
Leg impalement presentation and treatment.
Dr. Gabriel Pina, Department of Orthopaedics and Traumatology, Centro Hospitalar Tondela-Viseu, Portugal. E-mail: gabrielpina950@hotmail.com
Abstract
Introduction: Impalement injuries are defined as rare, high-energy lesions caused by foreign bodies, usually steel bars or wooden objects, which pierce body cavities or extremities and remain interposed in the perforated body region. They usually occur with road accident or civil construction falls.
Case Report: A 24-year-old male patient was admitted at the emergency department after a motorcycle accident, resulting a left leg impalement with a wooden object. A partial deep peroneal nerve palsy and a proximal third fibula fracture were observed. The foreign body removal and wound debridement were performed. The patient evolved favorably without complications, with complete neurological recovery and returning to his normal life activities.
Discussion: Impalement injuries represent a challenge in pre-hospital care, emergency room, and operating room hospital care, due to its rarity and specificity: Type of object, anomalous foreign body location, and trajectory. There is a consensus that whenever possible, it should be removed in the operating room, due to the foreign body may be tamponing a major arterial laceration, thus preventing massive hemorrhage.
Conclusion: Neurovascular injury exclusion, foreign body removal in the operating room, debridement, and antibiotic prophylaxis represent the treatment basis of these injuries.
Keywords: Impalement, Trauma, Leg
Impalement is defined as injuries caused by foreign bodies, usually steel bars, or wooden objects, which pierce body cavities or extremities and remain interposed in the perforated body region [1]. This type of trauma corresponds to an injury spectrum occasionally reported in the literature, being more frequent in the thoracic, abdominal and perineal areas [2,3,4]. Its report at the extremity level is even rarer [5]. They usually occur on road accidents or civil construction falls [6]. The aim of this work was to report a leg impalement clinical case, whose anatomical location is not reported in the scientific literature.
A 24-year-old male patient, was admitted at the emergency department with his left leg impalement with a wooden object after a motorbike fall. (Fig. 1.1 and 1.2).
At the initial approach in the emergency room, the patient did not have impaired airway, ventilation, and circulation. In the secondary evaluation, presented a wooden object proximal third left leg impalement with an antero-posterior direction. The leg entry wound was at the antero-external aspect and an exit wound on the posterior aspect, without active bleeding. Upon vascular evaluation, the patient had a vacularized limb, with no anterior tibial pulse, and normal posterior tibial pulse. Lower limb neurological assessment showed a tibial nerve partial sensory deficit and foot dorsiflexion MRC Grade 3 muscular strength. Superficial peroneal nerve function was normal. The patient started at the emergency room, prophylactic intravenous antibiotics with ceftriaxone 2 g / day and gentamicin 160 mg / day for 2 days. Leg AP and lateral X-rays were requested. Where the presence of a foreign body was observed in the proximal tibio-peroneal space with proximal third fibula shaft fracture (Fig. 23.1 and 2.24).
The patient was urgently sent to the operating room for foreign body removal and wound debridement. During positioning, we selected a right lateral decubitus position, since it allowed us to approach the entry and exit wounds, and the foreign object did not conflict with the operating table. A tourniquet was applied but not inflated. The patient was then subjected to foreign body removal through the entry and exit holes after sectioning the anterior foreign body end with a bone saw, allowing the passage of the foreign body in a shorter length through the created path, decreasing iatrogenic injuries risk during its removal. After foreign body extraction, wound exploration and debridement were performed. Anterior tibial pulse was recovered after foreign body removal. Deep peroneal nerve and anterior tibial artery exploration were realized and no anatomical interruption was documented. No major bleeding was observed after impaled object removal. Primary wound closure was not performed. (Fig. 3.15 and 3.26). No immobilization was applied for fibula fracture treatment.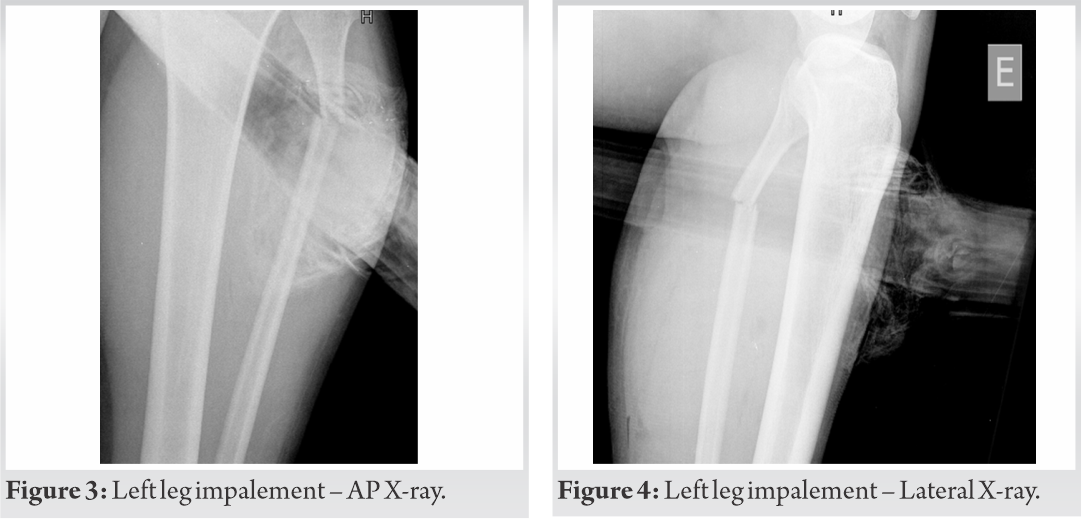
In the early post-operative period, wounds evolved favorlyfavor without infection signs and foot dorsiflexion MRC Grade 4 muscular strength was observed. On the 3rd post-operative day, the wounds were sutured. The patient was discharged on the 5th post-operative day without early complications. Walk training according to pain tolerance was performed and advised. (Fig. 4.17, 4.2, 5.1 and- 5.210).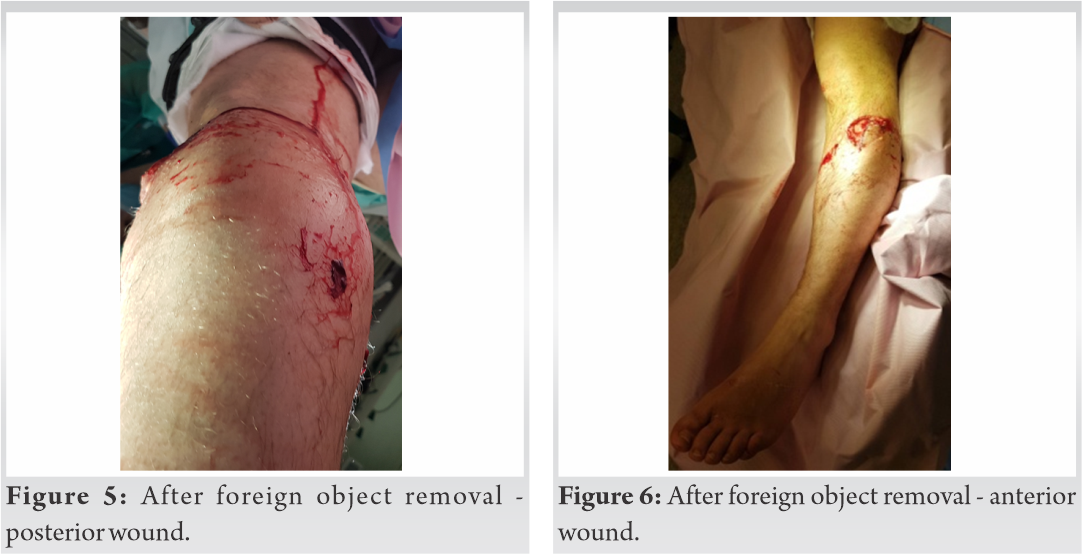
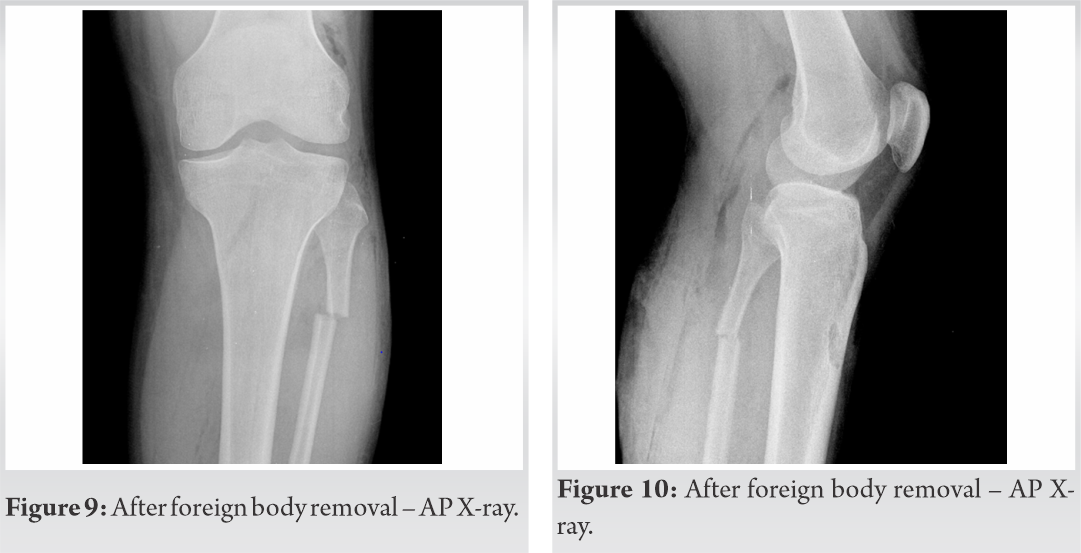
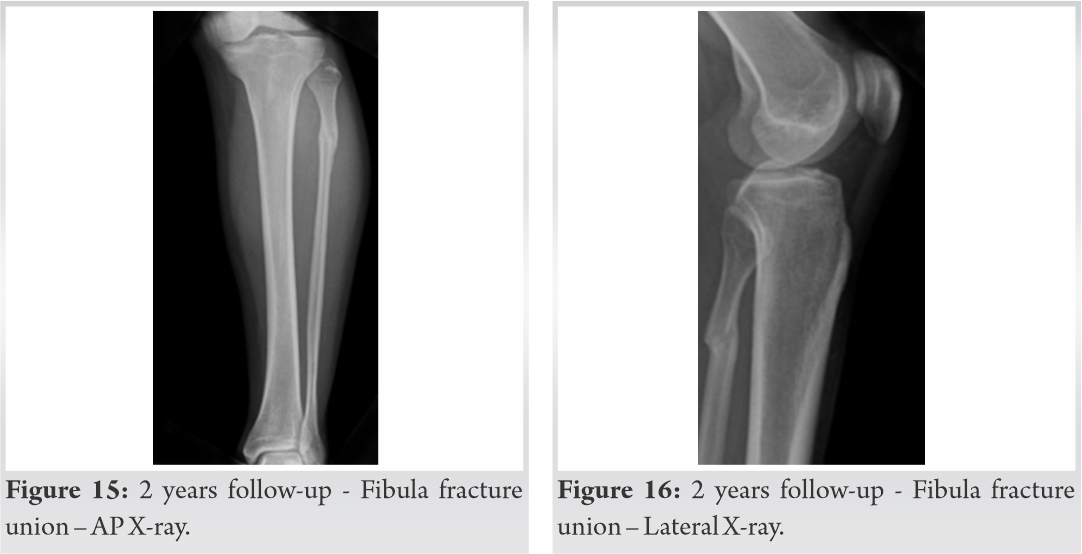
The patient was followed up at 2 weeks, 3 months, 6 months, 1 year, and 2 years. Wound healing, foot dorsiflexion MRC muscular strength, knee and ankle range of motion, walking ability, and leg X-rays were recorded. At 2 weeks, the suture material was removed, and normal wound healing was observed, and physical therapy was started. At 6 months, foot dorsiflexion Grade 5 MRC muscular strength and normal walking ability was observed. The fibula fracture evolved to union without complications. The patient returned to normal life activities without limitations. (Fig. 6.111, 6.2, 7.1, 7.2, 8.1 and 8.2-16).

Impalement injuries represent a challenge both in pre-hospital care, emergency room, and operating room care, due to its rarity and traumatic specificity: Foreign object features, anatomical location, and trajectory influence patient pre-hospital transportation and operating room removal approach [7].
Impalement injuries represents high-energy trauma that causes injuries by blunt, piercing, and lacerating mechanism. The main risk group for impale type injuries is construction industry workers [8].
All impalement trauma patients should be approached according to ATLS principles, assessing and ensuring the airway, ventilation and hemodynamic stability, which includes limb vascular evaluation, since major vessel laceration could be present [9,10]. After patient’s patient’s vital parameters stabilization, limb soft tissue, and bone assessment should be the next priority [17,11]. Complementary radiographs must be requested in order to establish foreign object trajectory and precise location [11,12].
There is a consensus that impaled object removal should be in the operating room. The reason lies in the fact that the foreign body may be tamponing a major arterial laceration, preventing massive hemorrhage [9, 10, 12, 13 ]. However, the foreign object ends can be cut to facilitate transport, positioning, and removal [13,14]. Foreign body removal before surgery also has advantages: it facilitates patient correct positioning for better wound approach and prevents contact between the sterile operative field and the contaminated foreign body [14,15].
In our clinical case, impaled foreign body removal was performed in the operating room. A lateral decubitus position was selected, since the foreign body was antero-posteriorly oriented. This position would also be chosen if the object had been removed preoperatively, for entry and exit wounds approach. We can conclude that it did not interfere with the optimal positioning. On the other hand, after the removal of the foreign body, the surgical drapes were replaced by sterile drapes, without compromising the infectious risk.
Impalement injury can be defined in two types: Type I, more common, the impaled human body moves towards the foreign object that is immobile.
Type II, less common, the foreign body in motion impales the immobile human body [15,16].
Kelly et al. reported four impalement cases, three were limb impalement, 1one forearm impalement, and two thigh impalements, without neurovascular injuries, treated with entry and exit holes foreign bodies removal, without complications [16,17]. Banshelkikar and all reported a thigh impalement with an iron bar without neurovascular injuries. The impaled object was removed using the entry and exit holes, without complications [17,11]. Ketterhagen and Wassermann, in a case report, reported a foreign body impaled object removal using a fistulotomy approach, joining the entry, and exit holes [13,14].
One of the most important therapeutic measures in these injuries is infection prevention, with wound debridement and washing with saline and prophylactic antibiotics. Anti-tetanus immunization should always be considered since most of these clinical cases occur with iron bars [10,11,12,13,14,15,16,17].
Impalement injuries represent a rare type of trauma with a specific therapeutic approach. The initial approach to the limbs should always include neurovascular injuries exclusion. Operating room foreign object removal, debridement, and antibiotic prophylaxis representss impalement injuries treatment basis.
Neurovascular exclusion, foreign body removal and wound debridement are the impalement injury manstay treatments.
References
- 1.Hyde MR, Schmidt CA, Jacobson JG, Vyhmeister EE, Laughlin LL. Impalement injuries to the thorax as a result of motor accidents. Ann Thorac Surg 1987; 43:189-90. [Google Scholar | PubMed]
- 2.Rautji R, Behera C, Dogra TD. An unusual fatal construction site injury in India: A case report. Med Sci Law 2009; 49:222-3. [Google Scholar | PubMed]
- 3.Liu YW, Tsai DL, Chou SH, Chen CW. Video-assisted thoracoscopic surgery for thoracic impalement with an iron rod. Ann Thorac Surg 2017; 104:1438-9. [Google Scholar | PubMed]
- 4.Amarjothi JM, Williams R, Inpharasun SA. Impalement injury with transanal prolapse of bowel content due to intraperitoneal rectal tear. Indian J Surg 2015; 77:72. [Google Scholar | PubMed]
- 5.El Alwany AM. Wrist watch causing impalement of the hand by a thick steel rod. J Hand Surg Eur Vol 2010; 35:684. [Google Scholar | PubMed]
- 6.Sawhney C, D’Souza N, Mishra B, Gupta B, Das S. Management of a massive thoracoabdominal impalement: A case report. Scand J Trauma Resusc Emerg Med 2012; 18:57. [Google Scholar | PubMed]
- 7.Golder SK, Friess H, Shafighi M, Kleeff JH, Büchler MW. A chair leg as the rare cause of a transabdominal impalement with duodenal and pancreatic involvement. J Trauma 2001; 51:164-7. [Google Scholar | PubMed]
- 8.Khandelwal A, Singh GP, Kharwar RK, Deganwa M. An iron rod restricting access to airway: An unusual presentation. Anaesthesiol Intensive Ther 2017; 49:241-2. [Google Scholar | PubMed]
- 9.Shahlaie K, Chang DJ, Anderson JT. Nonmissile penetrating spinal injury. Case report and review of the literature. J Neurosurg Spine 2006; 4:400-8. [Google Scholar | PubMed]
- 10.Horowitz MD, Dove DB, Eismont FJ, Green BA. Impalement injuries. J Trauma 1985; 25:914-6. [Google Scholar | PubMed]
- 11.Kelly IP, Attwood SE, Quilan W, Fox MJ. The management of impalement injury. Injury 1995; 26:191-3. [Google Scholar | PubMed]
- 12.Ozaydin S, Gulleroglu A, Karaaslan B, Celebi S, Besik C, Toker MK, et al. Penetrating injury caused by a long iron bar: A case report. North Clin Istanb 2018; 5:75-8. [Google Scholar | PubMed]
- 13.Tokushige J, Inokuchi A, Kawaguchi H. Impalement injuries involving the spinal canal. J Orthop Sci 2000; 5:614-7. [Google Scholar | PubMed]
- 14.Ketterhagen JP, Wassermann DH. Impalement injuries: The preferred approach. J Trauma 1983; 23:258-9. [Google Scholar | PubMed]
- 15.Sarıca C, Yücetaş SC, Üçler N. Steel rod impalement injuries involving the spine: A case report and literature review. Ulus Travma Acil Cerrahi Derg 2019; 25:417-23. [Google Scholar | PubMed]
- 16.Angelopoulos S, Mantzoros I, Kyziridis D, Fontalis A, Parpoudi S, Konstandaras D, et al. A rare case of a transabdominal impalement after a fall from a ladder. Int J Surg Case Rep 2016; 22:40-3. [Google Scholar | PubMed]
- 17.Banshelkikar SN, Sheth BA, Dhake RP, Goregaonkar AB. Impalement injury to thigh: A case report with review of literature. J Orthop Case Rep 2018; 8:71-4. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 9, 2018 Bilateral Spontaneous Bony Ankylosis of the Elbow Following Burn: A Case Report and Review of the Literature
September 9, 2018 Bilateral Spontaneous Bony Ankylosis of the Elbow Following Burn: A Case Report and Review of the Literature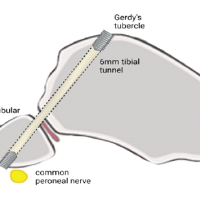 March 1, 2025 Biological Stabilization of Proximal Tibiofibular Joint Recurrent Instability with Semitendinosus Graft – Surgical Technique and Case Report
March 1, 2025 Biological Stabilization of Proximal Tibiofibular Joint Recurrent Instability with Semitendinosus Graft – Surgical Technique and Case Report October 1, 2025 Salvaging Femur Head in a Pipkin Type III Femoral Head Fracture with Open Reduction and Internal Fixation Using Herbert Screw Fixation: A Rare Case Report
October 1, 2025 Salvaging Femur Head in a Pipkin Type III Femoral Head Fracture with Open Reduction and Internal Fixation Using Herbert Screw Fixation: A Rare Case Report January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure
January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure