
[box type=”bio”] Learning Point of the Article: [/box]
Despite the solitary nature of schwannomas affecting the upper extremity, they can present as a group of multiple lesions engulfing the same nerve.
Case Report | Volume 10 | Issue 6 | JOCR September 2020 | Page 60-63 | Mohamed Salar, Marc B Kaye. DOI: 10.13107/jocr.2020.v10.i06.1876
Authors: Mohamed Salar[1], Marc B Kaye[1]
[1]Department of Orthopaedic Surgery and Rehabilitation, University of Florida-Jacksonville, Jacksonville, FL 32209, United States.
Address of Correspondence:
Dr. Mohamed Salar,
Department of Orthopaedic Surgery and Rehabilitation, University of Florida-Jacksonville, 655 W 8th St 2nd Floor, Ambulatory Care Center, Jacksonville, FL 32209, United States.
E-mail: mohamed.salar@jax.ufl.edu
Abstract
Introduction: Schwannomas are rare benign tumors affecting the peripheral nerves. They can grow in clusters when associated with neurofibromatosis Type II or with schwannomatosis. Typically, patients present with a palpable painless mass. However, some patients, on the other hand, present with symptomatic lesions that resemble a focal nerve compression caused by the encapsulating nature of these tumors. Surgical excision is an excellent solution for solitary symptomatic lesions. However, multiple schwannomas affecting the same nerve add another level of complexity to the surgery since these secondary masses can be too small to be detected on physical examination. A high index of suspension for schwannomatosis complemented with magnetic resonance imaging (MRI) ensures a more efficient pre-operative workup that can save the patient potentially an additional visit to the operating room.
Case Report: This is a case of a 36-year-old right-handed female presented to our clinic with a several-years history of a painful mass in her forearm. On physical examination, she had a palpable painful mass that was Tinel positive with pain and paresthesia radiating distally over the median nerve distribution. A subsequent MRI scan showed a second smaller mass distally adjacent to the main lesion along with the median nerve, both appearing to be schwannomas of the median nerve. In this case report, we discuss the patient presentation, diagnostic workup and radiographic finding, surgical technique, and pathological findings in addition to a review of the literature regarding multiple schwannomas affecting the upper extremity.
Conclusion: Schwannomas are rare benign tumors affecting the peripheral nerves. Despite their solitary nature, a handful of cases are reported in the literature that describes multiple masses encapsulating the same nerve. MRI is utilized to allow proper pre-operative planning and more accurate localization of these tumors to avoid an unplanned return to the operating room.
Keywords: Multiple schwannomas, neurilemoma, schwannomatosis.
Introduction
Schwannomas (also known as neurilemomas) are one of the most common peripheral nerve tumors [1, 2, 3]. They are typically a solitary encapsulated outgrowth originating from Schwann cells in the outer nerve sheaths [4]. They tend to localize in the head, neck, and frequently the brachial plexus. Less commonly, they tend to affect the upper and lower limbs [3, 4]. The ulnar and peroneal nerves are a frequent target and, to a lesser degree, the median nerve. The incidence of solitary lesions targeting the median nerve was reported to be around 5% [2, 5, 6, 7]. Neurilemomas are tumors of adult age with the majority of patients between the third and sixth decades. There is no gender predominance. Peripheral nerve tumors of the upper extremity pose a unique challenge when it comes to establishing a diagnosis [2, 4, 5]. They are slow-growing, and thus, symptoms develop over the years and may resemble focal peripheral nerve compressions such as carpal tunnel syndrome and cubital tunnel syndrome [5, 8]. Symptoms are reported as painless masses that form over multiple years [5, 8]. Some patients experience paresthesia and pain as the mass increases in size. Therefore, it is critical to workup the patient preoperatively in an appropriate manner to avoid unnecessary and improper surgical intervention. Magnetic resonance imaging (MRI) is frequently utilized to allow proper pre-operative planning and more accurate localization of these tumors. Despite their solitary nature, a handful of cases are reported in the literature that describes multiple masses encapsulating the same nerve. The incidence of multiple schwannomas has been reported to be approximately 1% [8, 9]. Multiple schwannomas of the ulnar and median nerves are typically more common than the radial nerve [8].
Case Report
A 36-year-old right-handed female presented to our clinic with a history of a painful mass in her right forearm for over 7 years. She reported that she was advised by her primary care provider to get an MRI to workup this lesion. However, she was lost to follow-up until her most recent presentation to our institution. She described her symptoms as an intermittent pain that is associated with touch and direct palpation over the volar aspect of her forearm. On examination, there was a palpable mass about 4.0 cm distal to the elbow on the volar aspect of the forearm, measured 3.5 cm×2.0 cm. The mass was tender to palpation and was Tinel positive with pain and paresthesia radiating distally over the median nerve distribution. There was no objective sensory or a motor deficit. The patient reported no history of trauma. The patient denied any personal or family history of neurofibromatosis (NF) or schwannomatosis. MRI was ordered to better characterize this tumor and to rule out multiple masses affecting the same nerve. Multiplanar multisequence MR images were obtained with and without contrast. The mass appeared to have a large fusiform shape. It was found to be deep to the pronator teres muscle and immediately medial to the brachial artery and vein, and it measured 3.5 cm×2.0 cm. In addition, within the volar forearm, there was a second lesion, adjacent, and concurrent. This mass was relatively smaller and appeared to be distal to the main lesion and was located posterior to the brachial artery and vein. It measured approximately 1.5 cm×1.0 cm. Both were, enhancing, well-rounded lesions associated with the median nerve. The patient was offered different treatment options and ultimately elected to proceed with surgery. A microsurgical technique was used to explore the median nerve. A curvilinear incision from the medial elbow to mid-lateral forearm, sharply through the skin, blunt dissection down onto the forearm fascia and lacertus fibrosis, and divided and then careful dissection onto the brachial artery and median nerve. The median nerve tumor at the elbow was identified and isolated. Continued dissection distally, with the release of the pronator and the forearm median nerve mass, was identified. The proximal mass was then dissected from the median nerve, with careful peeling of the fascicles that were splayed over the mass capsule. The mass was then excised. The distal mass was then similarly dissected from the median nerve, as was described earlier. The histology of the tumor showed a classic picture of a benign nerve sheath tumor. The first area appeared to be hypercellular with palisading nuclei bundles described in the literature as Antoni A tissue. There was also a second area with a loose stroma, myxoid changes, and fewer cells resembling an Antoni B tissue. The histology analysis showed an S-100 protein-positive which was consistent with schwannoma. Postoperatively, the patient reported minor dysesthesia that was resolved by the time she presented to her 2-week post-operative clinic visit. The patient was lost to follow-up 9 months postoperatively.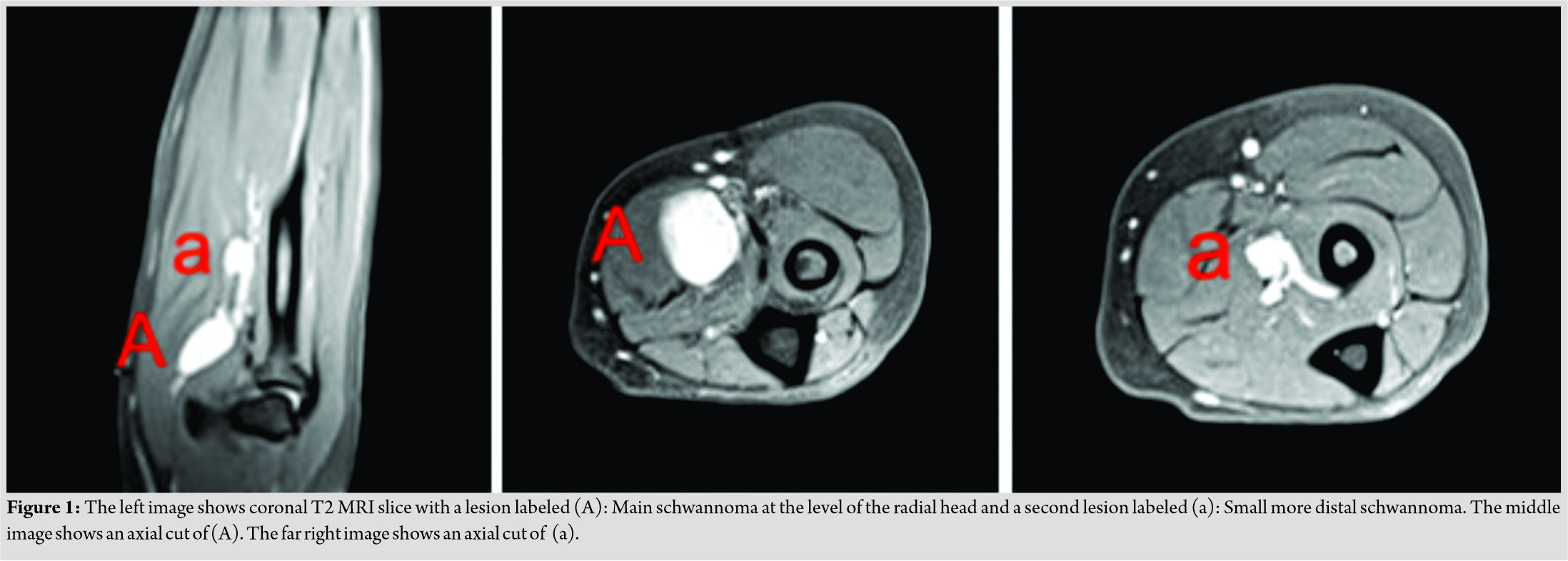
Discussion
Schwannomas are solitary peripheral nerve tumors. They can also form a group of contiguous lesions when part of a systemic pathology such as NF 2 and/or schwannomatosis [3, 4]. Nonetheless, a handful of cases reported previously in the literature which depicted multiple schwannomas encapsulating a single peripheral nerve with no associated systemic pathology [8]. Aslam et al. reviewed the literature from 1970 to 2000 and found only 14 reports similar cases depicting the rarity of this presentation. Therefore, they must be considered on the differential diagnosis during the pre-operative evaluation. Our case highlights the importance of the physical examination combined with the utility of advanced imaging. These lesions, though affecting the same nerve, typically are not the same size. Therefore, smaller lesions can be missed on physical examination as they tend to be difficult to palpate relative to their size. MRI is an important diagnostic tool and frequently employed to localize these masses. MRI can be used to better characterize the main lesion but can also be employed to investigate additional lesions adjacent or involving the same compartment, as was reported in the literature [4]. This will increase the likelihood of identifying multiple schwannomas in the upper extremity. The radiographic features of our case were similar to what previously reported regarding multiple schwannomas [10, 11]. The MRI study showed an eccentric mass with an enhanced signal on T2-weighted images and reduced signal on T1-weighted images (Fig. 1). The histology of these tumors tends to show a positive S-100 protein marker that is commonly associated with schwannoma and typically organized in two clusters, Antoni A and Antoni B. These clusters help distinguish schwannoma from neurofibroma which tends to be less organized. These tumors usually are surgically excised. The use of a tourniquet is typically employed to prevent surgical field distortion by bleeding. With a microsurgical method, a meticulous dissection of the soft tissue and nerve is carried proximal to distal from the lesions. The goal is to establish a window into the epineurium in an area void of splayed fascicles. This is followed by a circumferential dissection to separate the tumor from the healthy nerve tissue. Once the mass is excised completely, the wound is copiously irrigated, the tourniquet is released, and hemostasis is established. The patient can start range of motion as tolerated immediately postoperatively.
Conclusion
Despite the solitary nature of these nerve tumors, in rare instances, schwannomas can occur in a group. More than one lesion can affect the same peripheral nerve in a juxtaposition. Therefore, identifying all nerve-offending masses before surgery minimizes the soft-tissue insult during surgery and ensures a faster recovery. In addition, MRIs can possibly save patients an additional surgery if symptoms fail to improve secondary to undetected mass.
Clinical Message
Our case also highlights the importance of the physical examination combined with the utility of advanced imaging. It adds to few published reports of multiple schwannomas in the upper extremity. This report also underlines the clinical presentation of these patients, pre-operative workup, and proposed surgical intervention.
References
1. Barre PS, Shaffer JW, Carter JR, Lacey SH. Multiplicity of neurilemomas in the upper extremity. J Hand Surg Am 1987;12:307-11.
2. Phalen GS. Neurilemmomas of the forearm and hand. Clin Orthop Relat Res 1976;114:219-22.
3. Shin KH, Moon SH, Suh JS, Jahng JS. Multiple neurilemomas. A case report. Clin Orthop Relat Res 1998;357:171-5.
4. Aslam N, Kerr G. Multiple schwannomas of the median nerve: A case report and literature review. Hand Surg 2003;8:249-52.
5. Holdsworth BJ. Nerve tumours in the upper limb. A clinical review. J Hand Surg Br 1985;10:236-8.
6. Strickland JW, Steichen JB. Nerve tumors of the hand and forearm. J Hand Surg Am 1977;2:285-91.
7. Whitaker WG, Droulias C. Benign encapsulated neurilemoma: A report of 76 cases. Am Surg 1976;42:675-8.
8. Ozdemir O, Ozsoy MH, Kurt C, Coskunol E, Calli I. Schwannomas of the hand and wrist: Long-term results and review of the literature. J Orthop Surg (Hong Kong) 2005;13:267-72.
9. Hecht OA, Hass A. Regional multiplicity of a neurilemmoma. Hand 1982;14:97-9.
10. Spillane RM, Whitman GJ, Chew FS. Peroneal nerve ganglion cyst. AJR Am J Roentgenol 1996;166:682.
11. Lacour-Petit MC, Lozeron P, Ducreux D. MRI of peripheral nerve lesions of the lower limbs. Neuroradiology 2003;45:166-70.
 |
 |
| Dr. Mohamed Salar | Dr. Marc B Kaye |
| How to Cite This Article: Salar M, Kaye MB. Multiple Schwannomas of the Median Nerve: A Case Report and Review of the Literature. Journal of Orthopaedic Case Reports 2020 September;10(6): 60-63. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


