
Adherence to the key principles of anatomical reduction and stable osteosynthesis are critical in the successful management of unusual Monteggia variants.
Dr. Rajpreet Sahemey, Department of Trauma and Orthopaedics, Birmingham Heartlands Hospital, UK, B9 5SS. E-mail: rajpreet.s@gmail.com
Abstract
Introduction: The Monteggia fracture is a fracture to the proximal third of ulna associated with a radial head dislocation. Although this is well described and classified in adults, it is uncommon in children. Identifying growth plate trauma and subsequent surgical management are of critical importance. This report identifies a unique variant of Monteggia fracture with a Salter-Harris Type I injury of the radial head instead of a dislocation, and how it was successfully stabilised with a closed reduction.
Case Rport: We present a case of a nine 9 year-old female admitted to our unit with a deformed upper extremity following a fall from height. This was a closed and isolated injury without neurovascular compromise. Radiographs revealed a displaced fracture to the proximal ulna shaft. Unlike a true Monteggia, the radial fracture went through the proximal physis with anterior divergence of the distal fragment. The radiocapitellar joint remained congruent. The ulna fracture was stabilized with open reduction and plate osteosynthesis whilst the radial injury underwent closed reduction and intramedullary pinning with excellent outcomes and maintenance of full range of motion.
Conclusion: This case highlights a new variant and successful outcome following a closed reduction intramedullary fixation technique in this emergent pattern of injury. We highlight the need for a classification of these fractures in children.
Keywords: Case report, Monteggia, growth plate, pediatric, fracture, trauma, variant.
Monteggia fractures involve a fracture of the proximal third of ulna and a radial head dislocation. However, it may be part of a more complex injury involving the olecranon, coronoid, and ligamentous structures. The fracture pattern can lead to threatened skin integrity, loss of range of motion, and posterior interosseous neuropathy. In children, associated growth plate injuries must be taken into consideration.
There are few cases documented in the literature of a growth plate injury to the radius without radial head dislocation. We present a rare and interesting case of a Monteggia variant with a Salter-Harris Type I fracture to the proximal radial physis and anterior displacement. Management entailed of stable plate osteosynthesis of the ulna with a closed reduction intramedullary pinning of the radial physis. Our approach protected the annular ligament and permitted a successful outcome.
A 9 year-old, right handed child presented to a district general hospital after having fallen from 1.5 m in height. Physical examination by the orthopaedic team reported an isolated and painful deformation of her right upper extremity. This was a closed injury without neurovascular deficit or immediate threat to skin. She was fully assessed according to trauma protocols and placed in an above elbow back slab to splint the injury.
Plain film radiographs (Fig. 1) demonstrated an oblique fracture of the proximal third of ulna shaft with an apex anterior angulation of 30° and a Salter-Harris Type I fracture through the proximal radial physis with an anteriorly displaced proximal metaphysis. The proximal radial epiphysis however appeared to be congruent with the capitellum in orthogonal views.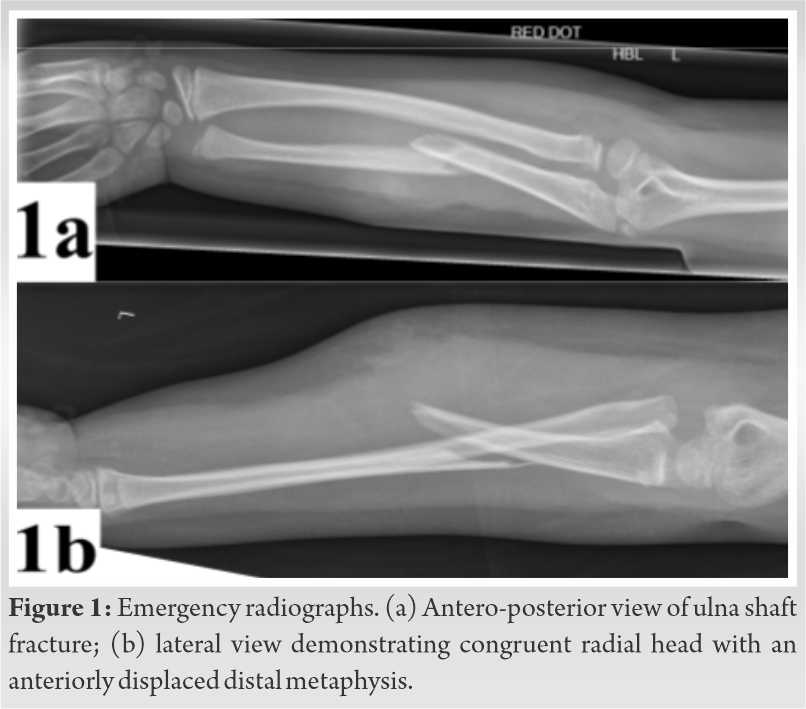
Given the history, examination and radiographic features of a significantly displaced growth plate fracture, the patient was taken to theatre under general anaesthesia and without tourniquet.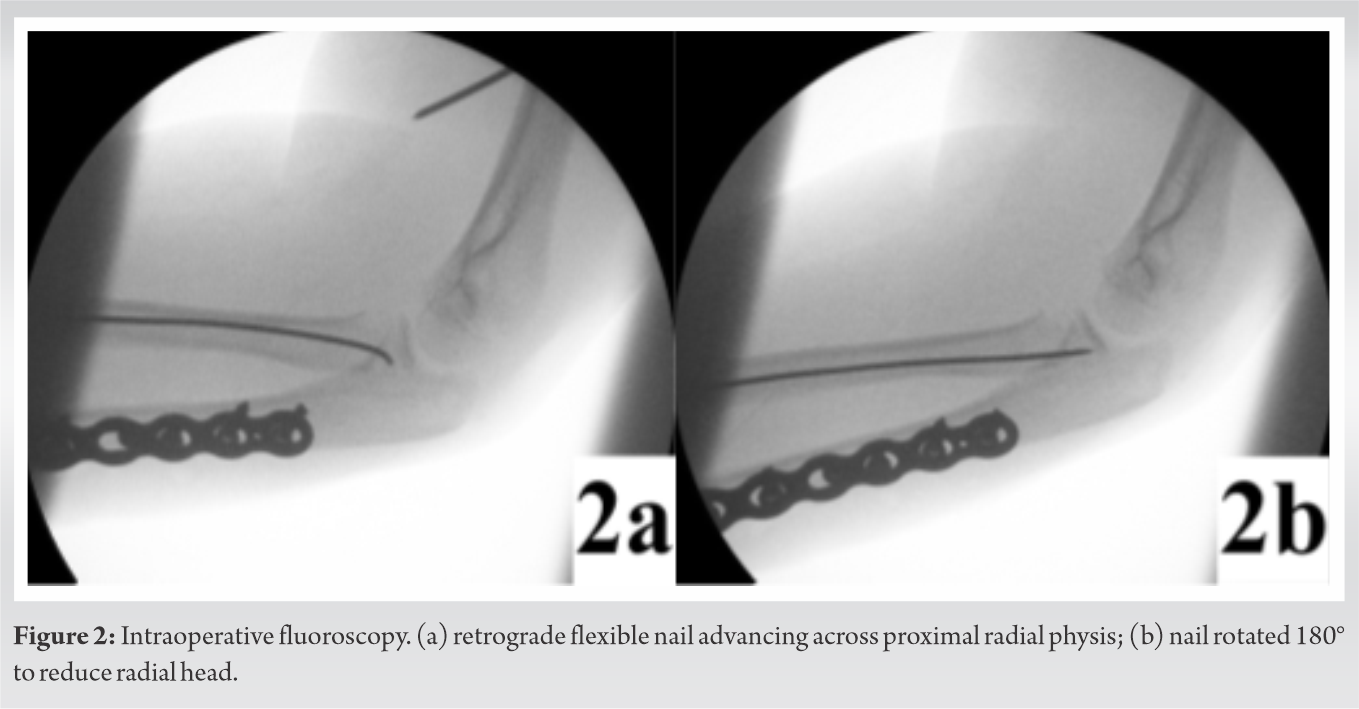
The ulna injury was addressed through a subcutaneous approach. The fracture was reduced and stabilised with an interfragmentary lag screw and Stryker VariAx Compression plate (Fig. 2). Despite manipulation, there was persistent dislocation of the proximal radial metaphysis therefore we opted for an intramedullary approach, in a manner described by Métaizeau et al. [1] and Tarallo et al. [2]. A 1.5 mm Stryker T2 Flexible Nail was introduced at the distal radial metaphysis and advanced proximally up to the physeal fracture site. A 1.4 mm Kirschner wire was then used percutaneously as a lever arm to aid in the reduction of the proximal epiphyseal fragment before advancing the intramedullary nail cranially across the fracture site with the proximal end of the nail fixing in the epiphysis. The intramedullary wire was rotated through 180 causing the proximal fragment to translate medially and result in an anatomical reduction of the radial head. After confirming stability under fluoroscopic control, the distal nail end was cut, bent and skin closed. The limb was splinted in an above elbow back slab in a position of elbow flexion and supination.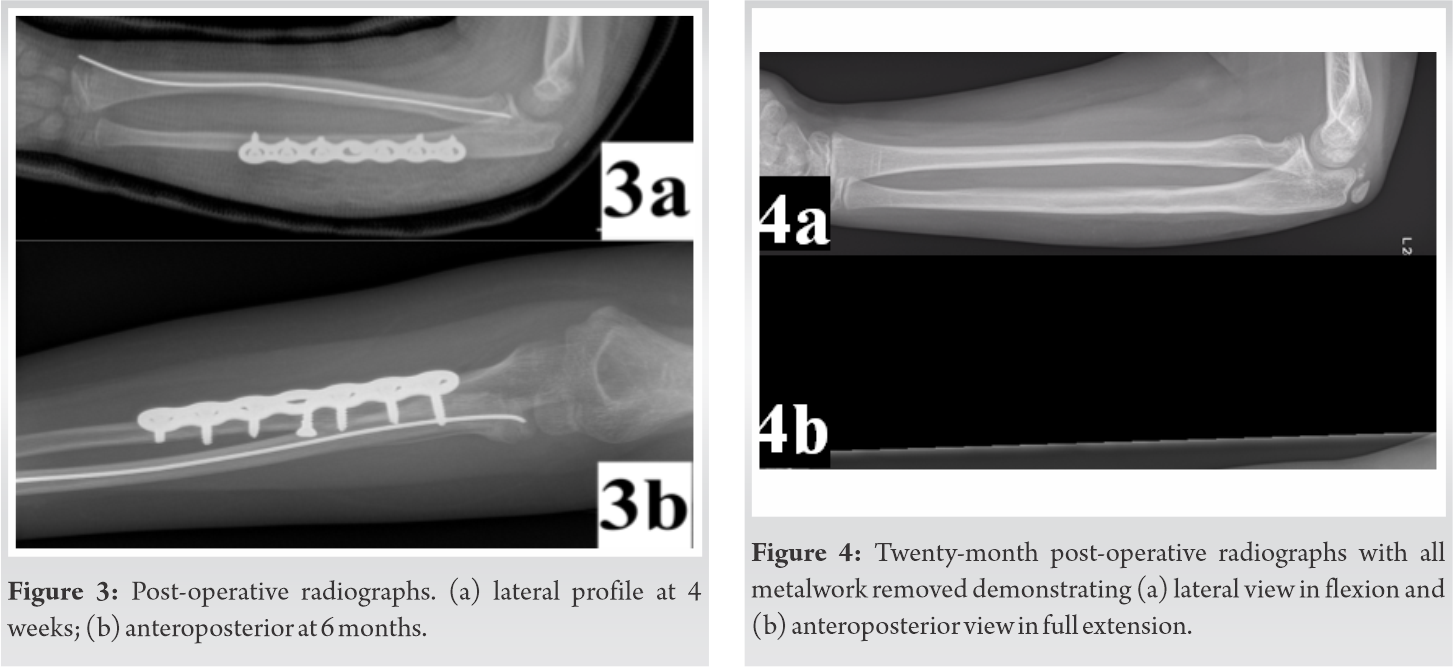
There was no post-operative complication. She was placed into a full arm cast after 1 week for a total of 4 weeks immobilisation before commencing active rehabilitation. At 6 weeks there was radiological evidence of fracture union and maintenance of anatomical reduction (Fig. 3).
At 6 months follow-up the patient did not report any difficulty with daily activity and a pain-free return to full function. Physical examination demonstrated excellent range of motion comparable with the uninjured limb (full supination/pronation, flexion 140° and extension +5°). Despite the presence of the centromedullary nail across the physis, there was no evidence of cubitus valgus. The ulna plate and radial nail were removed 8 months post operatively without complication. At 21 months follow-up radiographs demonstrate complete bony union of both fracture sites with no growth arrest or radiological deformity (Fig. 4). The patient maintained her full and complete range of motion comparable to the uninjured side (Fig. 5).
The pattern of injury originally reported by Giovanni Battista Monteggia in 1814 described a fracture of the ulna shaft associated with an anterior dislocation of the radial head in adults [3]. Later work by Bado classified the complexities of Monteggia fractures into four distinct lesions and equivalent variants [4]. Whilst Monteggia fractures are well documented and classified in adults, this is a relatively uncommon entity in children. Peak incidence in children occurs in the 4–10 age groups and represents 0.4% of all forearm fractures [5]. In 1985, Letts et al. [6] proposed a paediatric classification based on the Bado Type I injury which is reported to be the most common fracture pattern in this group [7]. Their body of work was based on the degree of ulna injury from its plastic deformation to complete fracture, but always in the presence of a radial head dislocation. The Monteggia injury we report here not only has a displaced ulna shaft fracture but also with an associated proximal Salter-Harris Type I fracture with an anteriorly displaced distal fragment and intact radiocapitellar joint, which has not previously been described.
Growth plate injury can be subtle and often overlooked in Monteggia fractures, therefore surgeons must be vigilant and actively look for associated physeal trauma such as in this case [8]. Reina et al. have previously reported a Monteggia Salter-Harris Type I variant with a posteriorly displaced distal fragment [9] and ElKhouly et al. described a similar injury but with a Salter-Harris Type II fracture [10]. With the many variants of Monteggia fractures, we highlight that further work is required toward classifying these injuries in children.
The few cases of adolescent Monteggia equivalent lesions reported in the literature describe a number of injuries involving radial neck and olecranon fractures with a concomitant radial head dislocation. Factors that led to poor outcomes in these cases such as recurrent radial head dislocation suggests that the stability of the annular ligament is paramount to a successful outcome [11,12].
Reina et al proposed a “bottle-opener” mechanism whereby the soft tissues surrounding the radial head including the annular ligament, lateral collateral ligament, and capsule act as a restraint around epiphysis during hyperextension. Thus, the force is transmitted through the relatively weaker growth plate resulting in a Salter-Harris variant fracture and metaphyseal displacement [9]. Uniquely in our case however, the annular ligament and soft tissues were intact which permitted a closed reduction of the growth plate fracture and an early return to full range of motion post operatively.
The management of Monteggia injuries warrant reduction and stable osteosynthesis of the ulna fracture which can then aid in the subsequent reduction of the radial head. This case however was a Salter-Harris Type I fracture rather than a dislocation and therefore required stable fixation. The modified Metaizeau technique we employed in this case is reproducible and has excellent results in the literature [1,9,13]. In some cases, soft tissue interposition may require an open reduction and repair of the annular ligament. In our case, had the initial reduction manoeuvre been unsuccessful then not only would we have to convert to open reduction but also advance the nail antegrade, which would have been challenging with the existing retrograde nail already partially in situ. Therefore, pre-operative planning and thorough screening of the radial injury with a trial closed reduction may be recommended before proceeding with an open-proximal or closed-intramedullary approach.
The long-term sequelae arise from avascular necrosis of the radial head [14], neurovascular injury, infection and disruption of growth potential. An intramedullary approach preserves the soft tissues and blood supply, is less traumatic when compared with screw fixation, and permits for easier removal of metalwork [9].
Paediatric Monteggia fractures are an infrequent occurrence such as in this case of an unusual variant combined with a unique growth plate injury to the radial head without true dislocation. Surgeons must be vigilant of these emerging complex and unstable injuries which may require further classification. We have proven that a successful surgical outcome and maintenance of full range of motion owes to the principles of anatomical reduction, stable osteosynthesis, and preservation of soft tissues.
Growth plate injuries are complex and have ever increasing variants. Clinical and radiographic evaluation of the fracture is essential. Key principles of anatomical reduction and stable fixation will determine a successful outcome.
References
- 1.Métaizeau JP, Prévot J, Schmitt M. Reduction and fixation of fractures of the neck of the radius by centro-medullary pinning. Rev Chir Orthop Reparatrice Appar Mot 1980;66:47-9. [Google Scholar | PubMed]
- 2.Tarallo L, Mugnai R, Fiacchi F, Capra F, Catani F. Management of displaced radial neck fractures in children: Percutaneous pinning vs. elastic stable intramedullary nailing. J Orthop Traumatol 2013;14:291-7. [Google Scholar | PubMed]
- 3.Rehim SA, Maynard MA, Sebastin SJ, Chung KC. Monteggia fracture-dislocations: A historical review. J Hand Surg 2014;39:1384-94. [Google Scholar | PubMed]
- 4.Bado JL. The Monteggia lesion. Clin Orthop 1967;50:71-86. [Google Scholar | PubMed]
- 5.Peter N, Myint S. Type I Monteggia lesion and associated fracture of the distal radius and ulna metaphysis in a child. CJEM 2007;9:383-6. [Google Scholar | PubMed]
- 6.Letts M, Locht R, Wiens J. Monteggia fracture-dislocations in children. J Bone Joint Surg Br 1985;67:724-7. [Google Scholar | PubMed]
- 7.Beaty J, Kasser J. Rockwood and Wilkins’ Fractures in Children. 7th ed., Vol. 92-B. New York: Lippincott, Williams & Wilkins; 2010. [Google Scholar | PubMed]
- 8.Perron AD, Miller MD, Brady WJ. Orthopedic pitfalls in the ED: Pediatric growth plate injuries. Am J Emerg Med 2002;20:50-4. [Google Scholar | PubMed]
- 9.Reina N, Laffosse JM, Abbo O, Accadbled F, Bensafi H, Chiron P. Monteggia equivalent fracture associated with Salter I fracture of the radial head. J Pediatr Orthop B 2012;21:532-5. [Google Scholar | PubMed]
- 10.ElKhouly A, Fairhurst J, Aarvold A. The MonteggiaFracture: Literature review and report of a new variant. J Orthop Case Rep 2018;8:78-81. [Google Scholar | PubMed]
- 11.Ruchelsman DE, Klugman JA, Madan SS, Chorney GS. Anterior dislocation of the radial head with fractures of the olecranon and radial neck in a young child: A Monteggia equivalent fracture-dislocation variant. J Orthop Trauma 2005;19:425-8. [Google Scholar | PubMed]
- 12.Ramsey RH, Pedersen HE. The Monteggia fracture dislocation in children. Study of 15 cases of ulnar-shaft fracture with radial-head involvement. JAMA 1962;182:1091-3. [Google Scholar | PubMed]
- 13.Ursei M, de Gauzy JS, Knorr J, Abid A, Darodes P, Cahuzac JP. Surgical treatment of radial neck fractures in children by intramedullary pinning. Acta Orthop Belg 2006;72:131-7. [Google Scholar | PubMed]
- 14.Young S, Letts M, Jarvis J. Avascular necrosis of the radial head in children. J Pediatr Orthop 2000;20:15-8. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2016 Posterior Hip Dislocation with Ipsilateral Femoral Head and Shaft Fracture – Using a Temporary External Fixator as a Method for Closed Reduction
November 10, 2016 Posterior Hip Dislocation with Ipsilateral Femoral Head and Shaft Fracture – Using a Temporary External Fixator as a Method for Closed Reduction November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture
November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture March 10, 2017 Editorial – New Orthopaedic Residents and Research: How do we Approach
March 10, 2017 Editorial – New Orthopaedic Residents and Research: How do we Approach February 10, 2021 Reviewers Acknowledgement & Photo-gallery February 2021
February 10, 2021 Reviewers Acknowledgement & Photo-gallery February 2021