
[box type=”bio”] Learning Point of the Article: [/box]
Naviculocuneiform and calcaneocuboid joint dislocation can occur after low energy trauma, which should be diagnosed and treated early with open reduction and stable anatomical fixation for good functional outcome.
Case Report | Volume 10 | Issue 6 | JOCR September 2020 | Page 41-43 | Kiran P. Dhole, Ajinkya R. Bandebuche, Nandan A. Marathe, Sudeep Date, Aditya Raj| . DOI: 10.13107/jocr.2020.v10.i06.1868
Authors: Kiran P. Dhole[1], Ajinkya R. Bandebuche[2], Nandan A. Marathe[3], Sudeep Date[3], Aditya Raj[3]
[1]Department of Orthopaedics, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra, India,
[2]Department of Orthopaedics, TNMC and B.Y.L. Nair Charitable Hospital, Mumbai, Maharashtra, India,
[3]Department of Orthopaedics, Seth G.S. Medical College and K.E.M hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Ajinkya R. Bandebuche,
Department of Orthopaedics, TNMC and B.Y.L. Nair Charitable Hospital, Mumbai, Maharashtra, India.
E-mail: ajinkya49@gmail.com
Abstract
Introduction: Midfoot injuries involving naviculocuneiform and calcanealcuboid joints are very rare. These injuries result from high-energy crushing trauma and most often causes dislocation of the midfoot in plantar direction.
Case Report: A 30-year-old female sustained an injury to the left foot after a fall from a very low height. A radiograph of the left foot demonstrated naviculocuneiform joint and calcaneocuboid joint fracture–dislocation. This unusual pattern of injury required open reduction and internal fixation with K-wires after a failed attempt of closed reduction. K-wires were removed after 8 weeks. At 24 months follow-up, she achieved a complete range of movements of left foot and ankle without any complications.
Conclusion: Injuries involving naviculocuneiform and the calcaneocuboid joint can occur following low-energy impact. Such complex injuries should be diagnosed and treated as early as possible. Initial open reduction and stable anatomical fixation are the keys to achieve a good functional outcome in such kind of injuries.
Keywords: Calcaneocuboid, Naviculocuneiform, Midfoot injury, Low energy, Fracture-dislocation
Introduction
Injuries involving midfoot are rare and comprise only 5% of all foot injuries. Among these, the most common midfoot injuries are the fracture–dislocation of Chopart and Lisfranc joints [1]. Dislocations involving calcaneocuboid and talonavicular joint or isolated dislocations of calcaneocuboid, talonavicular, or naviculocuneiform joints are very rare [2]. Midfoot injuries predominantly occur in motor vehicle collisions [3]. However, dislocation of naviculocuneiform and calcaneocuboid joint following low-energy injury has been infrequently reported in the literature. This case report presents the diagnosis and management of a patient with dislocation involving naviculocuneiform and calcaneocuboid joint, which is an unusual injury.
Case Report
A 30-year-old female (weight 65 kg and height 158 cm) came to our emergency department with injury to the left foot, due to fall from the stool of height approximately 2 feet. She lost her balance while arranging things in overhead cupboards when she was standing on a stool with heels elevated and landed on the floor with plantar flexion at ankle joint and abduction at midfoot. She presented to us immediately after trauma with pain and swelling over the midfoot region without any external wounds. On clinical examination, there was severe tenderness over mid-foot, and abnormal bony prominence was present over the dorsomedial aspect of the left foot, without any distal neurovascular deficit. Midfoot joint movements were severely restricted, making the patient unable to walk. The radiographs of the left foot were done in the form of anteroposterior, lateral, and obliques views. Radiographs revealed naviculocuneiform joint dislocation and fracture of anterior process of the calcaneus with calcaneocuboid joint dislocation (Fig. 1).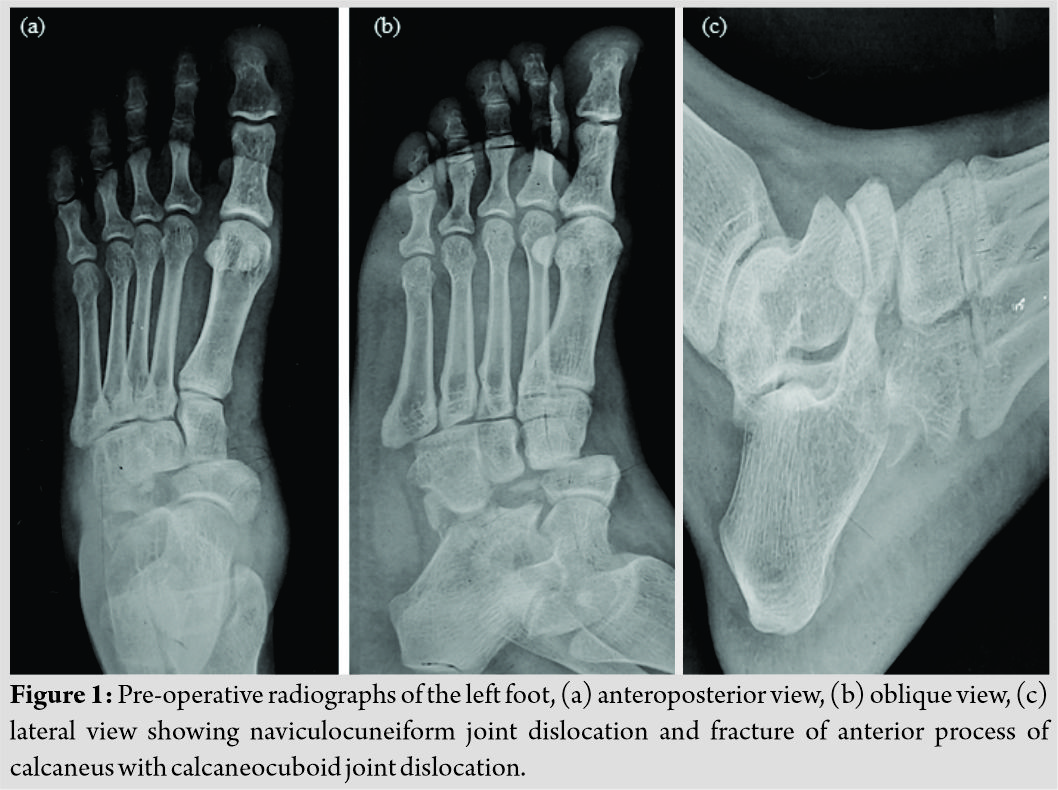
Closed reduction under anesthesia was attempted by traction and manipulation of midfoot, but it was not successful. Hence, open reduction and internal fixation with K-wire was planned. Calcaneocuboid and naviculocuneiform joints were approached with the help of two mini-open incisions 3 cm (dorsolateral) and 4 cm (dorsomedial), respectively, over midfoot. There was a disruption of interosseous ligament and medial naviculocuneiform joint capsule. The soft tissues entrapped between calcaneocuboid and naviculocuneiform joints were removed. Using axial traction in line with 1st metatarsal and adduction of midfoot, navicular was reduced. After confirming congruent reduction with the help of an image intensifier, two parallel, 2 mm K-wires were passed through medial cuneiform and navicular into the talus. A transverse K-wire was passed through medial cuneiform into middle cuneiform to give complete stability to the medial column. For the lateral column, a 2 mm K-wire was passed from cuboid to calcaneal head. Postoperatively, ankle and foot were immobilized in the below-knee slab posteriorly (Fig. 2).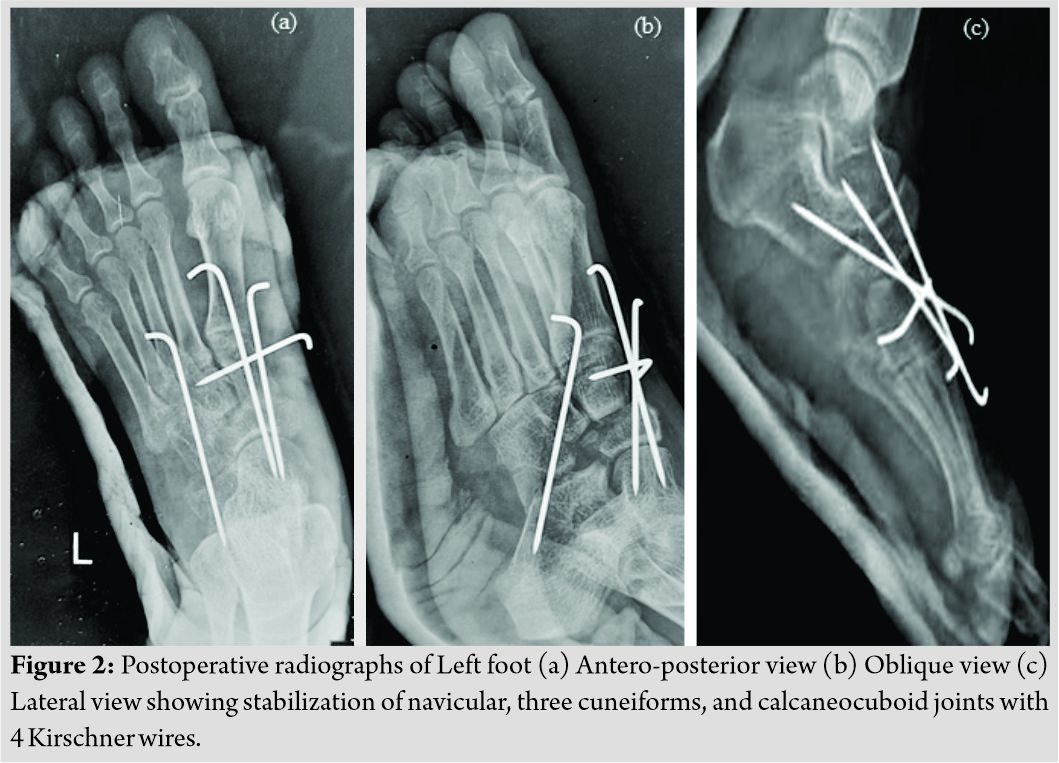
Sutures were removed after 2 weeks and below knee cast applied with strict non-weight-bearing. K-wires and below-knee cast were removed after 8 weeks and gradual weight-bearing as per tolerance started. At the end of 5 months, there was only a mild restriction of midfoot range of movements (adduction 5° and abduction 5°) with American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score of 85. At 24-month follow-up, she had a full range of midfoot movements and complained of mild pain only after fast walking and running with AOFAS midfoot score of 95 (Fig. 3).
Discussion
Dislocations involving calcaneocuboid, talonavicular, or naviculocuneiform joints are very rare [2]. The rarity of these injuries is due to the strong dorsal and volar ligamentous attachments and the rigid bony support surrounding the navicular and cuboid bones [4]. Main and Jowett reported the largest series of 71 midtarsal joint injuries. They classified these injuries according to the direction of deforming force and displacement: Medial forces, longitudinal forces, lateral forces, plantar forces, and crush injuries. Out of 71 cases, only 12 were caused by lateral displacement of the forefoot. Among these 12 cases, only four were fracture–dislocations which were managed; conservatively, the remaining injuries were undisplaced. Out of 4, two cases were operated with triple arthrodesis at a later stage. In their cases, the lateral displacement of the forefoot led to subluxation of the talonavicular joint with crushing and comminution of the lateral column of the midfoot (calcaneocuboid articulation) [5]. Our case remains unique, as the injury to the medial side of the foot consisted of a fracture–dislocation of the naviculouneiform joint, and the lateral column injury with calcaneocuboid fracture–dislocation. As per most reports, navicular dislocations are associated with extensive disruption of the midtarsal ligamentous supports, together with disruption of both medial and lateral columns of the midfoot [4, 5, 6]. Such extensive disruption suggests that the mechanism of an injury must be of high energy to produce these injury patterns. This is consistent with almost all of the published data on navicular and calcaneocuboid dislocations, the most frequently described mode of injury being road traffic accidents, a fall from a height, or significant crush injury [1, 2, 4]. This case describes a complex pattern of injury, in which plantar-abduction force at the midfoot caused the injury through naviculocuneiform joint and calcaneocuboid joints causing complete dislocation of the three cuneiforms and navicular and calcaneocuboid articulation which is very unusual considering the strong ligamentous supports around midfoot. However, unlike most other reported cases of naviculocuneiform and calcaneocuboid dislocation, this injury occurred as a result of a relatively low-energy mechanism. As per Renninger et al., a fall from a height of <4 feet is considered as a low-energy injury [7]. This case also differs due to the presence of anterior calcaneal process fracture with the intact cuboid. Main and Jowett described associated fractures to the body of the cuboid as part of their lateral dislocation groups, caused by compression between the metatarsals and calcaneum; the so-called “nutcracker fracture” [5]. Cheng et al. reported two cases of naviculocuneiform and calcaneocuboid dislocation, of which one case was associated with fracture of anterior process of calcaneum [1]. We believe that anterior calcaneal process fracture occurred due to the hyperabduction of forefoot, leading to compression of the calcaneocuboid joint at the time of injury. Anatomic reduction and stable fixation are the priority for any dislocation injury to avoid post-traumatic arthritis and to gain good functional outcome. Various treatment options for naviculocuneiform and calcaneocuboid dislocation include closed manipulation with back-slab under fluoroscopy [2], closed reduction and K-wires, open reduction, and internal fixation with K-wires or plates [1]. Richter et al. recommended long single dorsal or two dorsomedial/dorsolateral incisions in the majority of open procedures of midfoot and fixation with the help of K-wires and screws [3]. In our case, we used small incisions to approach naviculocuneiform and calcaneocuboid joint and used K-wires for fixation with good functional outcome.
Conclusion
Closed dislocation of naviculocuneiform and calcaneocuboid joints can occur following low-energy injury with plantarflexion and abduction deforming force at midfoot. Management includes early open reduction and stable anatomical fixation with gradual rehabilitation. Further reporting of such kind of midfoot injuries is required to make clear clinical guidelines for management in the future.
Clinical Message
This case report highlights the complex and very unusual variant of midfoot injury involving naviculocuneiform and calcaneocuboid joints. The mechanism of injury involves plantarflexion and abduction at midfoot which can occur by relatively low-energy impact. Priority should be given to restore the anatomy of both medial and lateral column of the foot. Initial open reduction and internal fixation yield a better functional outcome.
References
1. Cheng Y, Yang H, Sun Z, Ni L, Zhang H. A rare midfoot injury pattern: Navicular-cuneiform and calcaneal-cuboid fracture-dislocation. J Int Med Res 2012;40:824-31.
2. Choudry Q, Akhtar S, Kumar R. Calcaneocuboid and naviculocunieform dislocation: An unusual pattern of injury. Foot Ankle Surg 2007;13:48-50.
3. Richter M, Wippermann B, Krettek C, Schratt H, Hufner T, Thermann H. Fractures and fracture dislocations of the midfoot: Occurrence, causes and long-term results. Foot Ankle Int 2001;22:392-8.
4. Dhillon M, Nagi O. Total dislocations of the navicular: Are they ever isolated injuries? J Bone Joint Surg Br 1999;81:881-5.
5. Main B, Jowett R. Injuries of the midtarsal joint. J Bone Joint Surg Br 1975;57:89-97.
6. Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: Initial opens reduction provides better outcome than closed reduction. Foot Ankle Int 2004;25:340-8.
7. Renninger C, Cochran G, Tompane T, Bellamy J, Kuhn K. Injury characteristics of low-energy lisfranc injuries compared with high-energy injuries. Foot Ankle Int 2017;38:964-9.
 |
 |
 |
 |
 |
| Dr. Kiran P. Dhole | Dr. Ajinkya R. Bandebuche | Dr. Nandan A. Marathe | Dr. Sudeep Date | Dr. Aditya Raj |
| How to Cite This Article: Dhole KP, Bandebuche AR, Marathe NA, Date S, Raj A. An Unusual Midfoot Dislocation Involving Naviculocuneiform and Calcaneocuboid Joint following Low-Energy Injury: A Case Report. Journal of Orthopaedic Case Reports 2020 September;10(6): 41-43. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


