
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Idiopathic proximal Radioulnar synostosis is a rare condition, should be suspected in cases of restricted rotatory movements of the forearm without any history of trauma or surgery.
Case Report | Volume 10 | Issue 7 | JOCR October 2020 | Page 49-52 | Neetin P Mahajan, Prasanna Kumar. G S, Amit Kumar Yadav, Akash V Mane, Akhil Gop. DOI: 10.13107/jocr.2020.v10.i07.1914
Authors: Neetin P Mahajan[1], Prasanna Kumar. G S[1], Amit Kumar Yadav[1], Akash V Mane[1], Akhil Gop[1]
[1]Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Prasanna Kumar . G S,
Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India.
E-mail: prasannakumargs5@gmail.com
Abstract
Introduction: Radioulnar synostosis is a bony connection between the radius and ulna, which causes restriction of the active and passive rotational movements of the forearm such as supination and pronation, which can lead to significant functional disability in the patients.
Case Report: A 35-year-old male carpenter presented with the complaint of right forearm supination and pronation restriction for the past 8 months with minimal pain at the elbow region with no previous history of trauma or surgery. On examination, forearm supination and pronation movements were completely restricted with normal elbow flexion and extension and with no neurovascular deficit. X-ray of the right radius ulna with elbow revealed synostosis between proximal radius and ulna at the level of the radial tuberosity. Synostosis was removed using both anterior and posterior approaches. Postoperatively patient is having good supination and pronation movements, no pain, and difficulty in his occupation.
Conclusion: Idiopathic proximal radioulnar synostosis should be suspected in patients having restricted rotatory movements of forearm with no previous history of trauma or surgery and this is the first reported case of idiopathic proximal radioulnar synostosis. Complete resection of the synostosis with early initiation of aggressive physiotherapy helps in getting good functional outcomes.
Keywords: Idiopathic, Proximal radius ulna, Synostosis.
Introduction
Radioulnar synostosis is a bony connection between the radius and ulna, which causes restriction of the active and passive forearm supination and pronation movements, which can lead to significant functional disability in the patients. Radioulnar synostosis can be either congenital or post-traumatic type. Synostosis presents since birth called congenital variety and presents after trauma or surgery called post-traumatic variety [1]. The congenital variety seen only in the proximal forearm and the post-traumatic type may present anywhere along the radius and ulna depending on the site of trauma and soft tissue injury. Distal radioulnar synostosis may develop due to trauma, osteochondroma [2], or may be idiopathic [3]. Post-traumatic or post-surgical synostosis is the most common cause for proximal radioulnar synostosis followed by congenital variety. The management options include osteotomy and excision of the synostosis part, derotation osteotomy in low demand patients, and placement of fat, fascia, bone wax, silicone, polyethylene [4, 5] after resection to prevent the recurrence and early initiation of forearm rotation exercises.
Case Report
A 35-year-old male Carpenter presented with right forearm supination and pronation restriction for the past 8 months and also had difficulty in tightening and loosening of screws with minimal pain at the elbow region. There was no history of previous trauma, no history of any elbow or forearm surgeries. The patient was apparently normal 8 months back without any restriction of movements and pain. On examination, supination and pronation of the right forearm were completely restricted (Fig. 1) and had normal elbow flexion and extension with no distal neurovascular deficit.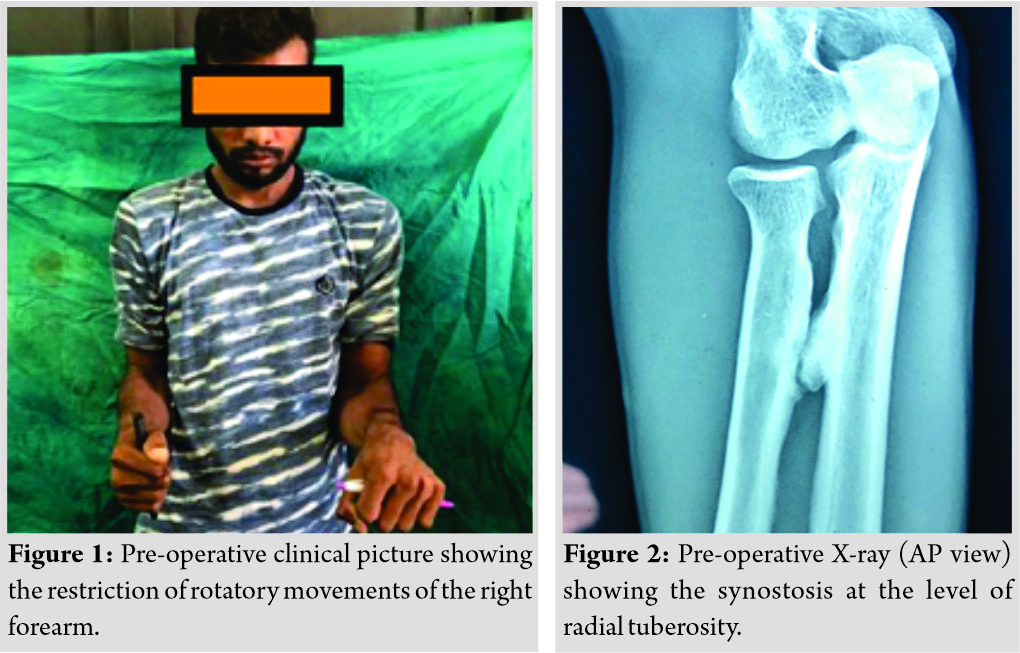
X-ray of the right radius ulna with elbow and wrist was taken, and it revealed a bony bridge (synostosis) between proximal radius and ulna at the level of radial tuberosity (Fig. 2, 3), Type 3b according to Jupiter and Ring classification [5]. CT scan of proximal radius ulna with elbow was done for better delineation of synostosis anatomy, location, and for pre-operative planning. It showed the bony connection between proximal radius and ulna (Fig. 4).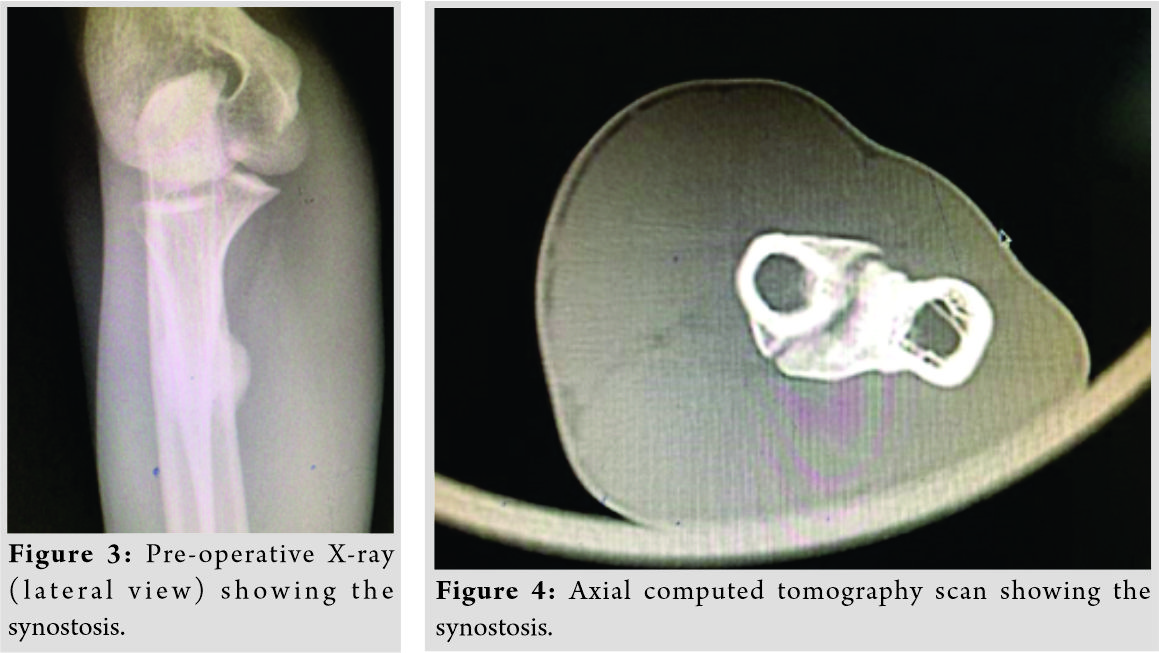
As the patient was having functional limitations in his occupation and daily routine activities due to restriction of forearm rotatory movements, and also patient demanded for surgery, we planned for surgical excision of synostosis after explaining the risks involved in surgery such as neurovascular injury, fracture, incomplete restoration of the forearm rotatory movements, and recurrence of synostosis.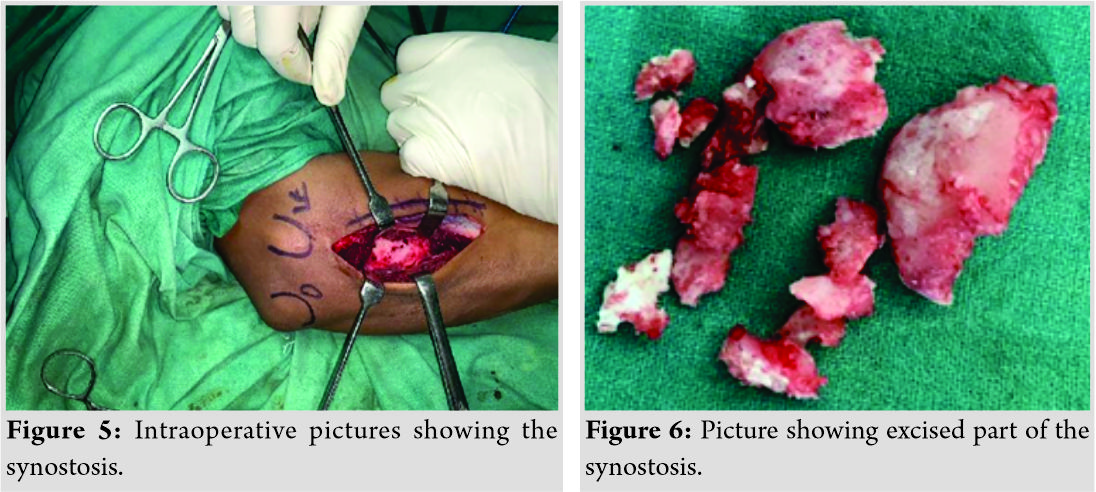
The patient was operated in a supine position using tourniquet by posterior approach initially. After identification of the posterior interosseous nerve, it was separated and protected and the synostosis site was reached (Fig. 5). Using 1.5 mm K wires, multiple holes were made at the margin of the synostosis. Then using osteotome, posterior part of the synostosis was separated and removed. Anterior part of the synostosis could not be removed completely from the posterior approach. Hence, it was removed using anterior approach to the proximal radius without sacrificing the biceps insertion. After the completion of excision, bone wax and forearm fascia were used as interposition materials to prevent recurrence and the wound was closed in layers. The excised synostosis part (Fig. 6) was sent for histopathological examination.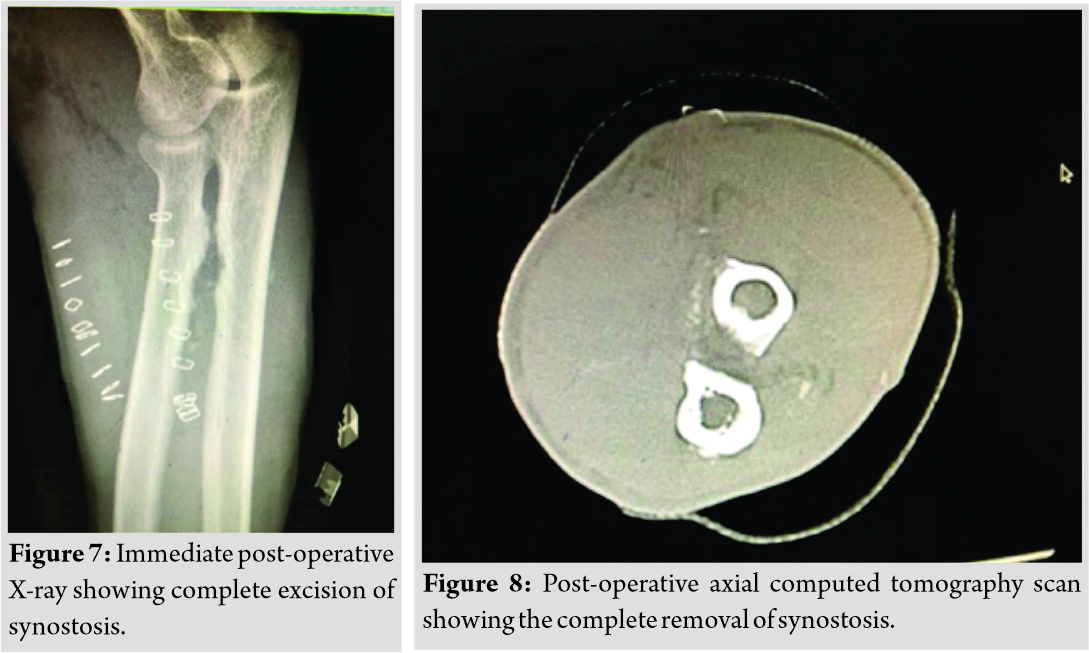
Post-operative physiotherapy was started on the 2nd post-operative day, including both active and passive supination, pronation of forearm and flexion, extension of the elbow, aggressive physio-therapy was continued up to 3 months post-surgery. The patient was able to perform good forearm rotatory movements after the surgery. Histopathology examination was suggestive of sclerotic bone fragments with no any other specific pathology. Post-operative X-ray and CT scan showed complete excision of the synostosis (Fig. 7, 8).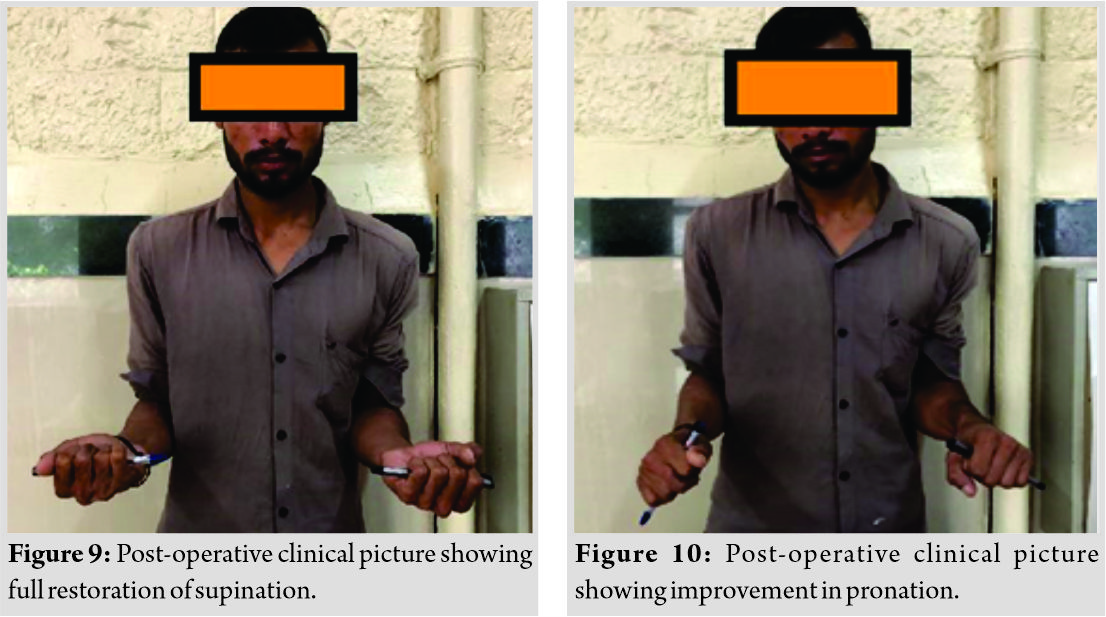
At present 2 years follow-up, the patient is having good forearm rotatory movements with complete restoration of supination and pronation restoration of about 40 degrees (Fig. 9, 10) with no pain and difficulty in his occupation and also there is no radiological evidence of recurrence. We are still following up the patient regularly to check for recurrence.
Discussion
The patient had a bony connection between the proximal radius and the ulna, this clinical entity is known as proximal radioulnar synostosis. The only reported causes of proximal radioulnar synostosis are post-traumatic and the congenital variety [1]. The congenital radioulnar synostosis caused by the failure of separation of fused cartilaginous precursors of radius ulna during the 7th week of gestation and 60% are bilateral. The congenital variety may be associated with other musculoskeletal disorders such as clubfoot, congenital dislocation of hip, polydactyly, or syndactyly [6, 7]. If the dis-ability is less, it can be compensated with adjacent joint movements. Physiotherapy, occupational therapy, and activity modifications help to avoid excessive strain over the adjacent joints and the surgery to regain rotatory movements rarely succeed [8]. Post-traumatic radioulnar synostosis is a rare complication after the elbow or forearm fracture. Synostosis can occur anywhere in the radius ulna, causing restriction of rotatory movements and functional impairment [9]. Surgical management is the optimal management for these cases if patients are functionally affected. The best timing for surgery is still debatable, resection between 6 and 12 months helps in reducing the recurrence if done in patients with radiographic bony maturation, according to Pfanner et al. [10], a similar thing was done in our case. Early and intensive rehabilitation therapy helps in good outcome; the recurrence risk after primary resection is about 6–35% with a higher incidence in significant soft tissue injury and associated head injury [9]. Heterotrophic ossification (HO) can also cause proximal radioulnar synostosis in extreme forms, which is commonly associated with trauma. We ruled out HO as the patient had no trauma, radiological and histopathological examination was not suggestive of HO. The patient did not have any history of trauma or previous surgical interventions. There was no radiological evidence of previous trauma or surgery. The other known etiology for proximal radioulnar synostosis is congenital, which seems unlikely in this case as the patient was apparently normal and had normal forearm movements till the age of 35 years. We did not find any causes for the development of proximal radioulnar synostosis in this case after thorough clinical and radiological examination. The patient did not give a history of trauma or previous surgery and the patient was apparently normal since childhood without any restriction in forearm rotatory movements. Hence, we are considering this case as an idiopathic variety of proximal radioulnar synostosis. According to the author’s best knowledge and review of literature, there were no reported cases of idiopathic proximal radioulnar synostosis and this is the first reported case of idiopathic proximal radioulnar synostosis.
Conclusion
Idiopathic proximal radioulnar synostosis should be suspected in patients having restricted rotatory movements of the forearm with no previous history of trauma or surgery. Complete resection of the synostosis with early initiation of aggressive physiotherapy helps in getting good functional outcomes.
Clinical Message
Idiopathic proximal radioulnar synostosis is a rare condition but should be kept in mind while examining the patients with restricted forearm rotatory movements which helps in clinical diagnosis. Complete excision or removal of the synostosis is essential to prevent recurrence and to get a better functional outcome. Early initiation and continuation of aggressive physiotherapy are very important to get final good functional outcome, which improves the functional disability of the patients.
References
1. Sachar K, Akelman E, Ehrlich MG. Radioulnar synostosis. Hand Clin 1994;10:399-404.
2. Radhakrishna R, Babu BR, Prashanth V. A case of osteochondroma of distal radius mimick-ing distal radio: Ulnar synostosis: Rare presentation-with review of literature. J Evol Med Dent Sci 2015;4:11918-21.
3. Shoham Y, Gurfinkel R, Sagi A. Idiopathic distal radioulnar synostosis. J Plast Surg Hand Surg 2014;48:89-90.
4. Failla JM, Amadio PC, Morrey BF. Post-traumatic proximal radio-ulnar synostosis. Results of surgical treatment. J Bone Joint Surg Am 1989;71:1208-13.
5. Jupiter JB, Ring D. Operative treatment of post-traumatic proximal radioulnar synostosis. J Bone Joint Surg Am 1998;80:248-57.
6. Wurapa R. Radioulnar Synostosis; 2009. Available from: http://www.emedicine.medscape.com/article/1240467-overview-a6. [Last accessed on 2016 Aug 02].
7. Guma M, Teitel AD. Adolescent presentation of congenital radioulnar synostosis. Clin Pe-diatr (Phila) 1996;35:215-7.
8. Tsai J. Congenital radioulnar synostosis. Radiol Case Rep 2017;12:552-4.
9. Osterman AL, Arief MS. Optimal management of post-traumatic radioulnar synostosis. Or-thop Res Rev 2017;9:101.
10. Pfanner S, Bigazzi P, Casini C, De Angelis C, Ceruso M. Surgical treatment of posttraumat-ic radioulnar synostosis. Case Rep Orthop 2016;2016:5956304.
 |
 |
 |
 |
 |
| Dr. Neetin P Mahajan | Dr. Prasanna Kumar. G S | Dr. Amit Kumar Yadav | Dr. Akash V Mane | Dr. Akhil Gop |
| How to Cite This Article: Mahajan NP, Kumar GSP, Yadav AK, Mane AV, Gop A. Idiopathic Proximal Radioulnar Synostosis – A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2020 October;10(7): 49-52. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


