
Ventral scapular osteochondroma should always be considered as a differential diagnosis for a young child presenting with a winged scapula.
Dr. Nihar Modi,
Department of Orthopaedics,
Grant Government Medical College and Sir JJ Group of Hospitals,
Mumbai, Maharashtra, India.
E-mail: modi.nihar95@gmail.com
Introduction:Winging of scapula is defined as a failure of dynamic stabilizing structures that anchor the scapula to the chest wall, leading to prominence of the medial border of scapula. It could be primary, secondary, or voluntary. Primary winging could be true winging due to neuromuscular causes or pseudo-winging due to osseous or soft-tissue masses. A scapular osteochondroma is a very rare presentation site and causes pseudo-winging leading to pushing away of the scapula away from the chest wall presenting as medial border prominence. Here, we are reporting a rare case of a scapular osteochondroma causing a pseudo-winging of the scapula.
Case Report: A 2-year-old male child presented with painless, immobile, and non-fluctuant swelling over the left scapular region, insidious in onset and progressive in nature. On examination, a non-tender, immobile swelling was palpable with a painless and unrestricted range of motion at the shoulder joint. After evaluating radiographs and CT scan, the patient was diagnosed to have a ventral scapular osteochondroma leading to pseudo-winging of the scapula.
Conclusion: Despite the rarity, a differential diagnosis of a scapular osteochondroma should be kept in mind while examining a young child presenting with a winged scapula.
Keywords: Scapula, osteochondroma, pseudo-winging.
Winging of scapula or scapula alata is defined as a failure of dynamic stabilizing structures that anchor the scapula to the chest wall, leading to prominence of the medial border of scapula [1, 2]. Winging may be described as primary, secondary, or voluntary. Primary scapular winging occurs as a result of anatomic disorders (neurologic, soft tissue or osseous origin) that directly affect the scapulothoracic articulation. Secondary scapular winging occurs due to abnormality in glenohumeral joints. Voluntary winging occurs due to psychological causes and is quite rare [3]. Primary winging comprises true winging which occurs due to neuromuscular causes such as long thoracic nerve palsy and pseudo-winging which occur due to osseous and soft-tissue masses over the scapula and thoracic cage [4]. Scapular osteochondroma is a rare cause of pseudo-winging which pushes the scapula away from the chest wall and inhibits muscle function [2]. We report a case of scapular osteochondroma arising from the ventral surface and leading to pseudo-winging of the scapula.
A 2-year-old male child presented to the outpatient clinic with a painless swelling and deformity over the left scapular region which was insidious in onset and gradually progressing over the past 3 months. The child was first born, with no siblings and there was no history of a similar condition in any of the family members. The child had developmental milestones appropriate for his age. There was no history of trauma and no swelling elsewhere in the body. There was no history of fever or weight loss. On clinical examination, the left scapula looked asymmetrical as compared to the right, with the medial border of the left scapula seeming prominent and elevated from the thoracic cage (Fig. 1). A swelling was palpable 5 × 4 × 4 cm in size which was non-tender, immobile, arising from underlying bone and non-adherent to the overlying skin. It was non-fluctuant and non-compressible. Skin overlying the scapula was intact. Range of motion of shoulder and cervical spine was normal and unrestricted. On neurological examination, the sensory, motor, and reflex testing of bilateral upper limbs were within normal limits. There was no sign of compression of nerves, vessels, or lymphatic system.
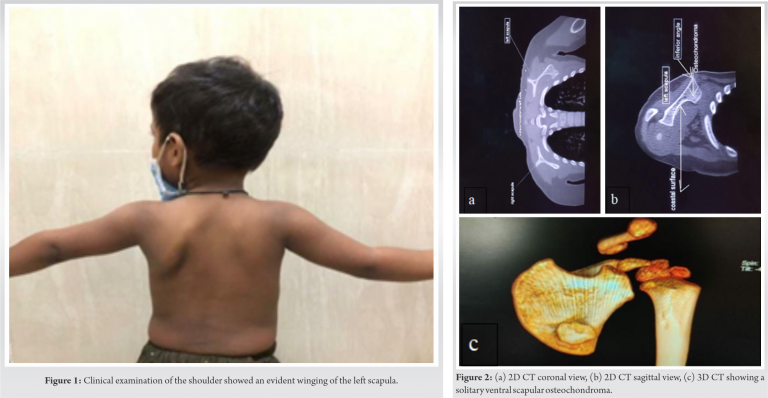
Plain radiographs and computed tomography (CT) scan (Fig. 2a, 2b, 2c) were done. The radiograph showed a bony lesion and the CT scan demonstrated a well-corticated bony excrescence arising from ventral surface of the left lower part of body of the scapula, 3 cm proximal to inferior angle and no associated fracture of the bony stalk. In this case, we had a skeletally immature 2-year-old male child who was asymptomatic apart from a painless mass over the scapula with no associated complications, and hence, was planned to be managed conservatively and followed up regularly at 6 monthly intervals till skeletal maturity. This was planned keeping in mind the fact that a benign ventral scapular osteochondroma ceases to grow after the growth plate has fused (once skeletal maturity has been reached) and is very rarely associated with complications such as fracture of the bony stalk, nerve impingement, and rapid enlargement associated with malignancy.
Osteochondroma is a developmental physeal growth defect which presents as a pedunculated or sessile cartilage-capped bony projection arising on the external surface of the bone containing a marrow cavity that is in continuity with that of the underlying bone and grows through endochondral ossification beneath the periosteum [5, 6, 7]. Osteochondroma represents 30% of all primary bone tumors, 45% of benign bone tumors and is the most common benign bone tumor in humans [5, 8]. It is most commonly seen around metaphysis of long bones. The proximal humerus and knee constitute 90% of occurrence sites [6]. Flat bones such as the pelvis and the scapula are rare sites for osteochondroma with 3–4.5% involvement of the scapula [9]. Osteochondromas are common in young patients under 30 years of age and increase in size in the first decade of life [10]. Incidence is higher in males probably because females tend to have a milder phenotype and hence is easily overlooked [11]. Ventral scapular osteochondroma is usually painless, but may sometimes present with pain, decreased range of motion especially abduction, crepitus, and snapping. Complications such as fracture of bony stalk, nerve impingement, and bursal formation may occur [5]. Very rarely, in 1% of cases, a malignant transformation may occur characterized by sudden increase in size and pain [5]. Usually, a benign osteochondroma ceases to grow when the growth plate closes at puberty, and a sudden increase in size at puberty should raise a concern for possible malignancy [10]. However, the patient mentioned in the case report was only 2 years old and had none of these symptoms. True winging of scapula is generally considered to be due to neuromuscular disorders like serratus anterior palsy which increases on forward flexion of the arm and is a dynamic kind of winging. Pseudo-winging is due to non-neuromuscular causes such as lesions over the scapula and adjacent thoracic cage and kyphoscoliotic deformities of upper and mid-thoracic spine with osteochondroma being the most common tumor cause among tumors. Pseudo-winging is a static kind of winging which is characteristically present at rest and does not increase with forward flexion of arm [4]. Osteochondromas are often seen as an incidental finding, as the lesions tend to present as asymptomatic, slow-growing masses on the involved bone [7]. AP and lateral radiographs are sufficient to make the diagnosis, but a CT scan gives us a better anatomical understanding of the lesion and helps in planning future management [5]. Histopathological evaluation shows endochondral ossification and cartilage with disorganized growth plate [12]. Diagnosis of pseudo-winging due to scapular osteochondroma is often missed. A summary of recent case reports published is presented in (Table 1). A ventral scapular osteochondroma causing pseudo-winging is usually managed with surgical excision of the entire lesion with stalk, unless skeleton is immature [7]. Patients can be followed up with routine clinical examinations and yearly radiographs until skeletal maturity. On subsequent outpatient department visits, new onset of symptoms such as nerve impingement, sudden onset of increased pain, or rapid increase in size of the lesion should be checked for, which could indicate a possible malignancy [5]. Prognosis of a solitary ventral osteochondroma after excision is excellent. Surgical excision helps to achieve a complete resolution and relief of mechanical symptoms, with a full range of motion in the affected shoulder [7]. Very rarely, tumor relapse is seen when unclear resection margins are left [7].
This case report highlights the importance of considering ventral scapular osteochondroma leading to pseudo-winging of scapula as a differential diagnosis, in a case of a young child presenting with winged scapula. A high degree of suspicion accompanied by proper clinical examination helps in diagnosing this rare entity.
Ventral scapular osteochondroma should always be considered as a differential diagnosis for a young child presenting with a winged scapula.
References
- 1.Danielsson LG, El-Haddad I. Winged scapula due to osteochondroma. Report of 3 children. Acta Orthop Scand 1989;60:728-9. [Google Scholar]
- 2.Gooding BW, Geoghegan JM, Wallace WA, Manning PA. Scapular winging. Shoulder Elbow 2014;6:4-11. [Google Scholar]
- 3.Kuhn JE, Plancher KD, Hawkins RJ. Scapular winging. J Am Acad Orthop Surg 1995;3:319-25. [Google Scholar]
- 4.Tittal P, Pawar I, Kapoor SK. Pseudo-winging of scapula due to benign lesions of ventral surface of scapula-two unusual causes. J Clin Orthop Trauma 2015;6:30-5. [Google Scholar]
- 5.Chillemi C, Franceschini V, Ippolito G, Pasquali R, Diotallevi R, Petrozza V, et al. Osteochondroma as a cause of scapular winging in an adolescent: A case report and review of the literature. J Med Case Rep 2013;7:220. [Google Scholar]
- 6.Barnawal SP, Gandhi BS, Rathod A. Pseudo-winging of scapula due to ventral scapular osteochondroma: A case report and literature review. J Orthop Case Rep 2020;10:69-72. [Google Scholar]
- 7.Alatassia R, Koabana S, Almugebelb I, Alshehri A. Scapular osteochondroma with winging: A case report. Int J Surg Case Rep 2018;45:138-42. [Google Scholar]
- 8.Rao VS, Pai MR, Rao RC, Adhikary MM. Incidence of primary bone tumours and tumour like lesions in and around Dakshina Kannada district of Karnataka. J Indian Med Assoc 1996;94:103-4. [Google Scholar]
- 9.Chun DI, Cho JH, Choi IH, Yi Y, Kim JY, Kim JH, et al. Osteochondroma of ventral scapula associated with chest pain due to rib cage compression: A case report. Medicine (Baltimore) 2018;97:e0510. [Google Scholar]
- 10.Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008;3:3. [Google Scholar]
- 11.Legeai‐Mallet L, Munnich A, Maroteaux P, Le Merrer M. Incomplete penetrance and expressivity skewing in hereditary multiple exostoses. Clin Genet 1997;52:12-6. [Google Scholar]
- 12.Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar]
- 13.Fageir MM, Edwards MR, Addison AK. The surgical management of osteochondroma on the ventral surface of the scapula. J Pediatr Orthop B 2009;18:304-7. [Google Scholar]
- 14.Tungdim PH, Singh II, Mukherjee S, Pertin T. Excision of solitary osteochondroma on the ventral aspect of left scapula presenting as pseudowinging in a 4-year-old boy: A rare case report. J Orthop Case Rep 2017;7:36-40. [Google Scholar]
- 15.Prakash S, Kalra P, Khan Y, Dhal A. Ventral scapular osteochondroma excision through triangle of auscultation: A case series. J Orthop Surgery (Hong Kong) 2020;28(1):2309499019892848. [Google Scholar]








