
Fixator-assisted nailing (FAN) is an innovative technique that is useful in conditioning of the skin, reducing the fracture and preventing rotational displacement of the intercalary segment, which can be used for closed segmental tibial shaft fractures with extensive soft tissue injury.
Dr. Vivek M Sodhai,
Department of Trauma, Sancheti Institute for Orthopaedics and Rehabilitation, Pune, Maharashtra, India. E-mail: vivek.sodhai89@gmail.com
Abstract
Introduction: Segmental tibia fractures with extensive soft tissue injuries are rare and surgical intervention is challenging with no definitive treatment strategies.
Case Report: A 52-year-old man presented with closed right segmental tibia and fibula fracture with extensive blistering of skin caused due to road traffic accident. Distal pulses were palpable and there were no signs of compartment syndrome and other systemic injuries. In the presence of extensive blistering, a monoplanar external fixator was applied within 24 h of injury. 3 weeks later, skin condition was conducive for internal fixation, and closed intramedullary multi-locking nailing was performed using the external fixator for reduction. Fracture healed at 15 months and patient had an excellent functional outcome with full knee range of motion at 2-years follow-up without any complications.
Conclusion: Fixator-assisted nailing is a simple, minimally invasive, and easily reproducible technique that is useful in reducing the fracture and preventing axial rotation of the intercalary segment minimizing the damage to the periosteal blood supply. Our case also highlights the importance of temporary external fixator in soft tissue healing and making the skin conducive for internal fixation.
Keywords: Devascularization, fixator-assisted nailing, intercalary segment, rotational displacement, segmental tibial fracture.
Segmental fracture is defined by two fractures lines resulting in one or multiple intermediate fragments of diaphyseal bone [1]. These injuries are rare with an incidence of approximately 3–12% and result from tremendous impact injuries [2]. Common associated injuries include extensive soft tissue components leading to a higher rate of complications such as infection, non-union, and compartment syndrome [1,3]. These complications arise due to severe soft tissue injury and periosteal stripping of the intercalary diaphyseal segment leading to the devascularization of that segment [4,5].
Surgical treatment of these fractures is difficult and one has several options such as intramedullary nailing (IMN), open reduction internal fixation, and definitive external fixation. However, there is no definitive treatment strategy [4]. The treatment method favors a minimally invasive technique of internal fixation thereby reducing further soft tissue injury and devascularization of fracture fragments [6]. A review conducted by McMohan et al. reported faster healing with IMN [5]. IMN is a biomechanically more stable and closed method of treatment. However, fracture malalignment and rotational displacement of the intercalary segment during reaming is a significant problem with IMN leading to devascularisation, infection, nonunion, and malunion [7]. External fixation has its advantages of being minimally invasive which can be used in poor skin conditions. However, it has the challenges of poor patient compliance and recurrent pin tract infections [8].
We report the combined benefits of two treatment methods using the “fixator-assisted nailing” (FAN) technique for surgical fixation of segmental tibial shaft fractures. A temporizing external fixator helps improve skin condition and can also be used as a reduction aid in definitive fixation of segmental tibia fractures. The patient was informed that the case would be published and written informed consent was taken.
A 52-year-old retired businessman was struck on his two-wheeler by a heavy vehicle and injured his right leg. He presented to our casualty 12 h later after receiving initial treatment and slab immobilization at a peripheral hospital. After a thorough clinical and radiological examination, the patient was diagnosed to have an AO 42C3 closed segmental tibia-fibula fracture of the right leg (Fig. 1) with extensive blistering of the skin. He was hemodynamically stable, distal pulses were palpable, sustained no other neurovascular or systemic injuries, and had no signs of compartment syndrome. The family gave us the prior history of hospital admission for hepatic encephalopathy which was successfully treated and currently had no symptoms, signs related to this comorbidity, or abnormal liver function tests. A thorough preoperative laboratory work-up was normal.

Because of extensive soft tissue injury associated with segmental tibia-fibula fracture, the family was counseled about the difficulties in the treatment and anticipated complications related to this injury. The decision of an initial temporizing external fixator was taken to improve the skin condition before definitive internal fixation. The fixator was applied using the principles of length, axis, and rotation. Due to extensive soft tissue stripping, it is difficult to achieve accurate reduction without opening at the fracture site. Fixator was applied in a manner that can be used as a reduction tool during definitive internal fixation (Fig. 2 and 3). At 3 weeks, the skin condition improved and was conducive for internal fixation (Fig. 4).
In supine position and under spinal anesthesia, the tourniquet was applied and the limb was prepared and draped. After inflating the tourniquet, the external fixator and Schanz pin holding the proximal and intercalary segment was retained and the remaining fixator was removed. A 3-mm K-wire was inserted across the posterior aspect of the proximal fragment which will act as a poller screw and allows the guide-wire to pass in the anterior quadrant and prevent fracture malalignment. In a semi-extended position, a longitudinal incision was taken for the transpatellar tendon approach. Using the fixator, the reduction was maintained and the guide-wire was passed anterior to the poller wire (Fig. 5).
Fig. 6 shows the diagrammatic representation of the FAN technique. Before reaming, the fixator was loosened and Schanz pins were made unicortical to prevent damage to the reaming equipment and fixator was re-tightened. An assistant was asked to firmly hold the fixator during reaming. Multi-locking IMN was used for fixation. Once the nail was negotiated through the proximal and intercalary diaphyseal segment, the fixator was removed and the nail was passed into the distal fragment. Distal and proximal locking was done routinely. Poller wire was then removed. Satisfactory reduction and fixation were confirmed under the c-arm and shown in the postoperative radiograph (Fig. 7).
In the post-operative period, the patient was started on active knee exercises and non-weight bearing walking was started on post-operative day 1. The patient was discharged after 1 week and sutures were removed at 2 weeks. The patient was followed up regularly at monthly intervals. After the radiological appearance of callus formation at 2 months, weight-bearing walking was allowed. The fracture healed successfully at 15 months. At a 2-years follow-up, the patient achieved full knee range of motion (Fig. 8) with a lower extremity functional scale of 88.75% and the radiograph showed healed tibial fractures with consolidation (Fig. 9).
In the past, various authors have reported the modification of standard reduction and fixation techniques for complex fractures of the tibia to overcome the intraoperative difficulties and still be able to follow the principles of minimal soft tissue damage and preserve blood supply to the bone by minimizing periosteal stripping. These modifications include a variety of options such as combining external and internal locking plates [9], clothesline technique during IMN [8], using Farabeuf clamp during undreamed nailing [10], application of large pointed reduction forceps [11], a temporary application of unicortical plates to prevent malalignment [12] and most recently FAN for difficult tibial fractures [13].
The use of internal plates can cause unnecessary extensive periosteal stripping resulting in further reduced blood supply to the diaphyseal bone. Pointed reduction forceps provide limited hold of the cortex and its difficult to control reduction and hence may be ineffective in preventing malalignment. Even though farabeuf clamp is an excellent tool to prevent distraction and rotation of the intercalary segment, there is some amount of periosteal stripping to open the fracture site. Clothesline technique utilizes two monolateral external fixators for preventing malalignment. However, it is useful in cases with proximal tibial shaft fractures. Suprapratellar nailing in the semi-extended position of the knee is also described for these fractures [14]. However, it requires special equipment to prevent cartilage injuries and thereby increases the cost of the procedure. Recently, Semenistyy et al. describe the FAN technique in detail. They utilized a biplanar external fixator for the reduction and fixation of complex tibial fractures. However, the procedure is technically demanding. Further, there is no hold in the intercalary segment to prevent its spinning while reaming.
The described technique is simple, minimally invasive, and unique in certain aspects. Firstly, it utilizes the same temporizing external fixator (used for soft tissue healing and improving skin condition) in the intraoperative period. The fixator applied perpendicular to the coronal plane of the tibia and the semi-extended position of the knee counters the deforming forces of IMN that cause fracture malalignment during fixation. Second, the fixator holds the intercalary segment preventing the axial rotational, thereby minimizing injury to the remaining periosteal blood supply. To the best of our knowledge, although Semenistyy et al. [13] reported FAN in the acute phase, there is no described technique in the literature to address these two keys steps together. However, no technique is without its risks. Pin tract infection is a minor risk that can be successfully avoided by regular antiseptic pin tract dressings and antibiotics.
FAN is a simple, minimally invasive, and easily reproducible technique that is useful in reducing the fracture and preventing axial rotation of the intercalary segment minimizing the damage to the periosteal blood supply. FAN is a viable treatment option for closed segmental tibial shaft fractures with extensive soft tissue injury. However, further studies are required to establish the effectiveness of this technique.
“FAN” is a simple, minimally invasive and easily reproducible technique that can be used in a staged manner for closed segmental tibial shaft fractures with extensive soft tissue injury. Initially, external fixator helps in conditioning the skin and soft tissue healing. During definitive internal fixation with intramedullary nail, the same external fixator helps in reducing the fracture and preventing axial rotation of the intercalary segment minimizing the damage to the periosteal blood supply.
References
- 1.Woll TS, Duwelius PJ. The segmental tibial fracture. Clin Orthop Relat Res 1992;20:4-7. [Google Scholar | PubMed]
- 2.Teraa M, Blokhuis TJ, Tang L, Leenen LP. Segmental tibial fractures: An infrequent but demanding injury. Clin Orthop Relat Res 2013;471:2790-6. [Google Scholar | PubMed]
- 3.Rommens PM, Coosemans W, Broos PL. The difficult healing of segmental fractures of the tibial shaft. Arch Orthop Trauma Surg 1989;108:238-42. [Google Scholar | PubMed]
- 4.Foster PA, Barton SB, Jones SC, Morrison RJ, Britten S. The treatment of complex tibial shaft fractures by the Ilizarov method. J Bone Joint Surg Br 2012;94:1678-83. [Google Scholar | PubMed]
- 5.McMohan SE, Little ZE, Smith TO, Trompeter A, Hing C. The management of segmental tibial shaft fractures: A systematic review. Injury 2016;47:568-73. [Google Scholar | PubMed]
- 6.Farouk O, Krettek C, Miclau T, Schandelmaier P, Guy P, Tscherne H. Minimally invasive plate osteosynthesis and vascularity. Injury 1997;28 Suppl 1:SA7-12. [Google Scholar | PubMed]
- 7.Arastu MH, Sheehan B, Paolucci EO, Buckley RE. Does it really spin? Intra-medullary nailing of segmental tibial fractures a cadaveric study. Injury 2015;46:643-8. [Google Scholar | PubMed]
- 8.Belangero WD, Pires RE, Livani B, Rossi FL, de Andrade AL. “Clothesline technique” for proximal tibial shaft fracture fixation using conventional intramedullary nail: A simple, useful, and inexpensive technique to prevent fracture malalignment. Eur J Orthop Surg Traumat 2017;28:721-5. [Google Scholar | PubMed]
- 9.Ma CH, Tu YK, Yeh JH, Yang SC, Wu CH. Using external and internal locking plates in a two-stage protocol for treatment of segmental tibial fractures. J Trauma 2011;71:614-9. [Google Scholar | PubMed]
- 10.Robertson A, Giannoudis PV, Matthews SJ. Maintaining reduction during unreamed nailing of a segmental tibial fracture: The use of a Farabeuf clamp. Injury 2003;34:389-91. [Google Scholar | PubMed]
- 11.Ruedi TP, Murphy WM, editors. AO Principles of Fracture Management. New York: Thieme; 2000. [Google Scholar | PubMed]
- 12.Matthews DE, McGuire R, Freeland AE. Anterior unicortical buttress plating in conjunction with an undreamed interlocking intramedullary nail for treatment of very proximal tibial diaphyseal fractures. Orthopaedics 1997;20:647-8. [Google Scholar | PubMed]
- 13.Semenistyy AA, Litvina EA, Fedotova AG, Gwam C, Mironov AN. Fixator-assisted nailing of tibial fractures: New surgical technique and presentation of first 30 cases. Injury 2019;50:515-20. [Google Scholar | PubMed]
- 14.Sanders RW, DiPasquale TG, Jordan CJ, Arrington JA, Sagi HC. Semiextended intramedullary nailing of the tibia using a suprapatellar approach: Radiographic results and clinical outcomes at a minimum of 12 months follow-up. J Orthop Trauma 2014;28:245-55. [Google Scholar | PubMed]




“Fixator-assisted Nailing” Technique for Closed Segmental Tibia Shaft Fracture with Extensive Soft Tissue Injury – A Case Report
Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2012 JOCR Oct-Dec 2012 – Reviewer’s Ackowledgement
October 10, 2012 JOCR Oct-Dec 2012 – Reviewer’s Ackowledgement June 1, 2025 Irreparable Isolated Infraspinatus Musculotendinous Lesion Treated With Lower Trapezius Tendon Transfer: Case Report
June 1, 2025 Irreparable Isolated Infraspinatus Musculotendinous Lesion Treated With Lower Trapezius Tendon Transfer: Case Report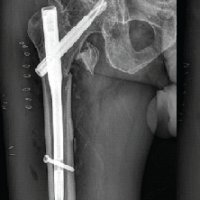 September 1, 2025 A Rare Case of Pseudoaneurysm of Profunda Femoris Artery Following Surgical Fixation of an Intertrochanteric Fracture
September 1, 2025 A Rare Case of Pseudoaneurysm of Profunda Femoris Artery Following Surgical Fixation of an Intertrochanteric Fracture July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus
July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus