
Solitary osteochondroma can present in the bones of the foot and require surgical treatment.
Dr. Nikolaos Laliotis,
Department of Orthopaedics,
Inter Balkan Medical Center, Thessaloniki, Greece.
E-mail: nicklaliotis@gmail.com
Introduction : Solitary osteochondromas are extremely rare in the bones of the foot. In the growing skeleton, few cases affecting the metatarsals and the talus have been reported. At present, there have been no reports of osteochondromas affecting the cuneiforms.
Case Report: We report the case of a 13-year-old male patient. He presented with marked prominences in the plantar surface of his left foot and pain while participating in sporting activities. Radiological examination with X-rays, computed tomography (CT) scan, and magnetic resonance imaging revealed two solitary osteochondromas growing from the medial cuneiform and the head of the 1st metatarsal. The patient was treated surgically by excision of the osteochondromas. Histological examination confirmed the diagnosis of osteochondromas. He had an uneventful recovery and returned to his sporting activities.
Conclusion: Solitary osteochondroma can present in the cuneiform and metatarsal of a growing adolescent. CT scan is useful for the accurate diagnosis and surgical removal of the tumor.
Keywords: Osteochondroma, foot, metatarsal, cuneiform, child.
Osteochondromas are the most common benign lesions, which affect the metaphyseal area of long bones. They can be found in the feet of children diagnosed with multiple exostoses. Solitary osteochondromas of the foot are rare and only sporadic cases are described, affecting the calcaneum, talus, metatarsals, and phalanges [1, 2, 3, 4, 5]. We report the case of a 13-year-old boy, with two distinct osteochondromas. The first was arising from the 1st cuneiform and the other from the 1st metatarsal head. We present the clinical and radiological investigation and the result of the surgical excision. Early excision is beneficial for the daily activities of young adolescents.
A young adolescent attended our outpatient department seeking advice on the unusual growth of his left foot. He was a healthy and active young boy, without other underlying pathology. He reported pain during daily activities, in particular while playing football. He was wearing shoes that were larger in size than anticipated for his body. On clinical examination, there was a marked prominence in the medial and plantar arch of the foot and the plantar area of the 1st metatarsal. The foot had minor skin sclerosis in the area of the 1st metatarsal. On palpation, two firm solid masses were found, one plantar and lateral to the head of the 1st metatarsal and the other in the plantar surface of the cuneiforms. No other prominences were found in the skeleton. His ability to tip toe and jump on his left foot was limited. He expressed discomfort in the passive movements of the 1st MTP joint. Plain X-ray revealed two distinct well delineated tumors. They both had marked calcification, extending in the plantar surface. One was located in the head of the 1st metatarsal and the other in the area of the cuneiforms. The tumor of the 1st metatarsal was protruding plantar and lateral. It extended to the 1st MTF joint, with enlargement of the joint. The growth plate of the metatarsal and of the proximal phalanx was not affected. The other tumor found on the cuneiform appeared as an osteosclerotic lesion with minimal widening of the joints between the cuneiforms. A computed tomography (CT) scan was performed confirming the presence of two giant osteochondromas. The first was arising from the 1st metatarsal, communicating with the metatarsal bone. The medial sesamoid was articulating with the osteochondroma, in the plantar area.
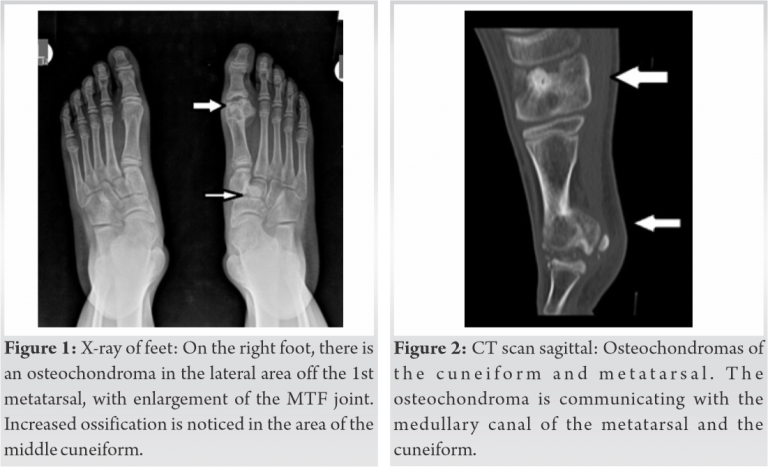
The second osteochondroma was found in the area of the cuneiforms, with clear borders. It was communicating with the medial cuneiform, distorting the normal relation of the cuneiforms with the navicular and the metatarsals.
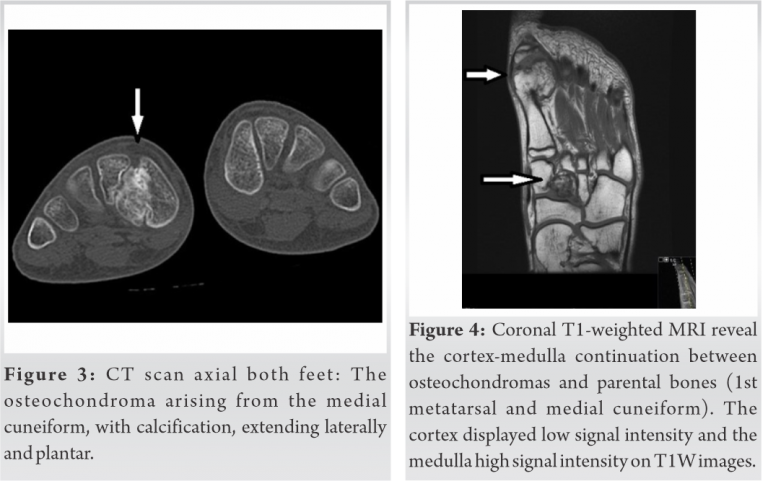
Further investigation with magnetic resonance imaging (MRI) was used, to have more information of the cartilaginous portion of the osteochondromas. We performed radiological examination on the lower limbs, to exclude the possibility of multiple osteochondromas located elsewhere. No other osteochondromas were found. After a discussion with both the patient and his parents, surgery was recommended. During the operation, we first removed the osteochondroma located on the 1st metatarsal, with care to protect the flexor muscles and the sesamoids. A large osteochondroma 3 × 4 cm was removed. Then using a medial approach, we identified the borders of the cuneiforms and removed the second osteochondroma from the 1st cuneiform. The boundaries of the normal cuneiform were undistinguished from the osteochondroma. The amount of osteochondroma removed was estimated so that the remaining cuneiform was resembling the normal cuneiform. We used fluoroscopy in attempt to locate the edges of the normal cuneiform but it had limited success. The second osteochondroma was removed in pieces. The mass removed was a little larger than the osteochondroma of the metatarsal, measuring 4 × 4 cm.
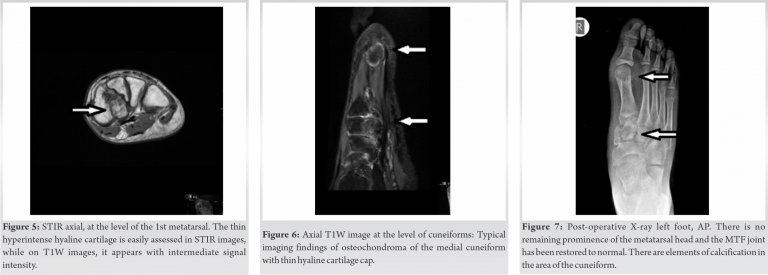
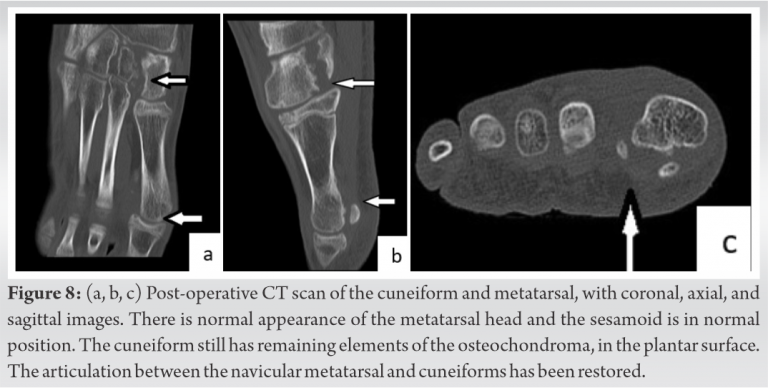
Both specimens were sent for pathologic examination confirming the diagnosis of two osteochondromas. Our patient had an uneventful recovery, with a 4-week period of partial weight-bearing. He is being regularly evaluated in our clinic. Six months after the operation, he stated that he could easily participate in football activities, playing for his city team. A post-operative X-ray and CT scan were performed showing restoration of the shape of the 1st metatarsal with normal position of the sesamoids. In the area of the cuneiforms, remnants of the osteochondroma were found in the plantar surface.
The young patient was very happy with the cosmetic appearance of his feet. There is minimal enlargement of the foot. We will continue to follow up the boy, to ensure that there is no recurrence or other disability in his foot.
Osteochondromas affecting the foot are extremely rare. Osteochondromas usually are found in the foot in children with multiple exostoses. Solitary osteochondromas affecting the foot are sporadically reported, affecting the calcaneum, talus, or metatarsals [1, 2, 6, 7]. Despite that osteochondromas develop during childhood, they remain undiagnosed until adolescent or in adult life. Delayed diagnosis has also been reported for solitary osteochondromas located in the hand [8]. Symptoms are usually related with the disturbance of weight-bearing. In the foot, the lesions are palpable under the skin. They are not covered by muscle as in the femur so are easily identified. As they grow, they distort the alignment of the metatarsals. They may affect the normal growth, creating short rays. A solitary osteochondroma of the 4th metatarsal was reported in a 13-year-old girl, causing deformation of the adjacent metatarsal. After excision of the osteochondroma, the cosmetic result was satisfactory. The authors report few cases of osteochondromas located in the metatarsals in adolescents [5]. Giant solitary osteochondromas have been described in the calcaneum of adults, where they must be distinguished from sarcomas, in cases of recurrence or if they grow rapidly [4, 9]. A 15-year-old boy presented with tarsal tunnel syndrome, from the pressure of an osteochondroma of the talus [10]. The patient had a similar clinical presentation to one of the three cases with talar osteochondromas, reported by Kumar et al. [2]. An 8-year-old boy presented with a history of repeated ankle sprains and limited movements of the subtalar joint. A solitary osteochondroma of the talus at the sinus tarsi was found. The authors reported in a literature review, cases of solitary osteochondromas of the talus, with only 10 cases diagnosed in skeletally immature patients [11]. A case of giant osteochondroma in the neck of the talus was reported in a 19-year-old athlete [12]. A 12-year-old girl presented with a rapidly progressing mass of the sinus tarsi. After an initial biopsy, the tumor was excised and the histological diagnosis of a solitary synovial osteochondroma was made [13]. Recently, a dorsal navicular osteochondroma found in an 11-year-old female, was reported. Investigation with X-rays, CT, 3D reconstruction, and MRI was performed before surgery. A small pedunculated tumor was excised and histology confirmed the diagnosis of osteochondroma [3]. A giant solitary osteochondroma of the 5th metatarsal with erosion of the adjacent metatarsal was found in a 20-year-old patient and treated with excision [14]. Osteochondromas of the metatarsal have been reported in adults [6, 7, 15]. We have not found any cases of solitary osteochondroma affecting the cuneiform. Radiological examination is characteristic for an osteochondroma. The lesion is an osseous enlargement of cortical and medullary bone which grows in a vertical direction to the normal bone axis. There are clear boundaries of the exostosis, with areas of calcification. It is important to identify the connection of the osteochondroma with the medullary canal of the host bone. The lesion is bigger than it appears on radiological imaging since the cartilaginous cup is not obvious. A CT scan can help to clarify the exact boundaries of the lesion. It is very helpful for pre-operative planning as it accurately shows the dimensions and the location of the osteochondroma. 3-D reconstruction can assist with the exact position of the osteochondroma. It helps to plan the surgical removal with safety [9, 11, 14]. MRI is used in cases where there has been recent enlargement of the tumor, with suspicion for sarcoma (chondrosarcoma or parosteal osteosarcoma). When there is increased thickness of the cartilaginous cap in an osteochondroma, we proceed in MRI investigation. This is important for adults with enlargement of the tumor, atypical calcification, or unclear borders of the osteochondroma. We performed MRI on our patient, to add more information for the lesion, since the presence of two solitary osteochondromas in the foot is extremely rare. MRI is useful to clarify the cartilaginous borders and help in accurate preoperative planning [4, 9]. Surgical treatment is the method of choice when treating a giant osteochondroma. It is easy to remove an osteochondroma that is pedunculated, but difficult when it grows from a small rectangular shaped bone, like the cuneiform. In the metatarsal, we tried to protect the flexor muscles and the sesamoids, to minimize further discomfort of our patient. Recurrence is an exception in the surgical treatment of osteochondromas and when it appears, we must evaluate the patient for the accurate diagnosis [9].
We report on a skeletally immature patient with two distinct osteochondromas of the metatarsal and the cuneiform. We describe the clinical and radiological examination. Surgical excision of the osteochondromas relieved the symptoms.
Solitary osteochondromas are very rare in the foot. They present as firm mass that disturbs the normal weight-bearing and interrupt the normal shape and alignment of the bones of the foot. We present a unique case of two osteochondromas of the medial cuneiform and 1st metatarsal. A CT scan was essential to evaluate the size and position of the osteochondromas. Surgery is the method of treatment. It was difficult to accurately determine the boundaries of the osteochondroma in a small host bone as the cuneiform. Early removal is important to avoid bone deformities.
References
- 1.Fuselier CO, Binning T, Kushner D, Kirchwehm WW, Rice JR, Hetherington V, et al. Solitary osteochondroma of the foot: An in-depth study with case reports. J Foot Surg 1984;23:3-24. [Google Scholar]
- 2.Kumar S, Dhammi IK, Jain AK, Shahi P. Osteochondroma of the talus: Three varying cases. BMJ Case Rep 2020;13:e237670. [Google Scholar]
- 3.Turati M, Bigoni M, Omeljaniuk RJ, Griffet J, Zatti G, Courvoisier A. Pediatric navicular dorsal osteochondroma: A rare case of navicular-cuneiform impingement. J Pediatr Orthop B 2019;28:602-6. [Google Scholar]
- 4.Blitz N, Lopez K. Giant solitary osteochondroma of the inferior medial calcaneal tubercle: A case report and review of the literature. J Foot Ankle Surg 2008;47:206-12. [Google Scholar]
- 5.Patil SD, Patil VD, Khan A, Khanore C. Correction of a forefoot deformity caused by a large, solitary metatarsal osteochondroma in an adolescent: A case report. J Foot Ankle Surg 2016;55:427-33. [Google Scholar]
- 6.Jadhav PU, Banshelkikar SN, Seth BA, Goregaonkar AB. Osteochondromas at Unusual Sites-case series with review of literature. J Orthop Case Reports 2016;6:52-4. [Google Scholar]
- 7.Molitor PJ, Myint S. An unusual solitary osteochondroma arising from the first metatarsal bone. Foot 1997;7:37-9. [Google Scholar]
- 8.Laliotis NA, Crysanthou CK, Konstandinidis PA. Solitary osteochondroma of the capitate, in a child. J Clin Orthop Trauma 2018;9:S136-9. [Google Scholar]
- 9.Koplay M, Toker S, Sahin L, Kilincoglu V. A calcaneal osteochondroma with recurrence in a skeletally mature patient: A case report. Cases J 2009;2:7013. [Google Scholar]
- 10.Won SH, Kim J, Min TH, Chun DI, Yi Y, Han SH, et al. Tarsal tunnel syndrome secondary to osteochondroma of the calcaneus: A case report. BMC Musculoskelet Disord 2020;21:491. [Google Scholar]
- 11.Andreacchio A, Marengo L, Canavese F. Solitary osteochondroma of the sinus tarsi. J Pediatr Orthop B 2018;27:88-91. [Google Scholar]
- 12.Galanis V, Georgiadi K, Balomenos V, Tsoucalas G, Thomaidis V, Fiska A. Osteochondroma of the talus in a 19-year-old female: A case report and review of the literature. Foot (Edinb) 2020;42:101635. [Google Scholar]
- 13.Lui TH. Giant solitary synovial osteochondroma of the subtalar joint. J Foot Ankle Surg 2016;55:183-7. [Google Scholar]
- 14.Yildirim C, Rodop O, Kuşkucu M, Sahin O, Gamsizkan M. Giant solitary osteochondroma arising from the fifth metatarsal bone: A case report. J Foot Ankle Surg 2010;49:298.e9-15. [Google Scholar]
- 15.Shtofmakher G, Kaufman MA, Bhoola PH, Patel AA, Rice SM, Cohen RE. Multiple osteocartilaginous exostoses of the lower extremity: A case report. Foot (Edinb) 2015;25:62-5. [Google Scholar]





