
Whenever doctors are confronted with chordoma they should be aware that distant metastasis could happen.
Dr. Amal AF Halim,
Department of Clinical Oncology and Nuclear Medicine, Faculty of Medicine, Mansoura Univ., Egypt.
E-mail: halim43210@mans .edu.eg
Introduction: Chordoma is a malignant neoplasm that arises from notochord remnants. Its incidence is highest above the age of 50 and behaves as a locally aggressive tumor with a slow growth rate. In most cases, complete surgical resection followed by radiotherapy offers the best chance of control. Developing metachronous tumors or distant metastasis is uncommon.
Case Report: A 56-year-old male patient of sacral chordoma was treated by surgery and radiotherapy. He developed later bilateral inguinal lymph node metastasis and metachronous clivus chordoma.
Conclusion: Chordomas are rare. Multiplicity of primary disease and distant metastasis could happen, so regular follow-up is warranted and more effective therapeutic modalities are needed.
Keywords: Chordoma, sacrococcygeal tumors, notochord tumors, lymph node metastasis, clivus tumors.
Chordomas arise from embryonic remnants of the notochord and show both epithelial and mesenchymal differentiation. Microscopic foci remain in the vertebral bodies at the cranial and caudal ends of the embryo skeleton [1]. Chordomas arise from the sacrum in approximately half of the cases and from the skull base region in approximately one-third of them [2]. Our sacral chordoma case showed a unique clinical scenario of developing bilateral inguinal lymph node metastasis followed by the development of a metachronous clivus chordoma.
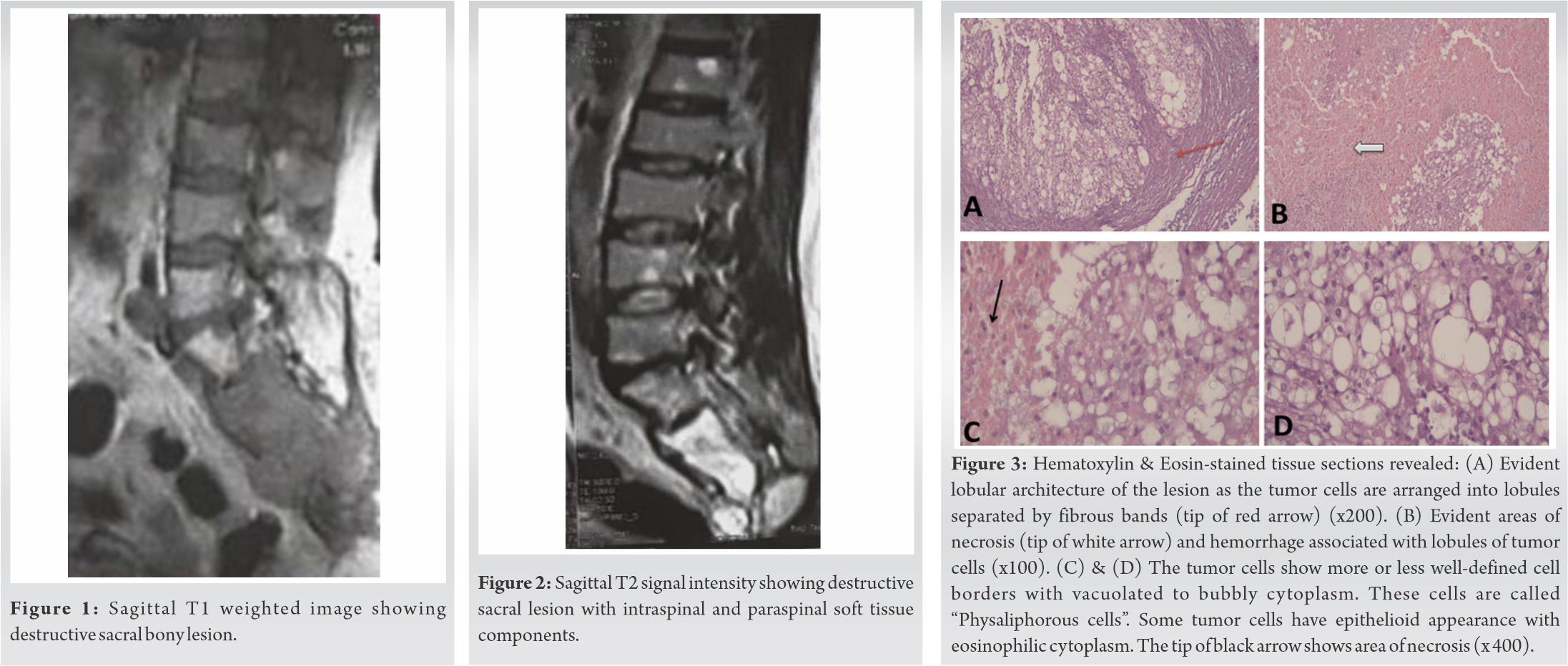
A 56-year-old male patient presented by a gradually progressive course of lower back pain, burning sensation of both lower limbs followed by urinary incontinence. The past history was irrelevant. X-ray of lumbosacral region revealed sacral osteolytic lesion with an associated soft-tissue mass. Non-contrast computed tomography of lumbosacral spine revealed a large 11 cm × 8 cm × 12 cm lobulated mass of the sacrum filling the sacral canal and having pre- and retro-sacral extension. The patient underwent maximal possible excision of sacral mass in December 2018 and the post-operative pathology revealed chordoma. Post-operative magnetic resonance imaging (MRI) showed a well-defined heterogeneously enhanced residual destructive bony lesion 8.5 cm × 6.5 cm × 7.5 cm affecting the sacrum (Fig. 1, 2). The panel decided post-operative conventional radiotherapy dose of 60 Gy in 30 sessions. The follow-up MRI revealed about 30% response. There was clinical improvement following the surgery and radiotherapy.
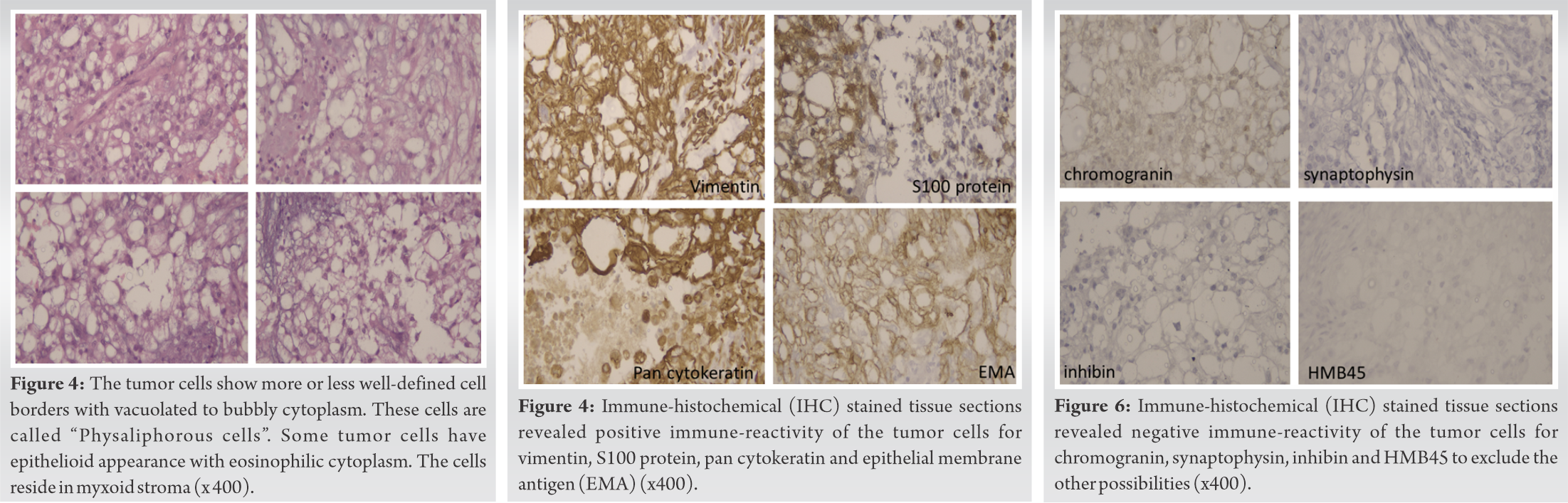
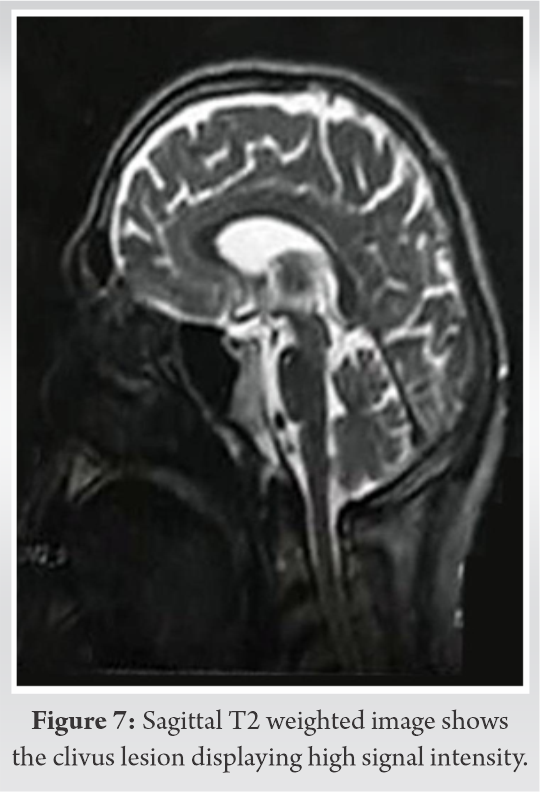
In February 2020, the patient developed left inguinal swelling. Pelvic sonar showed enlarged left inguinal lymph node 3.5 cm × 2 cm × 3 cm with distorted hilum. Excisional biopsy was done and revealed metastatic chordoma (Fig. 3-6). Metastatic work-up was free. The patient started Gleevec 400 mg daily. In June 2020, the patient developed an enlarged right inguinal lymph node 4 cm × 3.5 cm × 3 cm and the excision biopsy revealed metastatic chordoma as well. Metastatic work-up was free. Gleevec was stopped. A second-line target therapy was recommended but was not received by the patient. In September 2020, the patient developed headache, dysarthria, numbness at cheek, and lips. MRI brain revealed a well-defined abnormal signal intensity at the left side of clivus 3 cm × 4.5 cm × 4.8 cm suggesting chordoma (Fig. 7). Transnasal biopsy revealed chordoma.
In October 2020 , the panel decided conventional radiotherapy of 60 Gy in 30 sittings. The follow-up MRI revealed regression of the clivus lesion and the patient improved clinically. At present, the patient is clinically stable while on follow-up.
Metastatic chordomas in lymph nodes are rare. Sopta et al. [3] reported a case of a 38-year-old male patient with solitary inguinal lymph node metastasis without local recurrence of a previously surgically treated primary sacrococcygeal chordoma and Jain et al. [4] reported a skull base chordoma presented in association with a nasopharyngeal chordoma and cervical lymph node metastasis. Our case is a unique case of bilateral inguinal lymph node metastasis from sacral chordoma. Other metastatic sites were rarely reported in literature as heart, mandible, skin, lung, and the cerebrospinal fluid [5, 6, 7, 8, 9].Moreover, our case developed also a metachronous chordoma in the clivus. Synchronous and metachronous development of chordomas along the neural axis has been rarely reported [10, 11, 12, 13, 14].
Chordomas are rare. Multiplicity of primary disease and distant metastasis could happen.
Regular chordoma follow-up is warranted and more effective therapeutic modalities are needed.
References
- 1.Dahlin DC, McCarty CS. Chordoma. A study of 59 cases. Cancer 1952;5:1170-8. [Google Scholar]
- 2.Mirra JM, Nelson SD, Rocca CD, Mertens F. Chordoma. In: Fletcher CD, Unni KK, Mertens F, editors. World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of Soft Tissue and Bone. Lyon, France: IARC Press; 2002. p. 316-7. [Google Scholar]
- 3.Sopta J, Tulic G, Mijucic V, Mamontov P, Mandic N. Solitary lymph node metastasis without local recurrence of primary chordoma. Eur Spine J 2009;18 Suppl 2:191-5. [Google Scholar]
- 4.Jain BB, Datta S, Roy SG, Banerjee U. Skull base chordoma presenting as nasopharyngeal mass with lymph node metastasis. J Cytol 2013;30:145-7. [Google Scholar]
- 5.Stefàno PL, Barletta G, Andrei V, Cerillo AG, Nesi G, Pilato G, et al. Cardiac metastasis from sacral chordoma. Ann Thorac Surg 2020;2020:31750-1. [Google Scholar]
- 6.Krishnamurthy A. Mandibular metastasis as a presenting feature of a clival chordoma. J Cancer Res Ther 2020;16:668-71. [Google Scholar]
- 7.7-Berlucchi S, Nasi D, Zunarelli E, Valluzzi A, Ciufelli MA, Presutti L, et al. Cutaneous metastasis from cervical spinal chordoma: Case report and literature review. World Neurosurg 2020;137:296-303. [Google Scholar]
- 8.Agunbiade S, Nada A, Bhimaniya S, Whitehead MT, Mahdi ES. Chordoma with lung metastases at initial presentation of a pediatric patient. Radiol Case Rep 2020;15:382-6. [Google Scholar]
- 9.Nor FE, Desai V, Chew LL. Clival chordoma with drop metastases. J Radiol Case Rep 2018;12:1-9. [Google Scholar]
- 10.Lim JJ, Kim SH, Cho KH, Yoon DH, Kim SH. Chordomas involving multiple neuraxial bones J Korean Neurosurg Soc 2009;45:35-8. [Google Scholar]
- 11.Chou D, Acosta F Jr., Cloyd JM, Ames CP. Parasagittal osteotomy for en bloc resection of multilevel cervical chordomas. J Neurosurg Spine 2009;10:397-403. [Google Scholar]
- 12.Grossbach A, Baimeedi P, McDonald W, Bergman T. Multicentric chordoma: A case report and review of the literature. Neurosurgery 2011;69:E1327-32. [Google Scholar]
- 13.Anagiotos A, Preuss SF, Drebber U, Jumah MD. Multiple craniocervical chordomas presenting as a parapharyngeal mass. Head Neck 2013;35:E325-7. [Google Scholar]
- 14.Aydin AL, Sasani M, Oktenoglu T, Solaroglu I, Ozer AF. A case of chordoma invading multiple neuroaxial bones: Report of ten years follow up. Turk Neurosurg 2013;23:551-6. [Google Scholar]







