
Management of open Bosworth fracture is challenging. Early diagnosis and treatment play a key role in limb salvage.
Dr. Aayush Arora, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Belgaum, Karnataka, India. E-mail: ayush.arora52@gmail.com
Introduction:The Bosworth fracture is a distal fibula oblique fracture with proximal fibula posterior dislocation behind the posterior tibia tubercle. Extreme external rotation of the supinated foot causes it. These types of fractures and their treatment are infrequently described in the literatures.
Case Report:A 72 -year-old female pillion rider on a two-wheeler had a Road traffic accident. The patient arrived at the emergency room with a Bosworth fracture along with an open ankle dislocation (Gustilo-Anderson Type 2B). She underwent a staged procedure in form of an external fixator and later on definitive fixation in the form of ankle fusion with retrograde nailing. Since there is very little information regarding treatment modality for an open Bosworth fracture with an ankle dislocation, this case report is very rare. Fracture united well within 8 weeks.
Conclusion: These fractures in elderly patients with comorbidities if poorly managed can lead to severe consequences like an amputation. Awareness of these fractures patterns and their treatment can play a potential role in limb salvage.
Keywords: Bosworth fracture, ankle fusion, retrograde nailing, amputation, limb salvage, diabetic patient.
Bosworth published a study in 1947 describing five cases of an irregular ankle fracture-dislocation in which closed reduction failed to produce adequate results. On open exposure, a situation was discovered that had never been documented before, to the author’s knowledge [1]. Bosworth and Simonovich were the first to examine the mechanism of injury in the Bosworth lesion [2]. Perry et al. defined the latest widely accepted mechanism based on cadaver experiments. The capsule’s anteromedial region was ruptured first, followed by the interosseous ligament. The interosseous membrane tore 4–6 cm above the ankle mortise. As external rotation persisted, the fibula was dragged posteriorly by the ankle’s uninjured lateral collateral ligament and became entangled at the back of the posterolateral border of the tibia. The rotation of the talus over the preserved medial malleoli as well as deltoid ligament resulted in the fibula fracture in a supination-external rotation pattern. The final step of the injury is tearing of the deltoid ligament or medial malleolus fracture [3].
The aim of the treatment is to hold the foot in plantar flexion, correct the deformity of foot, restore bony stability, and avoid skin necrosis. The role of Intramedullary fixation for cases of ankle arthrodesis had been identified as providing rigid fixation, least soft tissue damage, correction of the deformity, decreased vascular disturbance, and an improved functional outcome [4]. In old age patients with articular ankle fractures, tibiotalar calcaneal nailing was an appropriate treatment choice, allowing early weight-bearing and decrease incidence of complication [5]. This case highlights the role of ankle fusion in cases of acute trauma.
A 72-year-old female, a housewife by occupation, belong to the state of Karnataka, known case of hypertension and type 1 diabetes mellitus with poor glycemic control was brought to the department of trauma and had chief complaints of pain, deformity, and open wound (Gustilo-Anderson Type 2B) was present over the medial malleolus of the tibia. The patient was unable to bear weight after the trauma. No neurovascular injury was present. On examination, there was tenderness present over the ankle joint, range of motion was painfull and restricted. An open wound of 5 × 5 cm was present over the medial malleolus of the tibia. X-ray showing a Bosworth fracture with tibiotalar dislocation (Fig. 1).
A closed reduction was performed, with the ankle being pulled anteriorly along with traction and foot in dorsiflexion. After an unsuccessful attempt the patient was taken to operation theatre under spinal anaesthesia, ankle joint was reduced with traction, and ankle spanning external fixator was applied along with debridement of the open wound and primary closure (Fig. 2).
Post-operatively infection was present over the medial sutured wound. The culture was sent and antibiotics started according to the culture sensitivity. A second procedure was performed after 10 days of the first surgery in the form of debridement along with vacuum-assisted closure dressing of the right ankle joint (Fig. 3).  Once the infection was settled, definitive fixation was planned. Transfibular osteotomy was performed through a lateral approach. The ankle joint’s articular cartilage was removed; the surface of the dome to the talus and tibial pilon were smoothened. Articular cartilage was detached from the subtalar joint. A stab incision (4 cm) was made over the plantar aspect of the foot. After separating the fascia, guidewire was passed through the calcaneus, subtalar and ankle joint upto the medullary canal of the tibia under fluoroscopic guidance. Hindfoot must be aligned with the tibia, and the ankle must be in favourable varus/valgus alignment. The guide pin must be placed centrally in the hindfoot and tibia medullary canal. After that, a cannulated drill was used to enter the medullary canal. The canal was reamed up to the desired height and diameter using adjustable reamers, as measured during preoperative preparation. The intramedullary nail attached to the jig was then pushed distal to proximal (retrograde) from the calcaneus, subtalar and via ankle joints, into the medullary canal of the tibia. Calcaneus was locked distally in a dynamic mode, allowing compression at the ankle joint with axial forces and weight-bearing. One screw was passed through the fibula into the talus. Proximal locking was done with one static and one dynamic screw (Fig. 4). The limb was kept elevated in a BB splint.
Once the infection was settled, definitive fixation was planned. Transfibular osteotomy was performed through a lateral approach. The ankle joint’s articular cartilage was removed; the surface of the dome to the talus and tibial pilon were smoothened. Articular cartilage was detached from the subtalar joint. A stab incision (4 cm) was made over the plantar aspect of the foot. After separating the fascia, guidewire was passed through the calcaneus, subtalar and ankle joint upto the medullary canal of the tibia under fluoroscopic guidance. Hindfoot must be aligned with the tibia, and the ankle must be in favourable varus/valgus alignment. The guide pin must be placed centrally in the hindfoot and tibia medullary canal. After that, a cannulated drill was used to enter the medullary canal. The canal was reamed up to the desired height and diameter using adjustable reamers, as measured during preoperative preparation. The intramedullary nail attached to the jig was then pushed distal to proximal (retrograde) from the calcaneus, subtalar and via ankle joints, into the medullary canal of the tibia. Calcaneus was locked distally in a dynamic mode, allowing compression at the ankle joint with axial forces and weight-bearing. One screw was passed through the fibula into the talus. Proximal locking was done with one static and one dynamic screw (Fig. 4). The limb was kept elevated in a BB splint.
Limb Elevation, ice packs, and medication were given to reduce pain and swelling. Hip and knee active range of motion, hip strengthening and upper extremity strengthening were started on day 2. The patient was allowed non-weight-bearing walking day 2 onwards with the help of a walker. Non-weight-bearing walking was advised for 6 weeks. After 6 weeks full weight-bearing using walking aid (Fig. 5).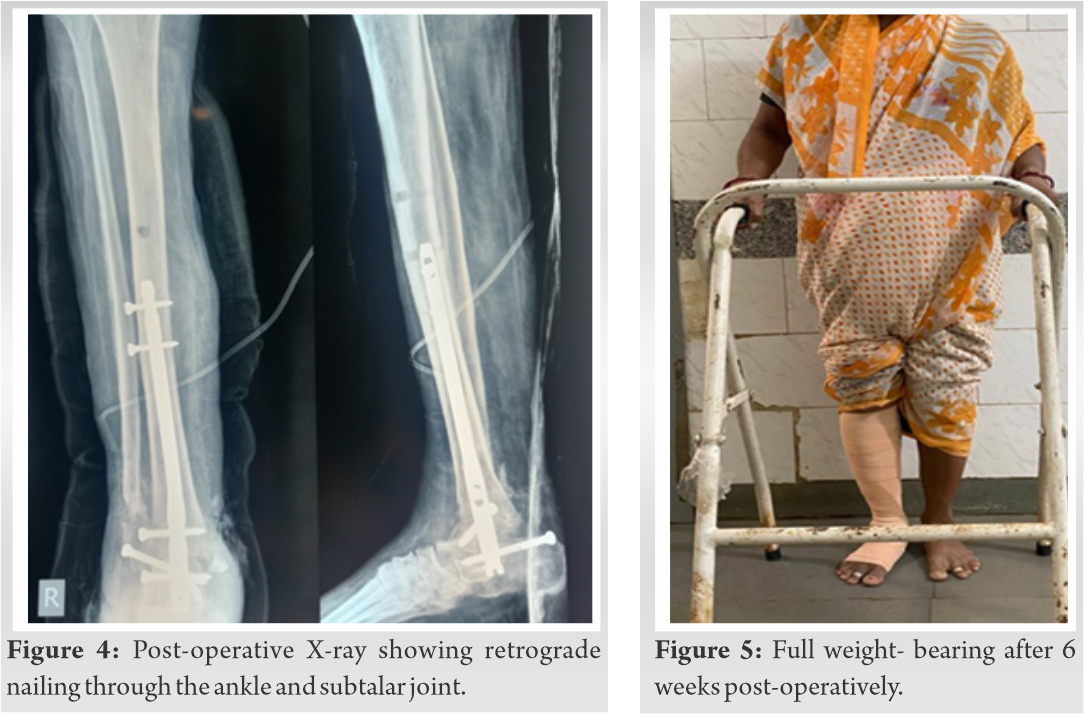
Until recently, tibiotalocalcaneal arthrodesis had been published infrequently, with generally promising outcomes [6]. There is a high risk of damage to the various structures around the ankle including the skin, plantar aponeurosis of the foot, muscles of plantar aspect, tendons, as well as neurovascular structures. Pochatko and his colleagues showed six zones injuring the plantar structures on cadaver specimens while passing an intramedullary nail (retrogradely). The location of the nail was placed central pre-requisite that the nail passed through the calcaneum at the zone between sustentaculum tali and calcaneum body [7]. Fusion of subtalar joint along with ankle joint is a drawback of retrograde nailing. Dorsiflexion is reduced by 50% and plantarflexion is reduced by 70% after an ankle fusion, with Chopart and Lisfranc joints exhibiting residual motion [8]. In cases where the subtalar joint is fused, it becomes mandatory to position the joint in mild degree of eversion. Intramedullary implants have a higher biomechanically stability for achieving union when compared with compression screws in terms of fixation. Early weight-bearing is also possible with intramedullary nail fixation, which is essential in this community of patients [10].
The optimum management for the Bosworth type of fracture along with ankle dislocation is undetermined. In elderly patients with open injury and comorbidities, ankle fusion with retrograde nailing gives a better option in terms of fusion rate and early mobilization.
Bosworth fracture with ankle dislocation is a rare presentation for which early diagnosis and management play a key role in limb salvage.
References
- 1.Bosworth DM. Fracture-dislocation of the ankle with fixed displacement of the fibula behind the tibia. J Bone Joint Surg Am 1947;29:130-5. [Google Scholar]
- 2.Harris RI. Discussion (of Bosworth paper). J Bone Joint Surg 1947;29:135. [Google Scholar]
- 3.Perry CR, Rice S, Rao A, Burdge R. Posterior fracture-dislocation of the distal part of the fibula. Mechanism and staging of injury. J Bone Joint Surg Am 1983;65:1149-57. [Google Scholar]
- 4.Oesman I, Asdi AR. Calcaneotalotibial arthrodesis by retrograde intramedullary nailing using expert tibia nail for charcot osteoneuropathy of the foot: A case series. Int J Surg Case Rep 2019;57:9-14. [Google Scholar]
- 5.Tarkin IS, Fourman MS. Retrograde hindfoot nailing for acute trauma. Curr Rev Musculoskelet Med 2018;11:439-44. [Google Scholar]
- 6.Kitaoka HB, Anderson PJ, Morrey BF. Revision of ankle arthrodesis with external fixation for non-union. J Bone Joint Surg Am 1992;74:1191-200. [Google Scholar]
- 7.Pochatko DJ, Smith JW, Phillips RA, Prince BD, Hedrick MR. Anatomic structures at risk: Combined subtalar and ankle arthrodesis with a retrograde intramedullary rod. Foot Ankle Int 1995;16:542-7. [Google Scholar]
- 8.Mann R. Arthrodesis of the foot and ankle. In: Surgery of the Foot and Ankle. 6th ed. United States: Mosby; 1993. [Google Scholar]
- 9.Beaudoin A, Fiore S, Krause W, Adelaar R. Effect of isolated talocalcaneal fusion on contact in the ankle and talonavicular joints. Foot Ankle 1991;12:12-25. [Google Scholar]
- 10.Anderson T, Linder L, Rydholm U, Montgomery F, Besjakov J, Carlsson A. Tibio-talocalcaneal arthrodesis as a primary procedure using a retrograde intramedullary nail: A retrospective study of 26 patients with rheumatoid arthritis. Acta Orthop 2005;76:580-7. [Google Scholar]






