
Dual mobility cup prevents post-operative dislocations and secondary procedures which, in turn, helps in getting good functional outcome.
Dr. Lalkar Laxman Gadod,
Flat no A-13, 3rd floor, A Wing, Nitiraj Apartment, Gandham, Nagar,
Near Bombay Sapras Police Station, Khadki – 411 006, Maharashtra, India.
E-mail: lalkargadod@gmail.com
Abstract
Introduction: Neck of femur fractures is the most common fractures in elderly people as they present with osteoporosis. There is a higher chance of proximal femur fracture in a schizophrenic patient as there is a loss of bone mineral density due to a drug-induced increase in the level of prolactin and immobility. Patients with Parkinson’s disease were at higher risk for the development of hip fractures due to gait disturbances and instability.
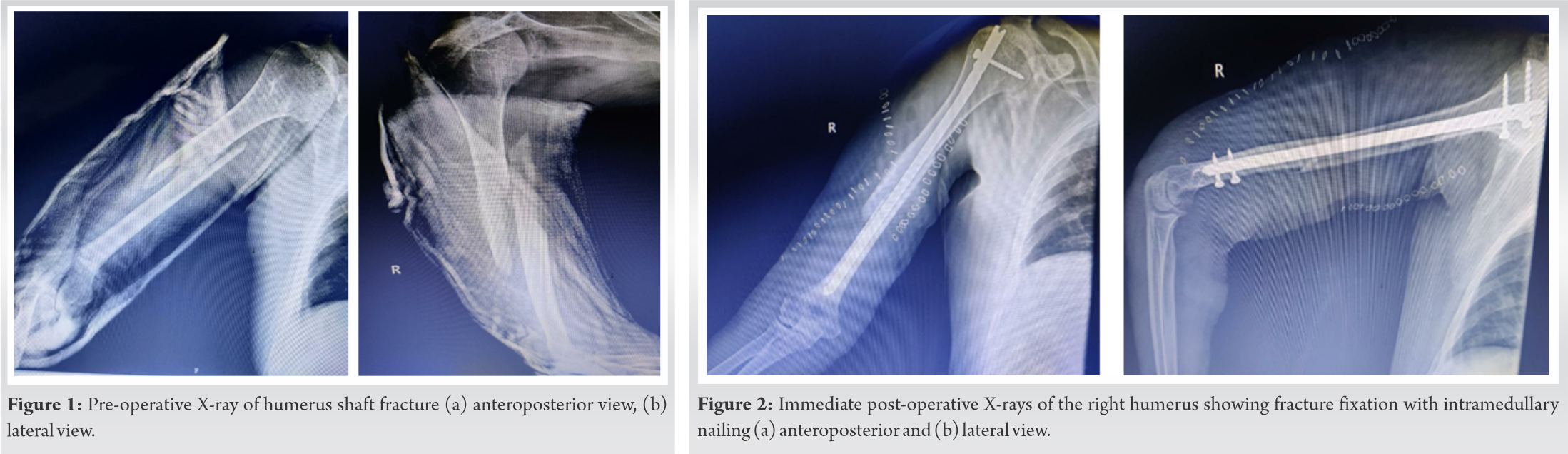
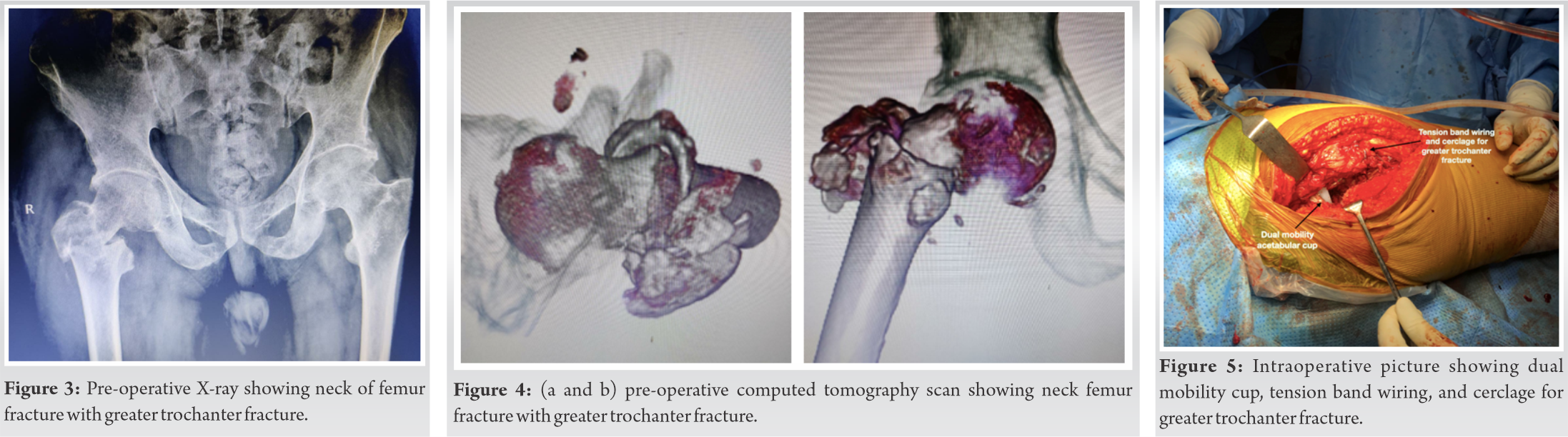
Case Report: A 63-year-old male patient presented with complaints of the right arm pain, swelling, deformity of the right arm, and difficulty in extending the wrist for 3 days. The patient had a history of falls and trauma to the left arm at home. X-ray right arm showed distal one-third spiral humerus fracture for which intramedullary nailing was done. X-ray of the pelvis with both hips showed right neck of femur fracture with associated greater trochanter (GT) fracture. We managed with total hip replacement using a dual mobility cup and tension band wiring for GT fracture. Postoperatively, the patient has a good range of motion at the hip. The functional outcome is good as per Harris’s hip score.
Conclusion: Neck femur fractures in elderly patients with associated comorbidities such as schizophrenia and parkinsonism are best managed with total hip replacement using a dual mobility cup. It avoids the risk of dislocation in high-risk patients and prevents secondary procedures. Careful clinical and radiological examination of the pelvis is very essential even in asymptomatic patients with a history of trauma to prevent delayed diagnosis of these types of fractures in patients with schizophrenia and parkinsonism.
Keywords: Neck of femur fracture, Parkinsonism, schizophrenia, dual mobility cup, total hip replacement.
Neck of femur fractures is the most common fractures in elderly people as they present with osteoporosis. These are intracapsular fractures and are associated with low-energy trauma like falls. It also occurs in young population due to motor vehicle accident and fall from height. Risk factors for the neck of femur fractures are female gender, immobility, and decrease mineral density. It accounts for 1.6 million hip fractures annually. About 90% of proximal femur fractures are of the neck of the femur including trochanteric fractures, more common in females than males over the age of 50 years. They consist of 2% of proximal femur fractures in 50 years below age group [1]. High rate of mortality is seen in patients with hypertension, mental illness (schizophrenia and parkinsonism), cardiac disease, renal insufficiency, diabetes, and smoking [2]. There is a higher chance of proximal femur fracture in a schizophrenic patient as there is a loss of bone mineral density due to a drug-induced increase in the level of prolactin and immobility [3]. Patients with Parkinson’s disease were at higher risk for the development of hip fractures due to gait disturbances and instability. It is associated with motor symptoms such as muscular rigidity, resting tremors, bradykinesia, postural, and gait impairment. As there is an increased frequency of falls in Parkinson’s disease patients, the risk of fracture is also increased. These patients also have osteoporosis due to immobilization, reduced activity, and Vitamin D deficiency [4]. The treatment options available for these patients include CC screw fixation, dynamic hip screws (DHS) plating, bipolar hemiarthroplasty, and total hip replacement. Operative management helps in early mobilization and reduces chances of pulmonary infection, bedsore, and deep vein thrombosis. Patients with parkinsonism have higher chances of dislocation and implant failure after total hip replacement and bipolar hemiarthroplasty. Another option for the management of neck femur fracture in elderly patient associated with schizophrenia and parkinsonism is total hip replacement using dual mobility prosthesis and tension band wiring (TBW) if there is a greater trochanteric (GT) fracture, which helps in early mobilization and prevents post-operative complication like dislocation [4]. Primary total hip replacement for the treatment of neck of femur fracture with GT fracture in elderly patient with parkinsonism and schizophrenia is difficult to perform due to distorted anatomy, a poor bone stock which poses problems during the femoral cut, cementing, and implantation. Nowadays, with the improved implant designs, it is possible to perform these types of surgeries with minimal complications.
A 63-year-old male patient came with complaints of the right arm pain, swelling, deformity of the right arm, and difficulty in extending the wrist for 3 days. The patient had a history of falls and trauma to the left arm at home. The patient had gone to some hospital where they had given slab and referred to our institute. On examination, the deformity was present in the right arm with wrist drop and mild tenderness in the right hip. X-ray right arm showed distal one-third spiral humerus fracture (Fig. 1a, b). The patient was a known case of parkinsonism, schizophrenia, and hypertension on medications. The patient was operated on with humerus nailing and radial nerve exploration was done by the plastic surgeon, which was intact (Fig. 2a, b). X-ray and computed tomography scan of the pelvis with both hips showed right neck of femur fracture with associated GT fracture (Fig. 3, 4). As the patient was old requiring early mobilization had pain and difficulty in walking, we planned for total hip replacement surgery with a dual mobility cup as the patient was a high risk for dislocation.
The patient was operated on in a lateral position under spinal anesthesia using the posterior approach. Initially, acetabular preparation was done, then the cerclage wires passed in the medial cortex of the proximal femur after the drilling using k-wires and then passed under the vastus lateralis muscle (Fig. 5).
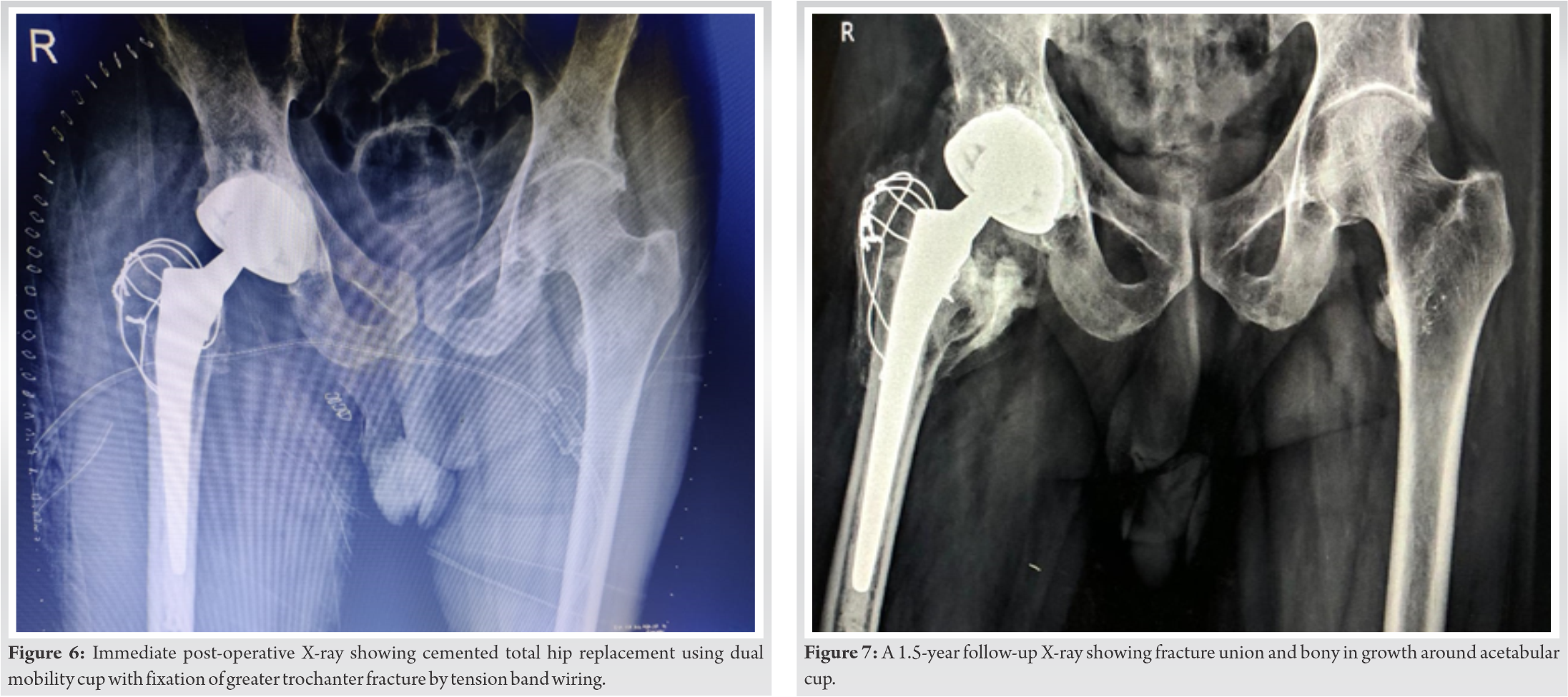
The femoral preparation was done using sequential rasps. The cemented total hip arthroplasty was done using Zimmer implant of the acetabulum (cotyle double mobilite size of 56–57), femoral component (femoral stem size of 13 and femoral head size of 28), and dual mobility polyethylene liner for the head 28 and cup 56–57. After the implant fixation and hip reduction, the TBW was passed from the tip of the GT through the abductors and distally taken out from the lateral cortex of the femur. Now, both the cerclage wires and TBW were tightened together. Intraoperatively, stability of the hip and the GT was stable. After putting the drain, the wound was closed in layers. The post-operative X-ray showed well-fixed femoral and acetabular components with proper inclination (Fig. 6). Weight-bearing was started from the 2nd post-operative day with the walker. After 1.5 years of follow-up, the patient is now comfortable with no pain and difficulty in walking and showing fracture union and bony in growth around stem and acetabular cup (Fig. 7). The patient has a good range of motion at the hip. The functional outcome is good as per Harris’s hip score.
Fractures around the hip in elderly osteoporotic patient with parkinsonism and schizophrenia are challenging. Risk factors for the neck of femur fractures are female gender, decrease in mobility, and decrease mineral density [1]. High rate of mortality is seen in patients with hypertension, mental illness (schizophrenia and parkinsonism), cardiac disease, renal insufficiency, diabetes, and smoking [2]. There are high chances of hip fracture which is seen in schizophrenic patients as there is the loss of bone mineral density due to a drug-induced increase in the level of prolactin and immobility , As is seen in our case [3]. Various treatment options for the neck of femur fracture are CC screw fixation, DHS plating, bipolar hemiarthroplasty, and total hip arthroplasty. Initially, bipolar hemiarthroplasty was not recommended for the neck of femur fracture with Parkinson’s disease due to the high mortality rate and chances of dislocation [4,5]. Another option for patients with Parkinson’s disease and schizophrenia is total hip arthroplasty using a dual mobility cup which prevents dislocation and reduces further complication. Bassiony et al. [4] in their study used a dual mobility cup in patients with a neurological deficit (Parkinson’s disease) and concluded that a dual mobility cup is a good option for patients with instability and obtained good functional outcome. According to Coughlin and Tempelton [5], very poor results, there was seen after arthroplasty in patients with Parkinson’s disease who were not mobilized in the 1st week after surgery (37% dislocation, 49% of pressure ulcers, and 75% mortality). As in our case, we mobilized the patient within a week after surgery. Karadsheh et al. [6] in their study did internal fixation for valgus impacted neck fracture in parkinsonism patients and concluded that they are at higher risk of fixation failure as in our case, we did dual mobility total hip arthroplasty considering the age of patient, type of fracture, and chances of dislocation. According to Gaillard et al. [7], dual mobility articular surfaces are better than traditional bearing surfaces as they provide good stability and a high survival rate in both primary and revision surgeries. Onochi et al. [8] in their study used freedom constrained liner for recurrent dislocation, in a schizophrenic patient who underwent dual mobility total hip arthroplasty already and concluded that freedom liner may provide salvage solution for joint instability in dual mobility total hip arthroplasty as in our case till the time no history of dislocation. Gianluca et al. [9] found that dual mobility total hip arthroplasty in femur neck fracture has good clinical outcome and low rate of dislocation. The proper wise selection of implants, meticulous soft-tissue dissection, and surgery help in getting a better outcome in patients with neck of femur fracture with GT fracture with parkinsonism and schizophrenia requiring a total hip replacement.
Neck femur fractures in elderly patients with associated comorbidities such as schizophrenia and parkinsonism are best managed with total hip replacement using a dual mobility cup. It avoids the risk of dislocation in high-risk patients and prevents secondary procedures. Careful clinical and radiological examination of the pelvis is very essential even in asymptomatic patients with a history of trauma to prevent delayed diagnosis of these types of fractures in patients with schizophrenia and parkinsonism.
Dual mobility cup is essential in patients with schizophrenia and parkinsonism undergoing total hip replacement which avoids the risk of dislocation.
References
- 1.Filipov O. Epidemiology and social burden of the femoral neck fractures. J IMAB 2014;20:516-8. [Google Scholar | PubMed]
- 2.Iglesias SL, Gentile L, Vanoli F. Femoral neck fractures in the elderly: From risk factors to pronostic features for survival. J Trauma Crit Care 2017;1:16-21. [Google Scholar | PubMed]
- 3.Hummer M, Malik P, Gasser RW, Hofer A, Kemmler G, Naveda RC, et al. Osteoporosis in patients with schizophrenia. Am J Psychiatry 2005;162:162-7. [Google Scholar | PubMed]
- 4.Bassiony AA, Gameel S. The dual mobility hip arthroplasty for hip fracture in Parkinson’s disease. Open J Trauma 2020;4:32-5. [Google Scholar | PubMed]
- 5.Coughlin L, Tempelton J. Hip fractures in patients with Parkinson’s disease. Clin Orthop Relat Res 1980;148:192-5. [Google Scholar | PubMed]
- 6.Karadsheh MS, Weaver M, Rodriguez K, Harris M, Zurakowski D, Lucas R. Mortality and revision surgery are increased in patients with Parkinson’s disease and fractures of the femoral neck. Clin Orthop Relat Res 2015;473:3272-9. [Google Scholar | PubMed]
- 7.Gaillard R, Kenney R, Delalande JL, Batailler C, Lustig S Ten-to 16-year results of a modern cementless dual-mobility acetabular implant in primary total hip arthroplasty. J Arthroplasty 2019;34:2704-10. [Google Scholar | PubMed]
- 8.Onochi Y, Fukui K, Kaneuji A, Ichiseki T, Wang X, Kawahara N. Dual mobility acetabular construct with freedom constrained liner for treatment of recurrent dislocations after total hip arthroplasty: A case report and literature review. Int J Surg Case Rep 2020;75:94-9. [Google Scholar | PubMed]
- 9.Gianluca C, Alessandro M, Mirco C, Francesco MK, Luigi M. Dual mobility total hip arthroplasty in the treatment of femoral neck fractures: A retrospective evaluation at mid-term follow-up. Acta Biomed 2019;90:98-103. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report
March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement
June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study
March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report
February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report