
Medial malleolar osteotomy with smooth K-wire fixation appears to be a safe method for gaining access to the talus when required for reduction and/or fixation of pediatric talus fractures.
Mr. Cindy L. Austin, MS, CCRP, Trauma & Burn Research, Mercy Hospital - Springfield, 1235 E Cherokee, Springfield, MO 65804, USA. E-mail: cindy.austin@mercy.net
Abstract
Introduction: Talus fracture injuries are rare and most literature pertains to fractures in skeletally mature adults. It is unusual for pediatric talus fractures to be treated operatively and is normally treated with immobilization. The location of the talus fracture required a medial malleolar osteotomy to facilitate exposure and reduction, which was fixed with temporary smooth K-wires. The authors were unable to identify a previous description of this technique in the literature.
Case Report: An 11-year-old female was referred to our hospital due to polytraumatic injuries sustained in a roll-over MVC. A displaced fracture of the talus body was present. Due to the fracture location, a medial malleolar osteotomy was required for exposure. An open reduction and internal fixation was performed using subchondral minifragment screws under general anesthesia. The patient healed uneventfully, regained a normal gait and full, pain-free range of motion.
Conclusions: Medial malleolar osteotomy with smooth K-wire fixation appears to be a safe method for gaining access to the talus when required for reduction and/or fixation of pediatric talus fractures.
Keywords: Adolescent, talus fracture, osteotomy.
The talus is the most superior bone of the foot. It has a trapezoidal-shaped upper surface that articulates with the tibia and fibula to form the ankle joint. Body weight is transferred from the tibia to the talus then on to the calcaneus (heel bone) which distributes the weight to the ground. Talus fracture injuries are rare and most literature pertains to fractures in skeletally mature adults [1]. The injury may be less common in children due to the cartilaginous nature of the talus in children, and thus, the incidence of pediatric talus fractures is approximately a fifth of the adult fracture rate [2]. Most talus fractures occur in the talar neck, with only 13–23% of them occurring in the body of the talus [3]. Furthermore, it is unusual for pediatric talus fractures to be treated operatively and is normally treated with immobilization [4], however, occasionally severe displacements are treated with internal fixation. These fractures are often caused by a significant axial load on a dorsiflexed foot [4].
This case involves an 11-year-old female who was a restrained, backseat passenger in a motor vehicle rollover. On EMS arrival, the patient was found hanging partially out of the back, driver side window. The patient was noted to be tachycardic and hypotensive with a subarachnoid hemorrhage, internal carotid artery dissection. In addition, there were multiple skeletal injuries, including an open Type 3 supracondylar humerus fracture that was treated urgently, right meta-diaphyseal distal tibia and fibula fractures. There was initially no report of left ankle or foot injury, and the preliminary radiographs were read as negative for fracture. Subsequently, however, the patient reported persistent pain in the left ankle, and a computed tomography (CT) scan was ordered, identifying a displaced left talar body fracture (Fig. 1). The CT scan revealed that the body of the talus was comminuted and was dislocated posteriorly relative to the subtalar joint. There was also considerable impaction between the calcaneus and the talar body. Due to displacement, surgery was indicated, and due to the posterior location of the fracture line and need for an anatomic reduction with rigid fixation would necessitate medial malleolar osteotomy.
The patient was positioned in the supine position, placed under general anesthesia with neuromuscular blockade and pre-operative antibiotics were administered. The left leg was fitted with a tourniquet and a medial incision centered between and paralleling the anterior tibial and posterior tibial tendons was utilized. As anticipated, it was apparent that a medial malleolar osteotomy would be required. The physis was located with the fluoroscope, and the osteotomy was performed distal to the physis using an oscillating saw and completed with an osteotome.
The patient’s talar body was in a posteriorly dislocated position and initial attempts to reduce this through simple manipulation was unsuccessful, therefore, a 3.2 mm Steinmann pin was placed through the calcaneus to allow for direct longitudinal distraction. A periosteal elevator was placed between the posterior facet of the calcaneus and the talus, and the talar body was levered back into position. With the talar body dislocation reduced, the fracture reduction was fine-tuned and K-wired, and 2.4 and 2.0 mm counter sunk lag screws were then placed for final fixation (Fig. 2).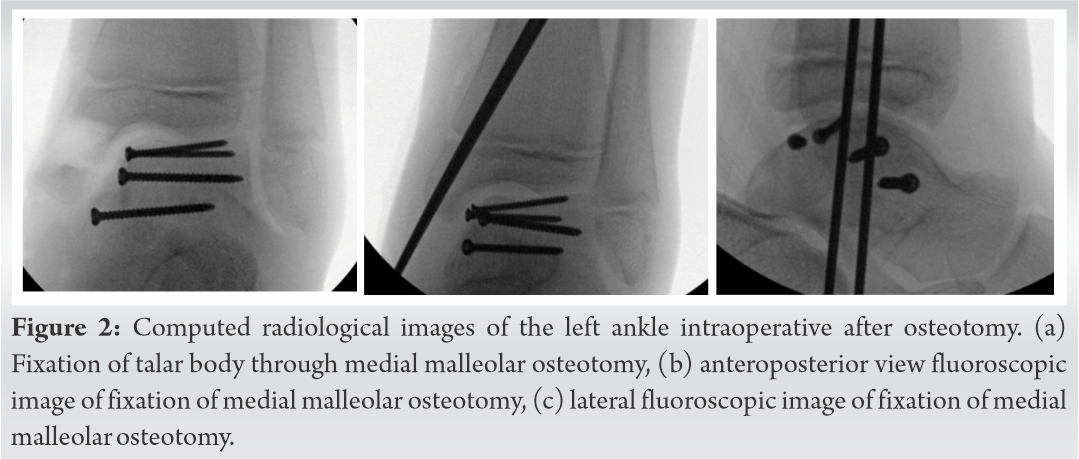
Before closing the wound, the medial malleolar osteotomy was reduced. The incision was re-approximated and a percutaneously placed smooth 2.4 mm K-wire was used to neutralize the osteotomy. Once the skin was closed, a second 2.4 mm K-wire was placed in a parallel fashion. These were driven across the physis to engage the lateral cortex of the tibia. The tips were left protruding and were removed 3 weeks post-surgery (Fig. 3). The patient was placed in a short leg splint for 3 weeks, then changed to a controlled ankle movement boot and allowed onto weight-bearing as tolerated at 6 weeks.
Talus fractures are uncommon, making up less than one percent of all fractures [4]. Fractures of the talar body are typically caused by anterior subluxation of the talus relative to the tibia with simultaneous axial load [5].
The scarcity of pediatric talus injuries is likely due to the cartilaginous nature of the talus in growing children, allowing it to absorb greater stress [6], the talus has been reported to require twice the force to fracture when compared to the other tarsal bones [7]. In a comparison of talus fractures of children younger than 12 years and those of adolescents older than 12 years, adolescents were shown to present with more severe fractures compared with children [8]. Talus fractures are usually high-energy injuries and are often associated with polytraumatized patients [1], as in this case.
This patient had a significantly displaced fracture/dislocation [9], requiring open reduction and internal fixation to restore ankle and subtalar joint congruity. Talar dislocations require an even greater force and are likely coupled with comminuted fractures, leading to displacement.
The medial malleolar osteotomy was indicated in concordance with the anteromedial incision to extend the field of view [10] and gain access to the fractured talus [11]. Since the talar body was both dislocated posteriorly and had a posterior fracture line, the osteotomy of medial malleolus was necessary to gain access to reduce the fracture and place rigid fixation. Otherwise, the fracture would have been impossible to repair due to the posterior location of the fracture lines and the trajectory required for screw fixation.
This patient case describes a relatively rare injury to the talar body in an 11-year-old female with multitraumas. The location of the talus fracture required a medial malleolar osteotomy to facilitate exposure and reduction, which was fixed with temporary smooth K-wires. We were unable to identify previous description of this technique in the literature.
To the best of our knowledge, this is the first publication describing this technique in an adolescent with a talus fracture. In a case, where the talar body was both dislocated posteriorly and had a posterior fracture line, the osteotomy of medial malleolus was necessary to gain access to reduce the fracture and place rigid fixation resulting with a successful outcome.
References
- 1.Sundararajan SR, Badurudeen AA, Ramakanth R, Rajasekaran S. Management of Talar Body Fractures. Indian J Orthop. 2018;52(3):258-68. [Google Scholar | PubMed]
- 2.Michel-Traverso A, Ngo TH, Bruyere C, Saglini M. Talus fracture in a 4-year-old child. BMJ Case Rep. 2017;2017. [Google Scholar | PubMed]
- 3.Ziran BH, Abidi NA, Scheel MJ. Medial malleolar osteotomy for exposure of complex talar body fractures. J Orthop Trauma. 2001;15(7):513-8. [Google Scholar | PubMed]
- 4.Byrne AM, Stephens M. Paediatric talus fracture. BMJ Case Rep. 2012;2012. [Google Scholar | PubMed]
- 5.Rockwood CA, Green DP, Bucholz RW. Rockwood and Green's fractures in adults. 3rd ed. Philadelphia: Lippincott; 1991. 2182 p. [Google Scholar | PubMed]
- 6.Letts RM, Gibeault D. Fractures of the neck of the talus in children. Foot Ankle. 1980;1(2):74-7. [Google Scholar | PubMed]
- 7.Waters PM, Skaggs DL, Flynn JM. Rockwood and Wilkins' Fractures in Children. 9th ed: Lippincott Williams & Wilkins (LWW); 2019. 1260 p. [Google Scholar | PubMed]
- 8.Eberl R, Singer G, Schalamon J, Hausbrandt P, Hoellwarth ME. Fractures of the talus--differences between children and adolescents. J Trauma. 2010;68(1):126-30. [Google Scholar | PubMed]
- 9.Smith JT, Curtis TA, Spencer S, Kasser JR, Mahan ST. Complications of talus fractures in children. Journal of pediatric orthopedics. 2010;30(8):779-84. [Google Scholar | PubMed]
- 10.Rammelt S, Godoy-Santos AL, Schneiders W, Fitze G, Zwipp H. Foot and ankle fractures during childhood: review of the literature and scientific evidence for appropriate treatment. Revista Brasileira de Ortopedia. 2016;51:630-9. [Google Scholar | PubMed]
- 11.van Bergen CJA, Tuijthof GJM, Sierevelt IN, van Dijk CN. Direction of the oblique medial malleolar osteotomy for exposure of the talus. Archives of orthopaedic and trauma surgery. 2011;131(7):893-901. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2016 A Case Report of Curettage and Kryptonite® use in Proximal Femur Intraosseous Lipoma
April 10, 2016 A Case Report of Curettage and Kryptonite® use in Proximal Femur Intraosseous Lipoma September 1, 2025 Effect of Teriparatide in Fracture Healing in Elderly
September 1, 2025 Effect of Teriparatide in Fracture Healing in Elderly January 10, 2018 Acquired Flat-foot in a Child (Report of a Case)
January 10, 2018 Acquired Flat-foot in a Child (Report of a Case) March 6, 2019 Popliteal Artery Pseudoaneurysm after Closing Wedge High Tibial Osteotomy
March 6, 2019 Popliteal Artery Pseudoaneurysm after Closing Wedge High Tibial Osteotomy