
Patients presenting with painless bilateral foot drop without bowel bladder symptoms should be investigated for spinal cause to arrive at the correct diagnosis and starstart early and valuable treatement t early treatment because lumbar spine degenerative disorders can also present in such manner without radiculopathy. without radiculopathy.
Dr. Nikhil Jain, Institute of Spine Surgery, FNB Spine Surgery, Institute of Spine, Jaypee Multispecialty Hospital, Sector 128, Noida - 210 304, Uttar Prades, India. E-mail: drnikhil.jn@gmail.com
Abstract
Introduction: Acute painless bilateral foot drop without bowel/bladder involvement is a very rare presentation of lumbar degenerative disorders. Only a few cases have been published on it in the literature. An early intervention could prove to be very helpful for the neurological recovery.
Case Report: We present three cases where patients developed acute onset bilateral foot drop without radiculopathy and without bowel/bladder involvement. The first case was due to acute lumbar disc herniation, the second was caused by acute disc prolapse in a pre-existing asymptomatic lumbar canal stenosis, and the third one precipitated in a progressive degenerative severe lumbar spinal stenosis. Two cases (case reports 1 and 3) underwent minimal invasive decompression while the other case (case report 2) underwent instrumentation+ decompression + fusion. Case 1 and 2 with a short duration of symptoms showed good neurological recovery, whereas Case 3 with longer duration of complaints did not improve.
Conclusion: Patients presenting with painless bilateral foot drop without cauda equine syndrome should be evaluated for spinal causes besides central nervous systemCNS, peripheral nerve, metabolic and autoimmune causes. Any finding in support of lumbar degenerative disease as the cause after excluding other causes should prompt for surgical decompression of the spine as an early intervention might help patient recover back to a normal and active lifestyle.
Keywords: Painless, bilateral, foot drop, acute.
Acute disc prolapse or lumbar spinal (LS) stenosis causing painless bilateral foot drop without cauda equina syndrome is extremely rare. To the best of author’s knowledge, only two such cases have been reported till date [1,2]. Cases have been reported about bilateral foot drop without cauda equina syndrome due to lumbar disc prolapse and LS stenosis, but they were associated with lower limbs radiculopathy [3].
Here, we present three cases where patients developed acute onset bilateral foot drop without radiculopathy and without bowel/bladder involvement. The first case was due to acute lumbar disc herniation, the second was caused by acute disc prolapse in a pre-existing asymptomatic lumbar canal stenosis, and the third one precipitated in a progressive degenerative severe LS stenosis.
A 45-year-old male patient with a history of chronic back pain developed acute onset weakness in both the ankle and feet while getting out of bed. The patient had moderately severe back pain for the past 15 days for which the patient was taking self-medications. At the time of presentation, the straight leg raising test was negative for both lower limbs. Muscle strength of ankle dorsiflexion, great toe extension and ankle inversion was 2/5 on the right and 1/5 on the left side. Ankle eversion and plantar flexion was normal and full bilaterally. Sensations were decreased only in L5 dermatomes in both legs. All deep tendon reflexes were normal and plantars were flexor bilaterally. Distal pulses were intact in both lower limbs. Perianal sensation and bowel/bladder control were intact. To rule out acute lumbar disc herniation a Lumbo-Sacral spine Magnetic Resonance Imaging (MRI) was performed, which revealed a large extruded central disc fragment at the L3-L4 level.
Surgical lumbar decompression was advised to the patient and indeterminate prognosis of recovery was explained in detail. The patient underwent microscopic L3-L4 laminectomy and the extruded central disc fragment was removed from the right side. Patient was put on physiotherapy and rehabilitation. One month later patient’s neurology improved to 4/5 bilaterally in both ankles and great toes.

A 65-year-old male suffering from chronic low back pain and bilateral neurogenic claudication presented with acute bilateral lower limb weakness and foot drop without any episode of radiculopathy. On clinical examination, the straight leg raising test was negative for both lower limbs. Muscle power testing revealed bilateral knee extension as 3/5, bilateral ankle dorsiflexion, great toe extension and ankle inversion as 0/5 and bilateral ankle plantar flexion and ankle eversion as 3/5. The sensations were decreased bilaterally in L4, L5 and S1 dermatomes. Ankle reflexes were absent and knee reflexes were sluggish in both the lower limbs. Plantars were mute bilaterally. Distal pulses were intact in both lower limbs. Perianal sensation and bowel/bladder function were intact. MRI L-S spine for the patient was done.
The disease, treatment and indeterminate prognosis were explained to the patient. The patient underwent posterior instrumentation+central decompression+interbody fusion L3-L5 from the right side. After surgery, the patient was put on physiotherapy and rehabilitation. Two months later the patient’s neurology improved to 4/5 bilaterally in both ankle and great toes.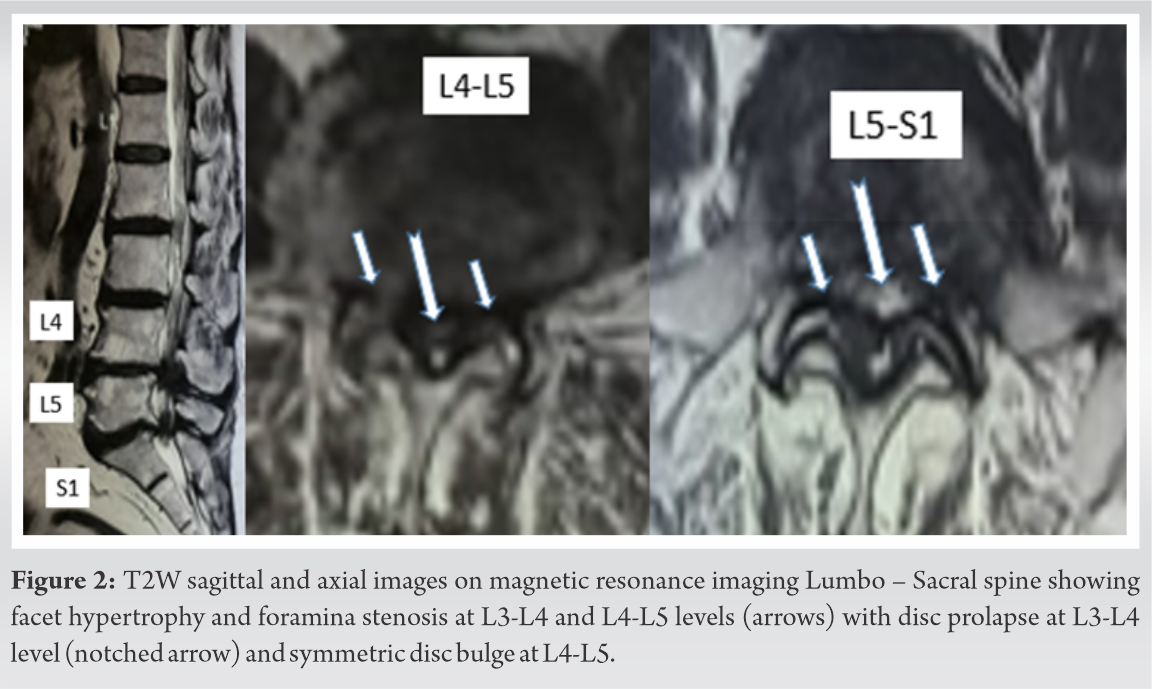
This is a case of a 76-year-old male with chronic bilateral gluteal pain and bilateral lower limb neurogenic claudication. The patient was a diabetic, well-controlled on medications. The patient developed insidious onset progressive subacute foot drop over two months with no history of radiculopathy. At the time of presentation, the straight leg raising test was negative for both lower limbs. On clinical examination muscle power testing revealed bilateral knee extension as 4/5, right ankle dorsiflexion, great toe extension and ankle inversion as 0/5 and left ankle dorsiflexion as 2/5 and great toe extension and ankle inversion as 0/5. Bilateral ankle plantar flexion and ankle eversion were 3/5. The sensations were decreased bilaterally in L4, L5, and S1 dermatomes. Ankle reflexes were absent and knee reflexes were sluggish in both the lower limbs. Plantars were mute bilaterally. Distal pulses were intact. Perianal sensation was intact with normal bladder and bowel function. L-S-MRI revealed severe lumbar canal stenosis at L4-L5, L5-S1 with ligamentum flavum hypertrophy.
The disease, treatment and indeterminate prognosis were explained to the patient. The patient underwent microscopic unilateral laminotomy and bilateral decompression L4-L5, L5-S1 from the right side. After surgery, the patient was put on physiotherapy and rehabilitation. One month later the patient’s neurology remained the same.
Bilateral foot drop can be seen in cauda equina/conus medullaris syndrome, thoracic spinal cord compression, central nervous system (CNS) pathology, peripheral neuropathy and metabolic/autoimmune diseases [4,5]. Less than 10% of cases with lumbar degenerative disc diseases develop foot drop [6]. Bilateral foot drop without cauda equina syndrome is very rare and very few cases have been reported in the literature so far. Aono et al. who has published extensive work on foot drop due to lumbar degenerative disorders, had only one patient suffering from acute painless bilateral foot drop without cauda equine syndrome out of their total 66 cases in their two studies [2,7]. A recent case study by Robles published about a patient who with history of painless foot drop in one limb, developed painless foot drop in the opposite lower limb secondary to lumbar canal stenosis at L3-L4 and L4-L5. The patient underwent surgery and showed recovery [1].
Excellent= when muscular strength improved to a manual muscle test score of 4 or 5, Good= for a score of 3, fair= when muscular strength improved but it remained <3, Poor=no improvement.
In our study, we have reported three cases of synchronous painless bilateral foot drop without radiculopathy and without cauda equina syndrome secondary to lumbar degenerative disorders. Two cases (case reports 1 and 3) underwent minimal invasive decompression while the other case (case report 2) underwent instrumentation + decompression + fusion. In our series cases with short duration of symptoms showed good neurological recovery (cases 1 and 2) while case with longer duration of complaints (case 3) did not improve. The patients in cases 1 and 2 were also younger compared to case 3 who did not improve neurologically. Both these points are in agreement to the study published by Aono et al., though motor grading of ankle dorsi-flexors which was another key feature predicting the recovery in such patients ranged between 0 and 2 in our recovered cases and stood in contrast to their outcomes [8]. Aono et al. in both their studies found no difference in outcomes of patients having foot drop secondary to disc herniation versus spinal stenosis but in our series the patient who did not recover suffered from severe spinal stenosis, though it should not be missed that the patient had longer duration of symptoms and was also a diabetic. Both these factors can adversely affect the nerve recovery [2,8].
Usually, a patient with LS stenosis or lumbar disc prolapse gives a history of low back pain and limb radiculopathy when nerve roots get compressed. Looking at the anatomy of cauda equina, the exiting nerve roots enter their respective foramen antecedent to the disc whereas the traversing nerve roots lie ventrolaterally and rest of the roots float dorso-medially when crossing the disc. The sensory fibres are more sensitive to compression in comparison to motor fibers explaining the sensory symptoms preceding any motor weakness when roots get compressed [9]. Even though the thecal sac was almost obliterated in all our cases, the mechanism of developing bilateral foot drop without having pain and sparing of bowel and bladder control is not clearly understood.
Through this study, we learn that lumbar degenerative disorders can present as acute neurological deficits even without radicular symptoms. Henceforth, we feel it is prudent to investigate the patient using X-ray and MRI of the lumbar spine before moving on to rule out other systemic/autoimmune causes.
Patients presenting with painless bilateral foot drop without cauda equine syndrome should be evaluated for spinal causes besides CNS, peripheral nerve, metabolic and autoimmune causes. Any finding in support of lumbar degenerative disease as the cause after excluding other causes should prompt for surgical decompression of the spine as an early intervention might help patient recover back to a normal and active lifestyle.
Patients presenting with painless bilateral foot drop without cauda equine syndrome should be evaluated for spinal causes besides CNS, peripheral nerve, metabolic, and autoimmune causes.
References
- 1.Robles LA. Metachronous bilateral painless foot drop secondary to spinal stenosis: Case report. Cureus 2018;10:e2276 [Google Scholar | PubMed]
- 2.Aono H, Nagamoto Y, Tobimatsu H, Takenaka S, Iwasaki M. Surgical outcomes for painless drop foot due to degenerative lumbar disorders. J Spinal Disord Tech 2014;27:258-61. [Google Scholar | PubMed]
- 3.Ramnaryan R, Palinikumar C. Bilateral foot drop without cauda equina syndrome due to L4-L5 disc prolapse: A case report. Internet J Neurosurg 2007;5:6. [Google Scholar | PubMed]
- 4.Westhout FD, Paré LS, Linskey ME. Central causes of foot drop: Rare and underappreciated differential diagnoses. J Spinal Cord Med 2007;30:62-6. [Google Scholar | PubMed]
- 5.Adams RD, Asbury AK. Diseases of the peripheral nervous system. In: Harrison’s Principles of Internal Medicine. New York: McGraw-Hill; 1980. p. 2027-39. [Google Scholar | PubMed]
- 6.Liu K, Zhu W, Shi J, Jia L, Shi G, Wang Y, et al. Foot drop caused by lumbar degenerative disease: Clinical features, prognostic factors of surgical outcome and clinical stage. PLoS One 2013;8:e80375. [Google Scholar | PubMed]
- 7.Aono H, Iwasaki M, Ohwada T, Okuda S, Hosono N, Fuji T, Yoshikawa H: Surgical outcome of drop foot caused by degenerative lumbar diseases. Spine (Phila Pa 1976) 2007;32:262-6. [Google Scholar | PubMed]
- 8.Iizuka Y, Iizuka H, Tsutsumi S, Nakagawa Y, Nakajima T, Sorimachi Y, et al. Foot drop due to lumbar degenerative conditions: Mechanism and prognostic factors in herniated nucleus pulposus and lumbar spinal stenosis. J Neurosurg Spine 2009;10:260-4. [Google Scholar | PubMed]
- 9.Canale ST, Beaty JH. Campbell’s Operative Orthopaedics E-Book. Amsterdam, Netherlands: Elsevier Health Sciences; 2012. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Anterior Hip Dislocation Following Total Hip Arthroplasty, Caused by Broken Trial Femoral Head Particles: A Case Report
March 1, 2025 Anterior Hip Dislocation Following Total Hip Arthroplasty, Caused by Broken Trial Femoral Head Particles: A Case Report July 10, 2015 Delayed Presentation of Metacarpophalangeal Joint Dislocation of the Thumb in Children Requiring Open Reduction: Two Cases Reported and Review of Literature
July 10, 2015 Delayed Presentation of Metacarpophalangeal Joint Dislocation of the Thumb in Children Requiring Open Reduction: Two Cases Reported and Review of Literature August 10, 2023 Non-metallic Fixation of Patella Fractures: A Paradigm Shift
August 10, 2023 Non-metallic Fixation of Patella Fractures: A Paradigm Shift May 1, 2019 Arthroscopic Repair of an Isolated Infraspinatus Tear in a Contact Athlete: A Case Report
May 1, 2019 Arthroscopic Repair of an Isolated Infraspinatus Tear in a Contact Athlete: A Case Report