. MarinelloPG, PeersS, SrajS, EvansPJ. A treatment algorithm for the management of distal triceps ruptures.Tech Hand Up Extrem Surg2015;19:73-80.
2. KhiamiF, TavassoliS, DeRidder Baeur L, CatonnéY, SarialiE. Distal partial ruptures of triceps brachii tendon in an athlete.OrthopTraumatol Surg Res2012;98:242-6.
3. AnzelSH, CoveyKW, WeinerAD, LipscombPR. Disruption of muscles and tendons; an analysis of 1,014 cases.Surgery1959;45:406-14.
4. YehPC, DoddsSD, SmartLR, MazzoccaAD, SethiPM. Distal triceps rupture.J Am AcadOrthop Surg2010;18:31-40.
5. vanRiet RP, MorreyBF, HoE, O’DriscollSW. Surgical treatment of distal triceps ruptures.J Bone Joint Surg Am2003;85:1961-7.
6. FarrarEL 3rd, LippertFG 3rd. Avulsion of the triceps tendon.Clin OrthopRelat Res1981;161:242-6.
7. SinghRK, PooleyJ. Complete rupture of the triceps brachii muscle.Br J Sports Med2002;36:467-9.
8. KeenerJD, SethiPM. Distal Triceps Tendon Injuries.Hand Clin2015;31:641-50.
9. ClarkJ, ObopilweE, RizziA, KomatsuDE, SinghH, MazzoccaAD, et al. Distal triceps knotless anatomic footprint repair is superior to transosseous cruciate repair: A biomechanical comparison.Arthroscopy2014;30:1254-60.
10. BachBR Jr., WarrenRF, WickiewiczTL. Triceps rupture. A case report and literature review.Am J Sports Med1987;15:285-9.
11. SollenderJL, RayanGM, BardenGA.Triceps tendon rupture in weight lifters.J Shoulder Elbow Surg1998;7:151-3.
12. WagnerJR, CooneyWP. Rupture of the triceps muscle at the musculotendinous junction: A case report.J Hand Surg Am1997;22:341-3.
13. DunnJC, KusnezovN, FaresA, RubinS, OrrJ, FriedmanD, et al. Triceps Tendon ruptures: A systematic review.Hand (N Y)2017;12:431-8.
14. StrauchRJ. Biceps and triceps injuries of the elbow.Orthop Clin North Am1999;30:95-107.
15. MadsenM, MarxRG, MillettPJ, RodeoSA, SperlingJW, WarrenRF. Surgical anatomy of the triceps brachii tendon: Anatomical study and clinical correlation.Am J Sports Med2006;34:1839-43.
 |
 |
 |
 |
 |
| Dr. Dylan Homen | Dr. E L Domingo-Johnson | Dr. J Matthew Helm | Dr. Melinda Schalow | Dr. Mimi Zumwalt |
| How to Cite This Article: Homen D, Domingo-Johnson EL, Helm JM, Schalow M, Zumwalt M. Case Report: Triceps Tendon Rupture – A Novel Repair of an Uncommon Injury. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 35-39. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


