
Traumatic hip dislocation with ipsilateral femoral neck and acetabulum fractures is complex injuries and surgeon managing these rare injuries should be well versed with both primary osteosynthesis and arthroplasty.
Dr. Atul Rai Sharma,
Department of Orthopaedics, Government Medical College Hospital, Chandigarh, India.
E-Mail: atortho00001@gmail.com
Introduction: Traumatic dislocation of hip associated with ipsilateral femur neck and acetabulum fracture is a rare and devastating injury as a result of high-energy trauma, with potential complications of femur head aseptic necrosis and hip joint degenerative arthritis. Patients, postoperatively, may encounter decreased functional outcomes and serious challenge, during activities of daily living. Management guidelines lack clarity, with possible options including fracture fragments fixation or hip joint replacement.
Case Report: A 45-year-old patient was diagnosed with posterior dislocation of hip with ipsilateral femur neck and acetabulum fracture. Plan for emergent hip reduction and primary surgical fixation of fracture fragments was made. Intraoperatively, posterior wall acetabulum fracture was found to be excessively comminuted and non-amenable for fixation and femoral head was found to be avascularized. Subsequently, plan was changed to total hip replacement with acetabular defect reconstruction. At 1-year follow-up, no aseptic loosening was observed on radiographic views of pelvis, with total Harris Hip Score of 91.
Conclusion: Early operative management for such complex injuries is a necessity. Definitive management in the form of primary fracture fixation/arthroplasty should be decided intraoperatively.
Keywords: Femur neck, hip dislocation, acetabulum fracture, ipsilateral, case report.
Ipsilateral dislocation of hip with associated femur neck and acetabulum fracture is a rare entity [1]. These types of injuries are mainly the result of very high-energy trauma [2]. Associated injuries of thorax, abdomen, and brain which may endanger the prognosis of the patient may be present [3]. Despite prompt and effective strategized treatment, its management remains a challenge, with complications including femur head aseptic necrosis and hip joint secondary degenerative arthritis [4]. Ideal management revolves around either fracture fragments fixation or hip joint replacement, with a very little literature being present to support either of the diagnosis [5]. We report an unusual case of posterior hip dislocation with ipsilateral femur neck and posterior wall acetabulum fracture.
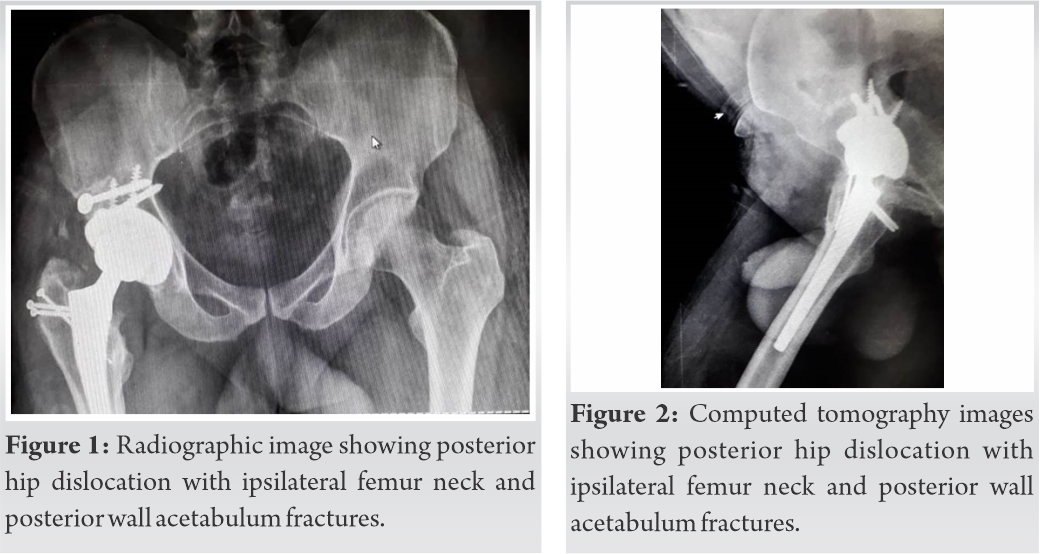
A 45-year-old male patient suffered a high-energy trauma when he was driving the vehicle and was hit from side from a trolley coming from opposite side on his right side. The patient was taken to the emergency block at a local hospital where the patient was stabilized and referred to our hospital for further management. At our hospital after making sure patient is stabilized, skin traction was given and X-rays were done. Following radiographic analysis, the patient was found to be suffering from posterior hip dislocation with ipsilateral femur neck fracture with posterior wall acetabulum fracture (Fig. 1).
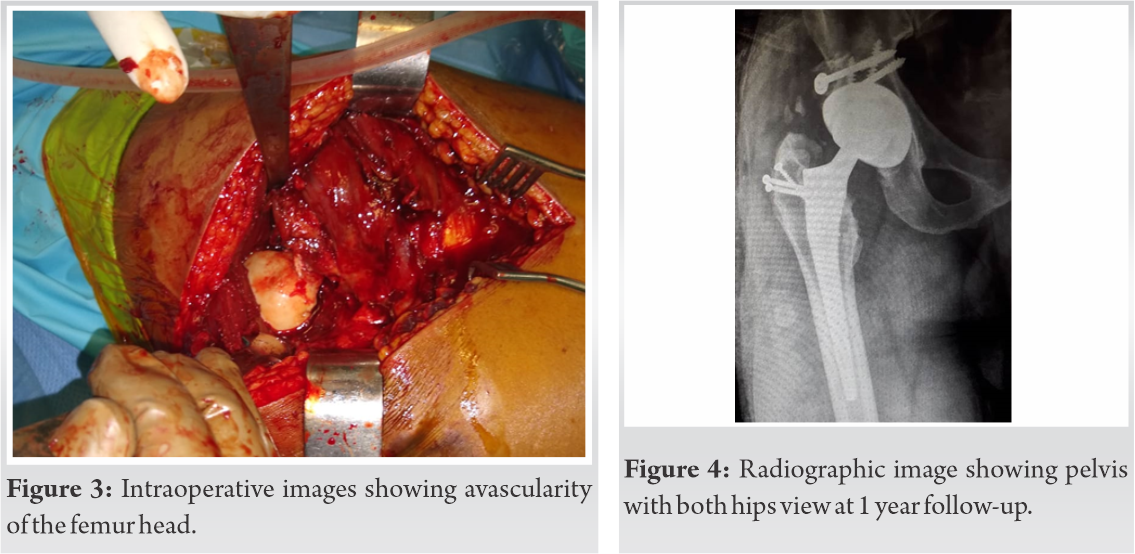
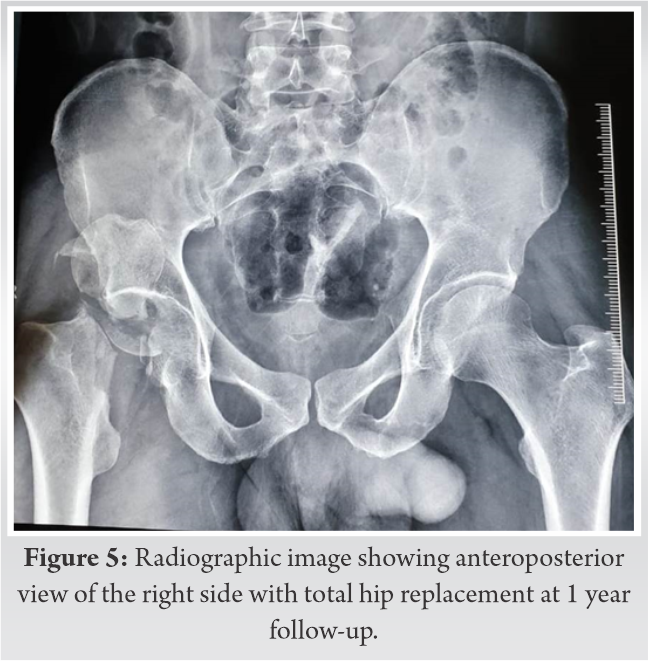
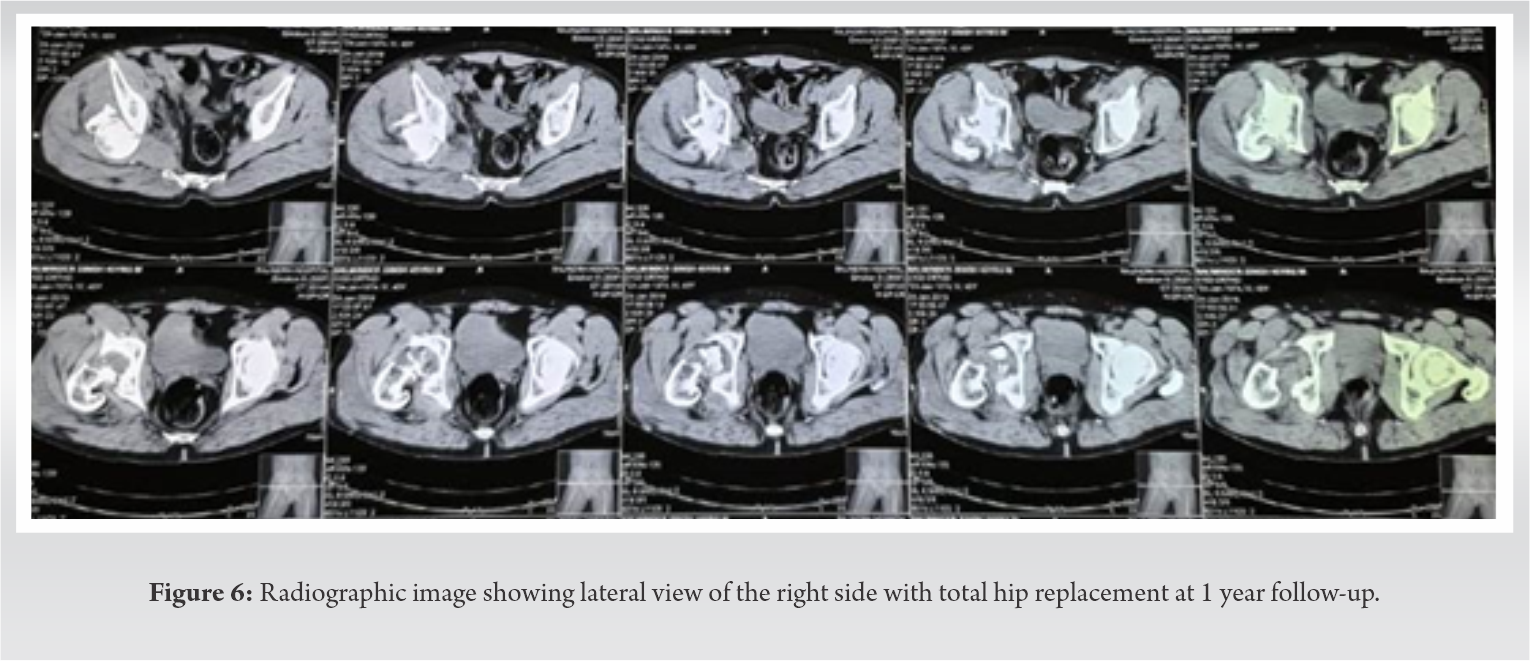
In our case, closed reduction had no effect as posterior segment of the acetabulum along with the associated femur neck fracture, hampered the reduction of the hip joint. Plan for emergent hip reduction and primary surgical fixation of fractures was made. With the patient in floppy lateral position, Kocher-Langenbeck approach was used for exposure and primary fixation of fractures [6]. Extended trochanteric osteotomy had to be done for better intraoperative visualization as the femoral head was present deep within the tissues and thus could not be visualized and to have a supratectal visualization of the acetabulum as fracture was seen to be extending there [7].On opening of the fracture site, posterior wall acetabulum fracture was found to be excessively comminuted non-amenable for fixation and femoral head was found to be avascularized, (Fig. 2) with no bleeding on drilling of the femoral head. Subsequently, plan was changed intraoperatively and uncemented total hip replacement with acetabular defect reconstruction with bone graft from femoral head was done. Postoperatively, the patient received 1.5 g of cefuroxime twice daily for 3 days with Ecosprin and indomethacin started from post-operative day (POD)-1 for prophylaxis of thromboembolism and heterotopic ossification, respectively, for 6 weeks. Rehabilitation was started from next day with high sitting, static quads, and knee bending. From POD-2, the patient was mobilized, with full weight-bearing walking started. At 1-year follow-up, no aseptic loosening was found on anteroposterior view of pelvis with total Harris Hip Score of 91 (Fig. 3) [8].
High-energy motor vehicle mishaps are often associated with complex fracture-dislocations involving the long bones and pelvis [5, 8]. External forces acting on greater trochanter transmit along the femoral neck axis to cause acetabulum fracture [9], with continued transmission of these forces causing concurrent femur neck fracture [10]. These injuries require a prompt and emergent management [11]. To better delineate a fracture pattern, evaluation with specialized radiographic views and non-contrast computed tomography scan is necessary [12].
Post-traumatic complex fracture dislocations, namely, posterior dislocation of hip with ipsilateral femur neck and acetabulum fracture, post a major challenge for the treating surgeon in deciding the best possible management [5, 13]. Patients postoperatively may encounter a serious challenge in terms of the functional outcomes and activities of daily living [3, 11]. Treatment options include either internal fixation or primary arthroplasty [14]. Current literature still lacks clarity on management guidelines for such complicated injuries with either fracture fragments fixation or hip joint replacement and remains to be controversial [15-18]. Secondary to osteosynthesis, aseptic necrosis, and secondary osteoarthritis remain a serious issue in due course of time [13, 19]. Further, a surgeon dealing with such complex cases should be familiar with both management options including fracture fixation and joint replacement, as there remain high chances of conversion to primary joint replacement intraoperatively where femur head is found to be avascularized or there is the presence of arthritic changes in the hip.
In the present study, posterior approach to the hip was used. Posterior approach to the hip aids in simultaneous management of these complex fracture dislocations, where there is a need to have access of both proximal femur and acetabulum at the same time, circumventing any additional trauma to the soft tissues of nearby area [6, 20]. The previous literature cites a total of 18 cases of complicated fracture of femur head/neck with acetabulum, where two were managed with primary fracture fragments fixation and five were managed with primary hip joint replacement [5, 13]. However, we could not find any article relating to the complex trauma of posterior dislocation of the hip with ipsilateral femur neck and acetabulum fracture, as in the present study.
Complex proximal femur and acetabulum fractures necessitate early operative intervention for long-term satisfactory functional outcomes. Both trauma and arthroplasty teams need to be present intraoperatively to aid in optimal management.
Appropriate approach and pre-operative surgical planning could get satisfactory results. Surgeon should not always opt for primary fixation in these types of complex injuries and should keep arthroplasty as the backup to provide satisfactory results.
References
- 1.Birkett J. Description of a dislocation of the head of the femur, complicated with its fracture; with remarks. Clin Orthop Relat Res 2007;458:10-11. [Google Scholar]
- 2.Canale ST, Beaty J. Acute Dislocations, Campbell’s Operative Orthopaedics. 12th ed. United States: Elsevier Health Sciences; 2012. Available from: https://www.elsevier.com/books/campbells-operative-orthopaedics/canale/978-0-323-07243-4. [Last accessed on 2020 Sep 3]. [Google Scholar]
- 3.Tile M. Fractures of the Acetabulum. 4th ed. Philadelphia, PA: Lippincott-Raven; 1996. [Google Scholar]
- 4.Sharma G, Chadha M, Pankaj A. Hip dislocation associated with ipsilateral femoral neck and shaft fractures: An unusual combination and dilemma regarding head preservation. Acta Orthop Traumatol Turc 2014;48:698-702. [Google Scholar]
- 5.Foulk DM, Mullis BH. Hip dislocation: Evaluation and management. J Am Acad Orthop Surg 2010;18:199-209. [Google Scholar]
- 6.Tosounidis TH, Giannoudis VP, Kanakaris NK, Giannoudis PV. The kocher-langenbeck approach: State of the art. JBJS Essent Surg Tech 2018;8:e18. [Google Scholar]
- 7.Harris WH. Advances in surgical technique for total hip replacement: Without and with osteotomy of the greater trochanter. Clin Orthop Relat Res 1980;146:188-204. [Google Scholar]
- 8.Rockwood CA, Green DP, Bucholz RW. Rockwood and Green’s Fractures in Adults. Philadelphia, PA: Lippincott Williams & Wilkins; 2006. [Google Scholar]
- 9.Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9-17. [Google Scholar]
- 10.Thompson VP, Epstein HC. Traumatic dislocation of the hip. J Bone Joint Surg 1951;33:746-92. [Google Scholar]
- 11.Balogh ZJ, Reumann MK, Gruen RL, Mayer-Kuckuk P, Schuetz MA, Harris IA, et al. Advances and future directions for management of trauma patients with musculoskeletal injuries. Lancet 2012;380:1109-19. [Google Scholar]
- 12.Wei L, Sun JY, Wang Y, Yang X. Surgical treatment and prognosis of acetabular fractures associated with ipsilateral femoral neck fractures. Orthopedics 2011;34:348. [Google Scholar]
- 13.Henderson L, Johnston A, Mockford B, Craig B. Posterior hip dislocation and ipsilateral isolated femoral neck fracture: A novel fixation method. J Surg Case Rep 2012;2012:14. [Google Scholar]
- 14.Duygulu F, Calis M, Argun M, Guney A. Unusual combination of femoral head dislocation associated acetabular fracture with ipsilateral neck and shaft fractures: A case report. J Trauma 2006;61:1545-8. [Google Scholar]
- 15.Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg 1988;70:233-9. [Google Scholar]
- 16.Klasen H, Binnendijk B. Fracture of the neck of the femur associated with posterior dislocation of the hip. J Bone Joint Surg Br 1984;66-B:45-8. [Google Scholar]
- 17.Maini L, Mishra P, Jain P, Upadhyay A, Aggrawal A. Three part posterior fracture dislocation of the hip without fracture of the femoral head: Review of literature and a case report. Injury 2004;35:207-9. [Google Scholar]
- 18.Tannast M, Mack PW, Klaeser B, Siebenrock KA. Hip dislocation and femoral neck fracture: Decision-making for head preservation. Injury 2009;40:1118-24. [Google Scholar]
- 19.Dortaj H, Emamifar A. Traumatic hip dislocation with associated femoral head fracture. Case Rep Orthop 2015;2015:1-3. [Google Scholar]
- 20.Farag AW, Shohayeb KA. Intrapelvic dislocation of the head of femur through the obturator foramen associated with ipsilateral fracture femur. J Bone Joint Surg Br 2003;85:1056-8. [Google Scholar]






