
[box type=”bio”] Learning Point of the Article: [/box]
Understanding not only the techniques of osteosynthesis, but also the biology of bone-healing and the principles of Pauwels’s causal histogenesis is important in Orthopaedic trauma surgery.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 47-49 | Christian Konrads, Thomas Schewior. DOI: 10.13107/jocr.2020.v10.i03.1742
Authors: Christian Konrads[1],[2], Thomas Schewior[3]
[1]Department of Trauma and Reconstructive Surgery, BG Klinik, University of Tübingen, Germany,
[2]Department of Orthopaedic Surgery, University of Würzburg, Germany,
[3]Regensburg, Germany.
Address of Correspondence:
Dr. Christian Konrads,
Department of Trauma and Reconstructive Surgery, BG Klinik, University of Tübingen, Schnarrenbergstr95, 72076 Tübingen, Germany.
E-mail: christian.konrads@gmail.com
Abstract
Introduction: Although fractures of the forearm and also Galeazzi fractures are normally treated by open reduction and internal compression plate fixation, Ilizarov published good results using his ring fixator even for these injuries. Because a patient with a Galeazzi fracture denied in-hospital stay and open reduction and internal fixation of the radius shaft, he was treated by means of external fixation.
Case Report: A50-year-old patient presented 4 weeks after a Galeazzi injury without initial treatment and a shortened radius shaft associated with a dislocated distal radioulnar joint. Through a ring fixator, the fragments were distracted, reduced, and stabilized. Besides an uncomplicated pin-tract infection, the injury healed uneventfully with a very good outcome and very high patient satisfaction still 25 years after the injury.
Conclusion: By applying the principles of bone healing and osteosynthesis, even older or unconventional treatment strategies can be indicated and conducted successfully in individual patients, leading to good results and high patient satisfaction.
Keywords: Ilizarov, distraction, radius fracture, radioulnar joint, the distal radioulnar joint, bone healing.
Introduction
A Galeazzi fracture is a fracture of the radial diaphysis with ligament disruption of the distal radioulnar joint (DRUJ). The injury mechanism usually is axial loading and rotation of the forearm. If the injury is misdiagnosed and a luxation of the DRUJ is overlooked, the bad outcome must be expected with a restricted range of motion (ROM) of the forearm, chronic wrist pain, and post-traumatic arthritis [1]. In adults, Galeazzi injuries are regularly treated with open reduction of the radial shaft fracture and compression plate osteosynthesis. Then, reduction of the DRUJ is checked meticulously, and additional stabilizing procedures addressing the unstable DRUJ are performed, if needed; for example, transfixation of the DRUJ with one or two Kirschnerwires (K-wires) in the acute setting [2].
Case Report
In 1983, a 50-year-old German farmer presented with a 4-week-old Galeazzi fracture. After an injury during work, he had continued his work for a month. Then, he looked for help because the distal fragment of the radial diaphyseal fracture almost perforated the skin. As the radial fracture was dislocated ad longitudinal(shortened), the DRUJ was dislocated. The patient rejected the hospital stay. Therefore, after long discussions with the patient, ambulatory treatment was planned. Local anesthesia was injected into skin and periosteum. Under traction of the forearm with the fingers of the injured extremity being fixed above the elbow and the forearm hanging in a vertical position, the ring fixator was mounted. The radial shaft fracture still was dislocated.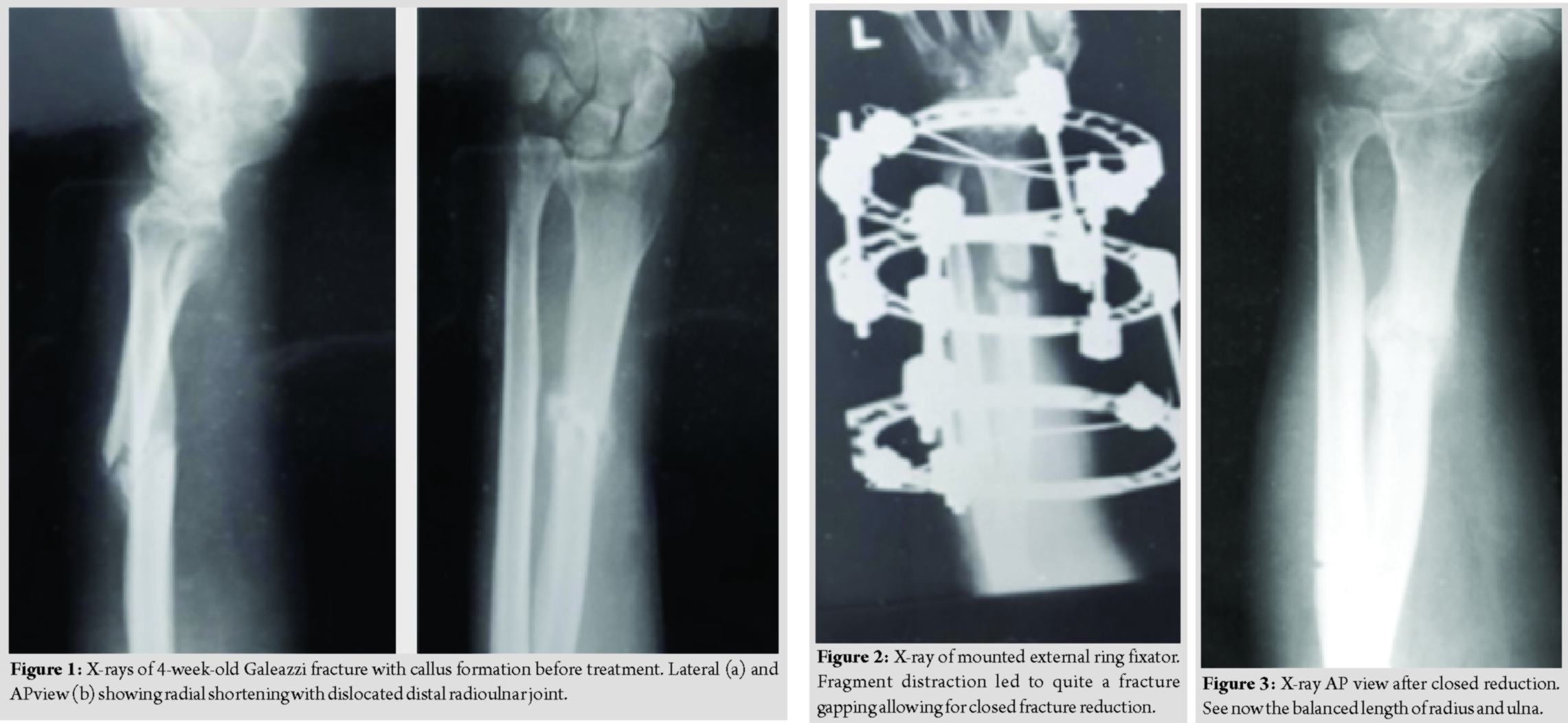
The patient was instructed to daily distract 1 mm in four small steps á 0.25 mm. After 10 days, there was a distraction of 10 mm, and the patient noticed a giving way at the fracture site of the radial diaphysis. As planned, the patient came back to the outpatient clinic, and a closed reduction of the distracted radial shaft fragments was done. The DRUJ dislocation reduced spontaneously at this moment.The farmer picked up his work again– also in the pigsty. He came back with a pin-tract infection, which could be managed with oral broad-spectrum antibiotics. The injury healed without further complications. (Fig. 1–3) depict the course of treatment. After bony consolidation and removal of the external fixator, the patient regained full ROM for a few weeks. The fracture healed, and at the last clinical follow-up, function and ROM were normal on both sides without any sign of subluxation.
Discussion
A 50-year-old patient with delayed diagnosis of a dislocated Galeazzi fracture was managed successfully using a ring fixator. Although fractures of the forearm and also Galeazzi fractures are normally treated by open reduction and internal compression plate fixation, Ilizarov published good results using his ring fixator even for these injuries [3]. Today, external fixation and especially ring fixators are used at the forearm mainly for the correction of complex deformities and bone lengthening [4, 5]. Because the patient with a Galeazzi fracture denied both, in-hospital stay and open reduction and internal fixation of the radius shaft, he should be treated by means of closed reduction and external fixation. Anatomic reconstruction of the radius shaft was needed, to have a chance for indirect anatomic reduction of the distal ulna into the sigmoid notch of the distal radius. This is known to be important for normal functioning of the wrist and forearm rotation [6, 7]. Due to the shortening of the radius shaft fracture for4 weeks, distraction was needed. This was addressed through a ring fixator. Using this device, the two bone fragments were distracted, reduced, and stabilized. First, distraction was applied: 1 mm daily in four small steps á 0.25 mm. After 10 days of distraction, there was an elongation of the radial bone of 10 mm, and the patient noticed a giving way at the fracture site of the radial diaphysis. Then, a closed reduction of the distracted radial shaft fragments could be achieved. The DRUJ dislocation reduced spontaneously at this moment. The external ring fixator construct was left in place stable until bony consolidation of the fracture without dislocation or malunion. Although the initial treatment had been delayed, under the biomechanical environment of tension-stress at the fracture site, no bone grafting was needed [8, 9]. The Ilizarov ring fixator allows for quasi-static tissue tension during distraction and significantly lower shear forces at the fracture site compared to unilateral external fixators [10]. From many studies, shear forces are well known to hinder bone healing [11, 12, 13, 14, 15].We think that using a ring fixator in the described way was helpful to optimize the biomechanical conditions for secure fracture healing. As the patient showed up 25 years after treatment being pain free with full function of the formerly injured forearm, due to ethical reasons, no X-ray could be performed at the last follow-up.
Conclusion
A 50-year-old patient, who presented 4 weeks after a Galeazzi injury without initial treatment and a shortened radius shaft associated with a dislocated DRUJ, was treated successfully through a ring fixator by fragment distraction, reduction, and stabilization showing successful clinical application of Pauwels causal histogenesis and Ilizarov’s law of tension-stress.
Clinical Message
This case shows that by applying the principles of bone healing and osteosynthesis, even older or unconventional treatment paths can be indicated and conducted successfully in individual patients, leading to good clinical long-term outcomes with high patient satisfaction.
References
1. Atesok KI, Jupiter JB, Weiss AP. Galeazzi fracture. J Am Acad Orthop Surg 2011;19:623-33.
2. Yohe NJ, De Tolla J, Kaye MB, Edelstein DM, Choueka J. Irreducible galeazzi fracture-dislocations. Hand (N Y) 2019;14:249-52.
3. Ilizarov GA. Transosseous Osteosynthesis: Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. New York: Springer; 1992.
4. Chen GX, Zhou ZA, Yang L. Ulnar lengthening using a half-ring sulcated external fixator for ulnar longitudinal deficiency: A case report. Cell Biochem Biophys 2013;67:809-12.
5. Ahmed AA. Gradual ulnar lengthening by an Ilizarov ring fixator for correction of Masada IIb forearm deformity without tumor excision in hereditary multiple exostosis: Preliminary results. J Pediatr Orthop B 2019;28:67-72.
6. Kasten P, Krefft M, Hesselbach J, Weinberg AM. How does torsional deformity of the radial shaft influence the rotation of the forearm? A biomechanical study. J Orthop Trauma 2003;17:57-60.
7. Gong HS, Roh YW, Oh JH, Lee YH, Chung MS, Baek GH. Computed tomographic assessment of reduction of the distal radioulnar joint by gradual lengthening of the radius. J Hand Surg Eur 2009;34:391-6.
8. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part I. The influence of stability of fixation and soft-tissue preservation. Clin Orthop Relat Res 1989;238:249-81.
9. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res 1989;239:263-85.
10. Ilizarov GA. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res 1990;250:8-26.
11. Carter DR, Beaupré GS, Giori NJ, Helms JA. Mechanobiology of skeletal regeneration. Clin Orthop Relat Res 1998;355:S41-55.
12. Claes L, Eckert-Hubner K, Augat P. The effect of mechanical stability on local vascularization and tissue differentiation in callus healing. J Orthop Res 2002;20:1099-105.
13. Augat P, Burger J, Schorlemmer S, Henke T, Peraus M, Claes L. Shear movement at the fracture site delays healing in a diaphyseal fracture model. J Orthop Res 2003;21:1011-7.
14. Claes L, Augat P, Schorlemmer S, Konrads C, Ignatius A, Ehrnthaller C. Temporary distraction and compression of a diaphyseal osteotomy accelerates bone healing. J Orthop Res 2008;26:772-7.
15. Claes L, Meyer N, Schülke J, Reitmaier S, Klose S, Ignatius A. The mode of interfragmentary movement affects bone formation and revascularization after callus distraction. PLoS One 2018;13:e0202702.
 |
 |
| Dr. Christian Konrads | Dr. Thomas Schewior |
| How to Cite This Article: Konrads C, Schewior T. Delayed Treatment of a Galeazzi Fracture Using an External Ring Fixator. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 47-49. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


