
The coexistence of a Quadratus Femoris hematoma and/or edema with Ischio-Femoral impingement in adolescents, may temper with the initial MRI measurements and render the diagnosis of the latter rather difficult.
Dr. Kyriakos A. Papavasiliou,
Department Orthopaedics, Aristotle University of Thessaloniki Medical School,
Papageorgiou General Hospital of Thessaloniki, Thessaloniki, Greece.
E-mail: papavasiliou.kyriakos@gmail.com
Abstract
Introduction: Hip pain in children and adolescents may become a diagnostic challenge. A wide range of causes must be considered in the deferential diagnosis. Ischiofemoral impingement (IFI) is a pathological condition defined by hip pain associated with narrowing of the ischiofemoral (IF) space. We report the case of an adolescent patient with non-traumatic quadratus femoris (QF) tear secondary to an occult IFI syndrome. To the best of our knowledge, this is the first such case reported in the literature.
Case Report: A 15-year-old girl reported persisting hip pain for a month following increased physical activity. The symptoms had started a couple of days following a weekend of increased activity due to her participating in a dancing contest. Physical examination and imaging studies (standard anterior pelvis radiograph and MRI-scan) failed to reveal any pathology apart from an area of diffused edema in the IF space. Standard hematology and biochemistry laboratory tests were all within normal range. Conservative treatment for 6 months with rest and modification of physical activities failed. A new MRI scan showed partial edema resolution and marked reduction in the IF and QF spaces (12 mm and 8 mm, respectively), thus suggesting IFI, which, in turn, led to a partial rupture of the QF. The patient underwent a local infiltration of the QF with betamethasone sodium phosphate and betamethasone acetate (6+6 mg/2 ml) under CT guidance, which led to the complete resolution of all her symptoms. She remains symptoms free for 24 months.
Conclusion: IFI is a rather uncommon condition in the developing skeleton. As in adults, in adolescents as well, MRI is the study of choice in cases of IFI, since it shows QF pathology and allows measurement of the IF and QF spaces, assisting physicians in establishing the right diagnosis. However, the coexistence of a QF hematoma and/or edema, may temper with the initial MRI measurements and render the diagnosis of the primary condition rather difficult. Conservative treatment (with local infiltration of the QF) was proven to be successful in the hereby described case.
Keywords: Ischiofemoral impingement, quadratus femoris tear, MRI, adolescent hip.
Pain in the adolescent hip poses a diagnostic challenge for the physician [1]. A wide range of causes must be considered in the differential diagnosis [2]. Quadratus femoris (QF) is an external rotator of the hip. Originating from the lateral aspect of the obturator ring above the ischial tuberosity, it inserts at the quadrate tubercle and the adjacent intertrochanteric crest. Although it is rather uncommon, QF pathology is a well-recognized cause of hip pain [3].
Ischiofemoral impingement (IFI) is a pathological condition defined by hip pain associated with narrowing of the ischiofemoral (IF) space. Initially described as a cause of post-operative hip pain following total hip arthroplasty and proximal femoral osteotomy [4], it is characterized by an impingement between the lesser trochanter on the femoral side and the ischial tuberosity on the pelvic side. This results in the injury of the underlying QF muscle [2]. It is difficult to diagnose patients with this pathology, especially when there is no history of a recent operation and/or other causes (i.e., trauma and tumors) leading to the impingement [5]. Nonetheless, in about 46% of cases, an underlying cause may be responsible for the so-called secondary IFI [6]. The majority of published cases report IFI in the adult population, with only a few cases reported in the literature regarding children and adolescents [6,7,8].
We report the case of a 15-year-old female patient with non-traumatic QF partial tear, secondary to an occult IFI syndrome. To the best of our knowledge, this is the first such case reported in pediatric population
An otherwise fit-and-well 15-year-old female patient complaining of persistent pain in her left hip for a month was referred to our outpatient clinic by her family’s physician. The patient (a recreational folk dancer) reported that her symptoms started a couple of days following a weekend of increased physical activity due to her participating in a dancing festival. She could not recall any recent injury and she was able to uneventfully complete her participation in the festival.
The patient was capable of full, nonetheless painful, passive range of motion at her hip with no mechanical or audible click. Active hip movements were more painful and restricted. The pain area could be easily pinpointed by the patient at her left gluteal area, just behind the greater trochanter. Pain was aggravated with passive internal and external rotation with the hip in flexion, extension, and hyperextension. Routine blood tests, including inflammatory markers, came back negative. A plain radiograph showed normal anatomy with a slightly increased neck-shaft angle (Fig. 1).
The initial therapeutic approach was based on rest and analgesia with paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs). Since there was no improvement after a week, the patient underwent an MRI scan. An area of diffused edema and hematoma in the IF space suggested a partial rupture of the QF muscle. However, both the IF (20.3 mm) and the QF (20.3 mm) spaces were within the expected for the patient normal range. On the contrary, the contralateral right hip’s IF space (17.3 mm) was narrower than expected (Fig. 2).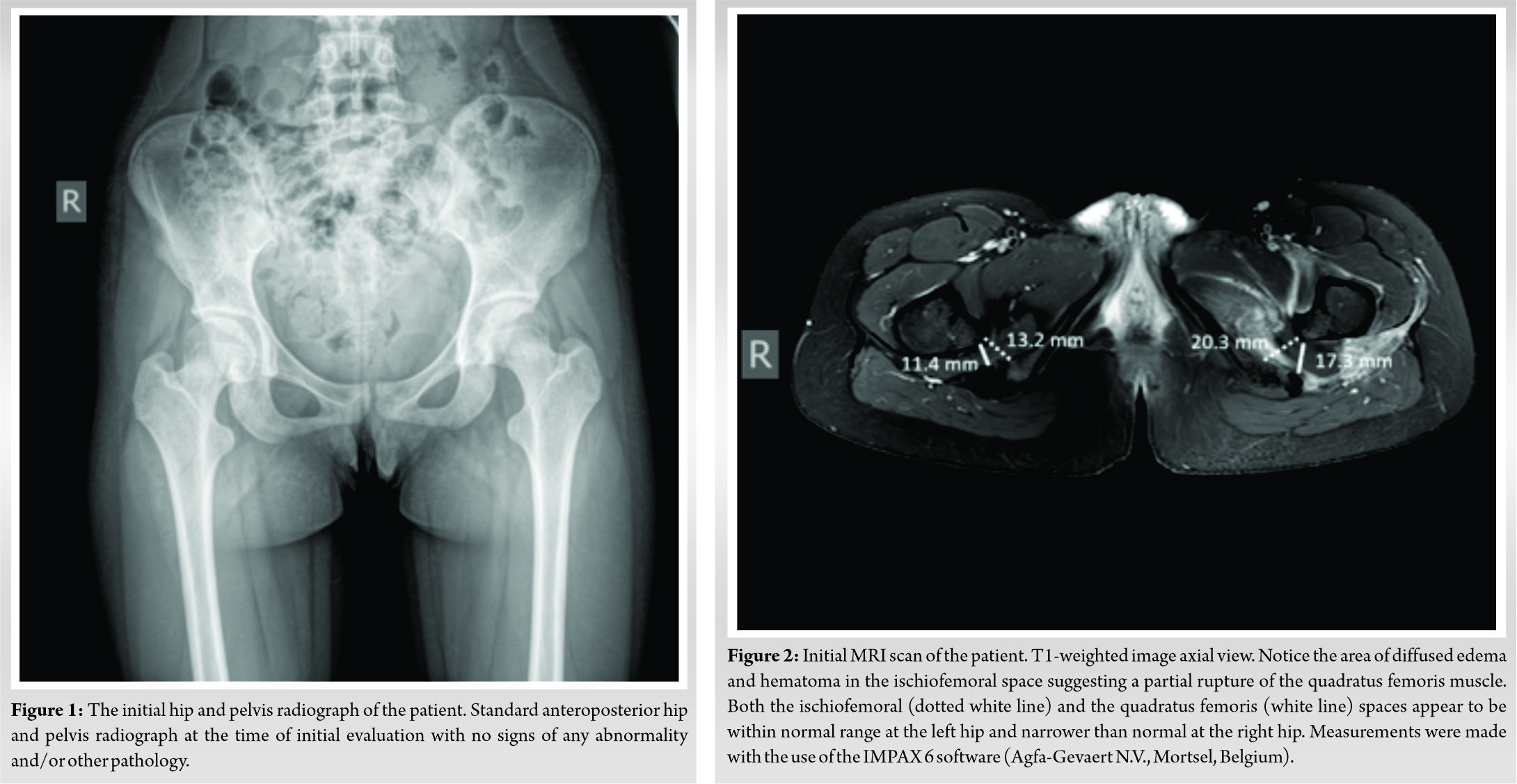 Despite the continuous use of analgesics and the avoidance of physical activities by the patient for a period of 1 month, the symptoms persisted. Physiotherapy was prescribed next, but also failed to relieve the patient from her symptoms. The patient was instructed to remain bedridden for a period of 15 days, but this measure was also proven unsuccessful. She was then told to avoid weight-bearing for another 15 days, but there was still no improvement. The patient underwent a new MRI scan 1 month following her initial evaluation, which showed a slight resolution of the QF edema in the IF space and a significant reduction of the QF space (Fig. 3).
Despite the continuous use of analgesics and the avoidance of physical activities by the patient for a period of 1 month, the symptoms persisted. Physiotherapy was prescribed next, but also failed to relieve the patient from her symptoms. The patient was instructed to remain bedridden for a period of 15 days, but this measure was also proven unsuccessful. She was then told to avoid weight-bearing for another 15 days, but there was still no improvement. The patient underwent a new MRI scan 1 month following her initial evaluation, which showed a slight resolution of the QF edema in the IF space and a significant reduction of the QF space (Fig. 3). 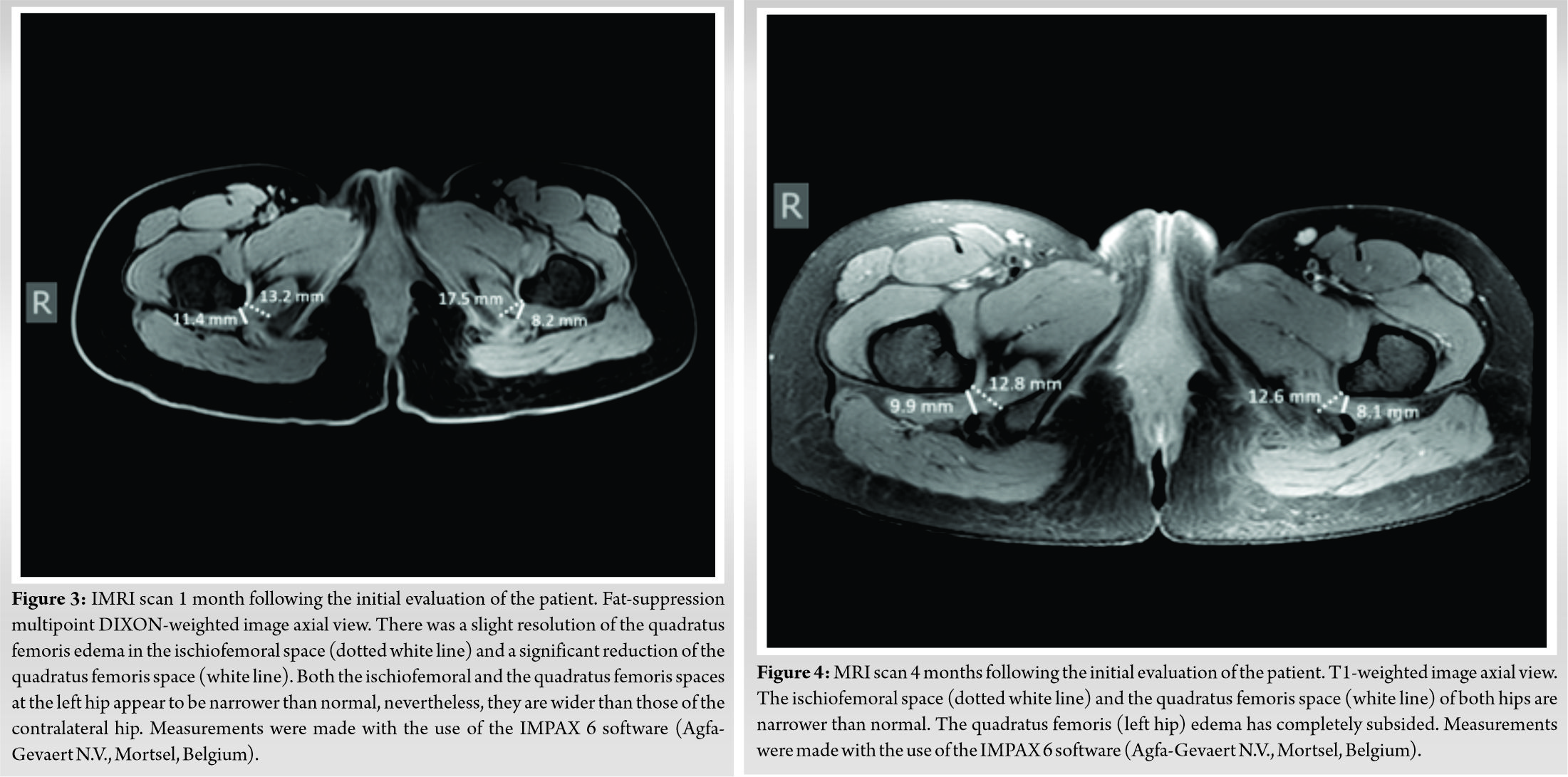
The patient was referred to a consultant rheumatologist and a consultant psychiatrist for evaluation. All laboratory tests failed to reveal any pathology and her psychiatric evaluation was also non-consistent with any disorder. She underwent a new MRI scan 3 months later (Fig. 4), which showed a partial resolution of the edema and revealed a marked reduction in the IF and the QF spaces (12.6 mm and 8.1 mm, respectively), suggesting thus the underlying IFI syndrome [6,7], which apparently had led to a partial rupture of the QF muscle (probably during the weekend of increased physical activities) and the subsequent development of a refractory tendonitis. Physical examination at this stage revealed positive IFI test and long-stride walking (LSW) test [8]. 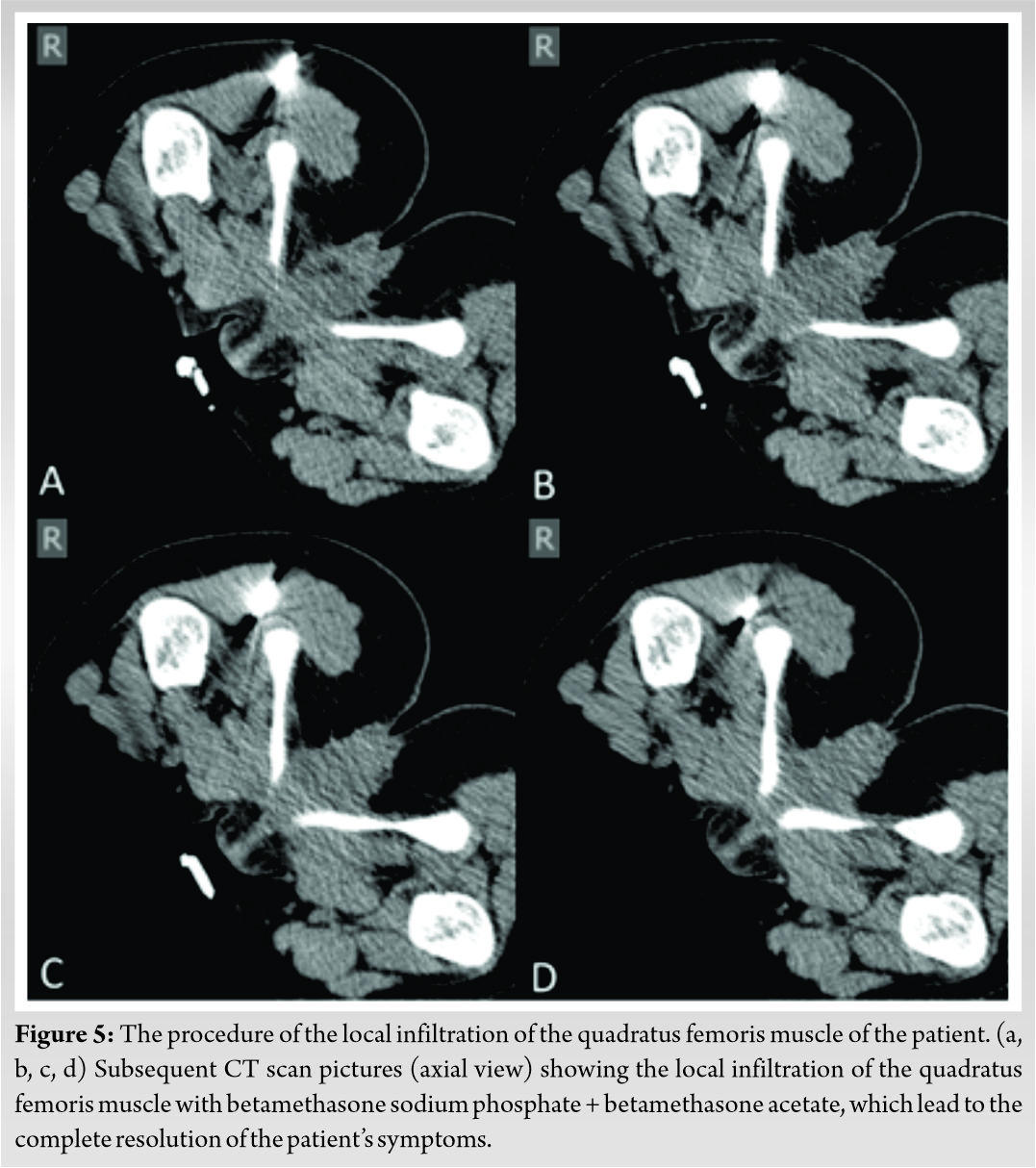 Although the IF and QF spaces were also narrow in the contralateral hip in all MRI scans (Fig. 2, 3, 4), the patient never complained about any symptoms and her physical examination was always negative for IFI.
Although the IF and QF spaces were also narrow in the contralateral hip in all MRI scans (Fig. 2, 3, 4), the patient never complained about any symptoms and her physical examination was always negative for IFI.
The patient underwent a local infiltration of the QF with betamethasone sodium phosphate + betamethasone acetate (6+6 mg/2 ml) under CT guidance (Fig. 5), which led to the complete resolution of all her symptoms within a few days. She remains symptoms free at her latest follow-up visit 24 months following the infiltration. She has fully returned to her previous activities and she is able to perform everyday life and sports activities without experiencing any pain and/or discomfort.
The diagnosis of the IFI is based on the patient’s history and physical examination and is usually confirmed by an MRI scan [9,10]. The clinical assessment of patients with IFI is not always easy, since they usually complain about a chronic vague pain in the groin or buttock area [11]. Clinical manifestation of IFI may also include sciatica or a snapping sensation associated with the hip joint motions. In most cases, the duration of these symptoms is long and it may vary between months and years [9]. The only reported specific physical examination tests of this syndrome are the IFI and the LSW tests [12].
MRI is the study of choice, as it reveals QF pathology and allows measurement of both the IF and QF spaces [13]. Goldberg-Stein et al. [8] reported significantly narrower IF and QF spaces both in children and adolescents, with a threshold value of 14.9 mm and 11.2 mm for IF and QF spaces, respectively, for children (7–12 years old) and 19 mm and 11 mm for adolescents (13–18 years old).
Although narrowing of the IF and QF spaces accompanied with QF edema is sensitive radiographic markers for the IFI syndrome [10], its exact pathophysiology remains disputed [14]. Papavasiliou et al. [15] reported reduced IF and QF spaces in non-symptomatic young athletes and Stenhouse et al. [7] found bilateral QF edema in young patients with unilateral symptomatology, as we did in our case (Fig. 5). More recently, other measurements such as the femoral mean neck anteversion and the mean angle between the femoral neck version and the lesser trochanter version have also been proposed [16].
The treatment of refractory cases of IFI is a relatively difficult task [17]. Conservative treatment with rest, NSAIDs, avoidance of activities which may provoke impingement, and physiotherapy, aiming on stretching and strengthening of the external rotators of the hip, seems to be the golden standard. Refractory cases may be dealt with a very few and complex surgical solutions. In such cases, extra-articular arthroscopy and debridement or even proximal derotational femoral osteotomies have been proposed [18]. Additional CT or US-guided injections or local anti-inflammatories (corticosteroids), analgesics, and more recently botulinum toxin may be used [6,19,20].
We report the case of a 15-year-old girl with non-traumatic QF partial tear presented as an overuse syndrome secondary to an occult IFI. To the best of our knowledge, this is the first such case reported in the pediatric population. IFI in children and adolescents is rare and can be a cause of significant, but ill-defined hip pain. Clinical diagnosis is not usually easy, as patient’s history and physical examination are imprecise and difficult to interpret.
In cases where IFI is combined with a QF tear, initial MRI measurements of the IF and QF spaces may be misleading, since they may appear normal or even larger than usual, thus hiding an existing IFI syndrome.
IFI in children and adolescents is rare and can be a cause of significant, but ill-defined hip pain. Clinical diagnosis is not usually easy, as patient’s history and physical examination are imprecise and difficult to interpret. The coexistence of a QF hematoma and/or edema with IFI may temper with the initial MRI measurements and render the diagnosis of the primary condition rather difficult.
References
- 1.López-Sánchez MC, Armesto Pérez V, Furelos LÁ, Vázquez-Rodríguez TR, Arrojo GC, Román TM. Ischiofemoral impingement: Hip pain of infrequent cause. Reumatol Clin 2013;9:186-7. [Google Scholar | PubMed]
- 2.Spahn G, Schiele R, Langlotz A, Jung R. Hip pain in adolescents: Results of a cross-sectional study in German pupils and a review of the literature. Acta Paediatr 2005;94:568-73 [Google Scholar | PubMed]
- 3.Zibis AH, Fyllos AH, Karantanas AH, Raoulis V, Karachalios TS, Arvanitis DL. Quadratus femoris tear as an unusual cause of hip pain: A case report. Hip Int 2016;26:e7-9. [Google Scholar | PubMed]
- 4.Johnson KA. Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases. J Bone Joint Surg Am 1977;59:268-9. [Google Scholar | PubMed]
- 5.Gollwitzer H, Banke IJ, Schauwecker J, Gerdesmeyer L, Suren C. How to address ischiofemoral impingement? Treatment algorithm and review of the literature. J Hip Preserv Surg 2017;4:289-98. [Google Scholar | PubMed]
- 6.Vassalou EE, Klontzas ME, Mercouris P, Bintoudi A, Natsika M, Karantanas A. Quadratus femoris muscle: Spectrum of MR imaging findings in 51 patients presenting with painful hip. Hell J Radiol 2018;3:1-11. [Google Scholar | PubMed]
- 7.Stenhouse G, Kaiser S, Kelley SP, Stimec J. Ischiofemoral impingement in children: Imaging with clinical correlation. AJR Am J Roentgenol 2016;206:426-30. [Google Scholar | PubMed]
- 8.Goldberg-Stein S, Friedman A, Gao Q, Choi J, Schulz J, Fornari E, et al. Narrowing of ischiofemoral and quadratus femoris spaces in pediatric ischiofemoral impingement. Skeletal Radiol 2018;47:1505-10. [Google Scholar | PubMed]
- 9.Torriani M, Souto SC, Thomas BJ, Ouellette H, Bredella MA. Ischiofemoral impingement syndrome: An entity with hip pain and abnormalities of the quadratus femoris muscle. AJR Am J Roentgenol 2009;193:186-90. [Google Scholar | PubMed]
- 10.Singer AD, Subhawong TK, Jose J, Tresley J, Clifford PD. Ischiofemoral impingement syndrome: A meta-analysis. Skeletal Radiol 2015;44:831-7. [Google Scholar | PubMed]
- 11.Hayat Z, Konan S, Pollock R. Ischiofemoral impingement resulting from a chronic avulsion injury of the hamstrings. BMJ Case Rep. 2014 Jun 25;2014:bcr2014204017. [Google Scholar | PubMed]
- 12.Gómez-Hoyos J, Martin RL, Schröder R, Palmer IJ, Martin HD. Accuracy of 2 clinical tests for ischiofemoral impingement in patients with posterior hip pain and endoscopically confirmed diagnosis. Arthroscopy 2016;32:1279-84. [Google Scholar | PubMed]
- 13.Bredella MA, Azevedo DC, Oliveira AL, Simeone FJ, Chang CY, Stubbs AJ, et al. Pelvic morphology in ischiofemoral impingement. Skeletal Radiol 2015;44:249-53. [Google Scholar | PubMed]
- 14.Vassalou EE, Zibis AH, Klontzas ME, Karantanas AH. Imaging of impingement syndromes around the hip joint. Hip Int 2017;27:317-28. [Google Scholar | PubMed]
- 15.Papavasiliou A, Siatras T, Bintoudi A, Milosis D, Lallas V, Sykaras E, et al. The gymnasts’ hip and groin: A magnetic resonance imaging study in asymptomatic elite athletes. Skeletal Radiol 2014;43:1071-7. [Google Scholar | PubMed]
- 16.Gómez-Hoyos J, Schröder R, Reddy M, Palmer IJ, Martin HD. Femoral neck anteversion and lesser trochanteric retroversion in patients with ischiofemoral impingement: A case-control magnetic resonance imaging study. Arthroscopy 2016;32:13-8. [Google Scholar | PubMed]
- 17.Nakano N, Shoman H, Khanduja V. Treatment strategies for ischiofemoral impingement: A systematic review. Knee Surg Sports Traumatol Arthrosc 2020;28:2772-87. [Google Scholar | PubMed]
- 18.Hatem MA, Palmer IJ, Martin HD. Diagnosis and 2-year outcomes of endoscopic treatment for ischiofemoral impingement. Arthroscopy 2015;31:239-46. [Google Scholar | PubMed]
- 19.Backer MW, Lee KS, Blankenbaker DG, Kijowski R, Keene JS. Correlation of ultrasound-guided corticosteroid injection of the quadratus femoris with MRI findings of ischiofemoral impingement. AJR Am J Roentgenol 2014;203:589-93. [Google Scholar | PubMed]
- 20.Chen YT, Jenkins KM. Ultrasound finding of ischiofemoral impingement syndrome and novel treatment with botulinum toxin chemodenervation: A case report. PM R 2018;10:665-70. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 June 27, 2021 Hemangioma of First Extensor Compartment of the Wrist– A Rare Case Report
June 27, 2021 Hemangioma of First Extensor Compartment of the Wrist– A Rare Case Report May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures
May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures January 3, 2019 Autologous Osteochondral Transplantation in Full-thickness Patella Chondral Lesion: A Case Series
January 3, 2019 Autologous Osteochondral Transplantation in Full-thickness Patella Chondral Lesion: A Case Series September 8, 2018 A Rare Case of Glomus Tumor of the Thigh with Literature Review
September 8, 2018 A Rare Case of Glomus Tumor of the Thigh with Literature Review