
Early diagnosis through meticulous clinical examination and investigations is important in treatment of psoas abscess and reducing associated morbidity and mortality.
Dr. Jishar Sainulabdeen, Department of Orthopaedics, Believers Church Medical College and Hospital, Thiruvalla - 689 103, Kerala, India. E-mail: drjishar.sa@gmail.com
Abstract
Introduction: Iliopsoas abscess is an uncommon condition, often with insidious and nonspecific symptoms. Patients often present with a limp, fever, weight loss, and flank or abdominal pain. An iliopsoas abscess can be either primary or secondary depending on the presence or absence of an underlying disease. Primary abscess is very common in Asia and other developing countries. If untreated, iliopsoas abscess can spread to lower limbs, compress iliac vein, ureter and can end up in sepsis. There have been only a very small number of cases of psoas abscess with associated hip septic arthritis reported so far. Bilateral iliopsoas abscess is also a rare entity.
Case Report: We report here a 58-year-old diabetic lady with fever and both hip pain subsequent to a fall at home one month back around one 1 month before. . She was initially seen elsewhere, and a diagnosis of L4-L5 disc bulge was made following which rest , analgesics and steroids were given. Later, repeat magnetic resonance imageMRI showed bilateral Iliacus abscess and bilateral hip synovitis. She was started on anti anti-tuberculosis medications and referred to us. We investigated for occult sources of infection and did bilateral iliopsoas abscess drainage followed by staged bilateral total hip replacement. She now continues to be symptom free.
Conclusion: Our patient had primary bilateral iliopsoas abscess with bilateral hip Streptococcus faeeacalis septic arthritis. It has not been reported in the literature till now.
Clinical Message: Early diagnosis through meticulous clinical examination and investigations is important in treatment of the abscess and reducing morbidity and mortality.
Keywords: Primary iliopsoas abscess, septic arthritis, bilateral iliopsoas abscess.
Iliopsoas abscess was first described by Mynter in 1881, who referred to it as psoitis [1]. It is classified as primary or secondary, depending on the presence or absence of underlying disease. Primary iliopsoas abscess occurs through hematogenous or lymphatic spread of an infectious process from an occult source in the body [2], and is more common in Asia, Africa, and North America whereas secondary abscess is common in other parts of the world [3]. The psoas muscle is close to multiple organs such as the sigmoid colon, appendix, jejunum, ureters, abdominal aorta, kidneys, pancreas, spine, and iliac lymph nodes. This proximity makes these organs potential sources of infection to the psoas muscle. The abundant blood supply of the muscle is believed to predispose it to hematogenous spread from occult sites of infection. Usually, young males are more affected [1,2,3]. The mortality rate is 2.4% in primary cases and 19% in secondary cases. Ricci et al. opined that the mortality can be 100 % when left untreated. The Iliopsoas bursa between the psoas muscle-tendon insertion at the lesser trochanter and the hip capsule is a potential route by which an infection from a psoas abscess can track into the hip joint [4]. Direct tracking along the iliopsoas muscle between the iliofemoral and iliopubic ligaments to the hip joint is also possible.
Iliopsoas abscess causing an ipsilateral hip septic arthritis is a rare phenomenon [4,5,6,7,8,9,10,11,12]. Again, bilateral Iliopsoas abscess is also rarely reported in literature (3%) [3,13]. We report here a rare case of bilateral primary psoas abscess with osteomyelitis and septic arthritis of both hip joints in a lady with Type II Diabetes.
A 58-year-old diabetic lady presented with complaints of inability to stand or walk subsequent to a fall at home 1 month back. She had a history of high-grade fever with general malaise and anorexia at the time of presentation. There was no history of back pain, abdominal pain, bowel, or bladder disturbances. She had no history of any chronic illnesses other than Type-II diabetes, with adequate control. When she presented to us, empirical anti tuberculosis (TB) treatment had been initiated.
She had bilateral hip tenderness with bilateral inguinal tender lymphadenopathy; the largest being 2.5 × 2.5 cm. Movements of both hips were painfully restricted in all directions. Blood investigations revealed elevated white blood cell count (26000/cumm) with predominant neutrophils. C-reactive protein was elevated (60 mg/l). Her glycaemic control was adequate. Magnetic resonance image (MRI) of the spine taken 1 week after the fall from the previous treating center showed an L4 -L5 disc bulge and she was managed with rest ,dexamethasone (8 mg) twice daily, and analgesics. 3 weeks later, MRI was repeated as symptoms persisted and bilateral iliopsoas abscess with synovitis of the hip was diagnosed (Fig. 1). Empirical anti TB drugs were started at that time, following which she presented to us.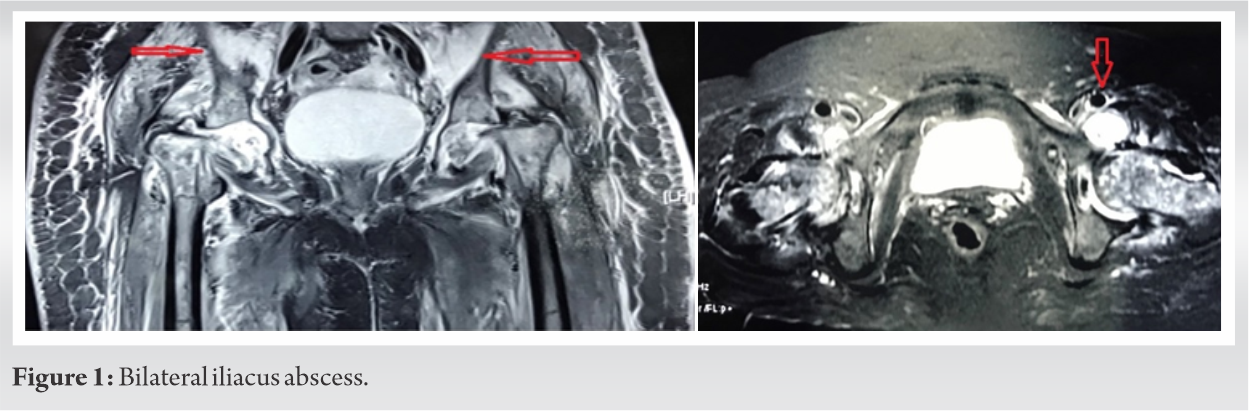
In view of the diagnosis of bilateral psoas abscess, we investigated for any sources of occult infection. Urine culture, blood culture, and sputum culture did not grow any organism. Widal and Brucella antigen was negative. Stool occult blood was also negative. She underwent bilateral iliopsoas abscess drainage through ilioinguinal approach (first window) and the pus grew Streptococcus faecalis sensitive to Gentamycin, Ampicillin, Linezolid, Tetracycline, and Chloramphenicol. Her Xpert TB Polymerase chain reaction was negative and anaerobic and fungal culture also was negative. Following initial I/V antibiotics, she was maintained on oral Linezolid for 6 weeks.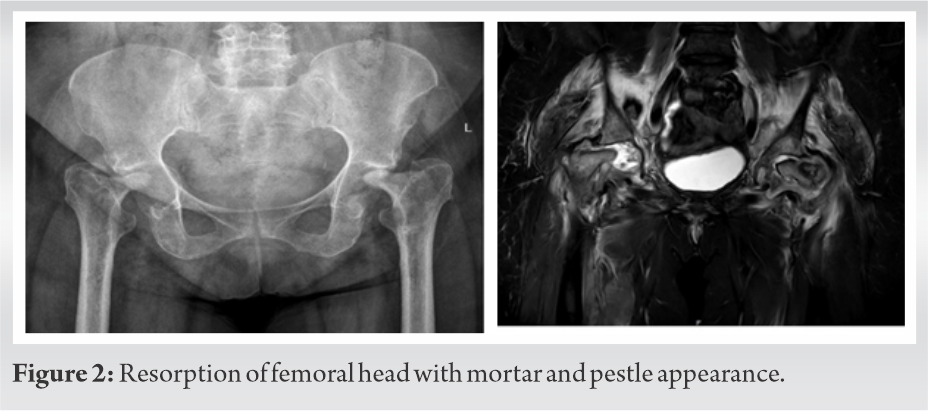
During her subsequent follow-up period, her general condition improved and CRP dropped to normal levels. However, she continued to complain of bilateral hip pain with restricted movements. X-rays of both hips showed mortar and pestle appearance. MRI of both hips showed complete resorption of both femoral heads (Fig. 2). After a disease-free interval of 3 months which was confirmed by a negative C-reactive protein level and negative culture from hip arthrocentesis, she underwent staged total hip replacement of both hips (Fig. 3) [14,15,16]. Intraoperative tissue culture and synovial fluid culture were negative and histopathology did not show any acute inflammation.
Patient has been under regular follow-up for 2.5 years. She remains symptom-free and ambulates independently (Video 1).
The iliacus arises from the iliac wing and inserts into the psoas tendon and lesser trochanter of the femur. The psoas major arises from the transverse processes of the lumbar vertebrae, the intervertebral discs and adjacent vertebral margins of T12 to L5, and the tendinous arches. Together, they form the common iliopsoas muscle, which passes beneath the inguinal ligament and ventral to the hip to insert on the lesser trochanter. It is separated from the hip joint by the iliopectineal (iliopsoas) bursa, which communicates with the hip joint in 15% of individuals [17,18]. Infection can also track to the hip capsule directly along the iliopsoas muscle between the iliofemoral and iliopubic ligaments [4]. This makes the hip joint vulnerable to septic arthritis in the presence of a psoas abscess.
The classical clinical triad consisting of fever, back pain, and limp is present in only 30% of the patients with iliopsoas abscess. Symptoms can be vague and hence careful physical examination is paramount for early diagnosis of this condition. Pain can radiate to the hip and thigh as L2, L3 and L4 nerves innervate the psoas muscle [19]. Hip may be positioned in flexion and external rotation for comfort and this points to the diagnosis. Psoas stretch test [20] also aids in prompt diagnosis. Hydronephrosis due to compression of the ureter or deep vein thrombosis secondary to iliac vein compression may also be presenting features [21]. Psoas abscess could spread to the lower limb and can produce infection of iliopsoas bursae and subsequent septic arthritis of the hip [5]. Our patient didn’t have the classical signs of psoas abscess and this led to delay in diagnosis.
Staphylococcus aureus is the pathogen in 88% of primary psoas abscesses [3]. TB of the spine is the common cause of secondary psoas abscess in developing countries [22,23] while Crohn’s disease is considered as the common cause in developed countries [24,25]. Other predominant organism seen in psoas abscess is Eschericia coli [26].
In our case, the synovitis of the hip joint was thought to be secondary to Pott’s disease and iliopsoas abscess, and anti TB medicines were started by the initial treating physician. But, MRI of the spine did not show any signs of TB spine. Furthermore, TB- PCR, culture, and biopsy were negative for Acid-Fast bacilli. Other secondary causes of psoas abscess were ruled out in our patient before making a diagnosis of primary psoas abscess.
S. faecalis is a common commensal organism of gastrointestinal flora. It is possible that it may have spread hematogenously or through the lymphatics and caused an iliopsoas abscess in this patient.
The patient gave a history of fall preceding the onset of symptoms. Therefore, It is also possible that there could have been injury to the psoas muscle, which increased the chances of abscess formation. Further, the initial administration of steroids could have aggravated the course of the disease process. Being diabetic, the patient may also have been immunocompromised to a certain extent, further predisposing to abscess formation. We are not sure about the role of Inguinal Lymphadenitis and probable suppuration in the formation of the abscess.
The incidence of bilateral psoas abscess is only around 3% [3,13]. Iliopsoas abscess with ipsilateral hip septic arthritis is reported rarely in literature [4,5,6,7,8,9,10,11,12]. Therefore, our patient with primary bilateral iliopsoas abscess and bilateral septic hip arthritis has not been reported in literature till date.
In summary, the original source of infection in our patient was not identified. When a diagnosis of iliopsoas abscess with hip synovitis is made, the possibility of septic arthritis should also be considered. Emphasis on early diagnosis through diligent clinical examination, aspirating the hip joint, pelvic imaging, and early intervention with a combination of appropriate antibiotics, adequate drainage of the abscess, and debridement of infected hip will reduce mortality and morbidity.
Bilateral Iliopsoas abscess with bilateral hip septic arthritis is a rare condition. Moreover, the vague presentation of iliopsoas abscess may lead to delayed diagnosis and increased morbidity and mortality. The importance of meticulous clinical examination cannot be over emphasised for the diagnosis of this condition and appropriate management of the abscess and its possible complications.
References
- 1.Mynter H. Acute psoitis. Buffalo Med Surg J 2009;1881:21202-10. [Google Scholar | PubMed]
- 2.Mallick IH, Thoufeeq MH, Rajendran TP. Iliopsoas abscesses. Postgrad Med J 2004;80:459. [Google Scholar | PubMed]
- 3.Ricci MA, Rose FB, Meyer KK. Pyogenic psoas abscess: Worldwide variations in etiology. World J Surg 1986;10:834-43. [Google Scholar | PubMed]
- 4.Kumagai K, Ushiyama T, Kawasaki T, Matsusue Y. Extension of lumbar spine infection into osteoarthritic hip through psoas abscess. J Orthop Sci 2005;10:91-4. [Google Scholar | PubMed]
- 5.Levitin B, Rubin LA, Rubenstein JD. Occult retroperitoneal abscess presenting as septic arthritis of the hip. J Rheumatol 1982;9:904-8. [Google Scholar | PubMed]
- 6.Compain C, Michou L, Orcel P, Hannouche D, Richette P. Septic arthritis of the hip with psoas abscess caused by Non-typhi Salmonella infection in an immunocompetent patient. Joint Bone Spine 2008;75:67-9. [Google Scholar | PubMed]
- 7.Beredjiklian PK, Adler L, Wong K, Katz M, Yeh GL, Garino JP. Prevertebral abscess with extension into the hip joint. Am J Orthop (Belle Mead NJ) 2001;30:572-5. [Google Scholar | PubMed]
- 8.Talbot NJ, Costa S, Giles NC. Pathological hip fracture following intracapsular spread of a psoas abscess. Injury 2004;35:936-7. [Google Scholar | PubMed]
- 9.O’Leary JM, Lipscomb PR, Dixon CF. Enteric fistula associated with osteomyelitis of the hip and spinal column: A report of 3 cases. Ann Surg 1954;140:897-900. [Google Scholar | PubMed]
- 10.Mccreas ES, Wagner E. Femoral osteomyelitis secondary to diverticulitis. J Can Assoc Radiol 1981;32:181-2. [Google Scholar | PubMed]
- 11.Messieh M, Turner R, Bunch F, Camer S. Hip sepsis from retroperitoneal rupture of diverticular disease. Orthop Rev 1993;22:597-9. [Google Scholar | PubMed]
- 12.Smith WS, Ward RM. Septic arthritis of the hip complicating perforation of abdominal organs. JAMA 1966;195:1148-50. [Google Scholar | PubMed]
- 13.Bresee JS, Edwards MS. Psoas abscess in children. Pediatr Infect Dis J 1990;9:201-6. [Google Scholar | PubMed]
- 14.Chen CE, Wang JW, Juhn RJ. Total hip arthroplasty for primary septic arthritis of the hip in adults. Int Orthop 2008;32:573-80. [Google Scholar | PubMed]
- 15.Bauer T, Lacoste S, Lhotellier L, Mamoudy P, Lortat-Jacob A, Hardy P. Arthroplasty following a septic arthritis history: A 53 cases series. Orthop Traumatol Surg Res 2010;96:840-3. [Google Scholar | PubMed]
- 16.Papanna MC, Chebbout R, Buckley S, Stockley I, Hamer A. Infection and failure rates following total hip arthroplasty for septic arthritis: A case-controlled study. Hip Int 2017;1:63-7. [Google Scholar | PubMed]
- 17.Guerra J, Armbuster TG, Resnick D, Goergen TG, Feingold ML, Niwayama G, et al. The adult hip: An anatomic study. Radiology 1978;128:11-20. [Google Scholar | PubMed]
- 18.Wunderbaldinger P, Bremer C, Schellenberger E, Cejna M, Turetschek K, Kainberger F. Imaging features of iliopsoas bursitis. Eur Radiol 2002;12:409-15. [Google Scholar | PubMed]
- 19.Chern CH, Hu SC, Kao WF, Tsai J, Yen D, Lee CH. Psoas abscess: Making an early diagnosis in the ED. Am J Emerg Med 1997;15:83-8. [Google Scholar | PubMed]
- 20.Wong JG. The psoas signs. Well-described but often forgotten physical examination findings of iliopsoas inflammation. N C Med J 1993;54:598-600. [Google Scholar | PubMed]
- 21.Arai Y, Kawakami T, Soga H, Okada Y. Psoas abscess associated with iliac vein thrombosis and piriformis and gluteal abscesses. Int J Urol 1999;6:257-9. [Google Scholar | PubMed]
- 22.Chawla K, D’Souza A, Bhat NS, Mukhopadhayay C. Primary tubercular psoas abscess: A rare presentation. J Infect Dev Ctries 2012;6:86-8. [Google Scholar | PubMed]
- 23.Goni V, Thapa BR, Vyas S, Gopinathan NR, Manoharan SR, Krishnan V. Bilateral psoas abscess: Atypical presentation of spinal tuberculosis. Arch Iran Med 2012;15:253-6. [Google Scholar | PubMed]
- 24.Agrawal SN, Dwivedi AJ, Khan M. Primary psoas abscess. Dig Dis Sci 2002;47:2103-5. [Google Scholar | PubMed]
- 25.Shields D, Robinson P, Crowley TP. Iliopsoas abscess--a review and update on the literature. Int J Surg 2012;10:466-9. [Google Scholar | PubMed]
- 26.Wong OF, Ho PL, Lam SK. Retrospective review of clinical presentations, microbiology, and outcomes of patients with psoas abscess. Hong Kong Med J 2013;19:416-23. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 August 6, 2024 A Rare Case of Periprosthetic Fracture with Fracture of Femoral Stem around a Bipolar Hemiarthroplasty
August 6, 2024 A Rare Case of Periprosthetic Fracture with Fracture of Femoral Stem around a Bipolar Hemiarthroplasty January 1, 2026 Peri-implant Femoral Fracture: An Uncommon Presentation in a Patient with Hallermann–Streiff Syndrome – A Case Report and Review of the Literature
January 1, 2026 Peri-implant Femoral Fracture: An Uncommon Presentation in a Patient with Hallermann–Streiff Syndrome – A Case Report and Review of the Literature March 10, 2023 The Glomus Tumor of Finger – A Case Series
March 10, 2023 The Glomus Tumor of Finger – A Case Series October 10, 2021 Report of a Case of Cold Urticaria Following Cryotherapy – Need for Screening for Untoward Effects of Cryotherapy in Physical Therapy Clinical Practice
October 10, 2021 Report of a Case of Cold Urticaria Following Cryotherapy – Need for Screening for Untoward Effects of Cryotherapy in Physical Therapy Clinical Practice