It is necessary to take measures such as bone grafting and select a stem as long as possible when a narrow medullary cavity requires the use of a narrow long stem with a distal locking screw.
Dr. Shun Igarashi, Department of Orthopedic Surgery, Akita University Graduate School of Medicine, 1-1-1 Hondo, Akita 010-8543, Japan. E-mail: s.igarashi0422@med.akita-u.ac.jp
Introduction:Fractures around the femoral stem are difficult complications to treat. In revision surgery, good results can be obtained by a long cementless stem with a distal locking screw. However, there are few reports of treatment for cases where the stem itself is broken.
Case Report:The case of a 69-year-old woman in which the femoral stem that was broken 5 years after performing revision surgery for a right periprosthetic femoral fracture was repaired using a solid long stem with a distal locking screw is presented. Her past history included osteoporosis and rheumatoid arthritis. She fell due to sudden right thigh pain and was then taken to the emergency department of our hospital. X-ray examination showed breakage of the stem itself at the position of the distal locking screw hole closest to the previous fracture. Revision total hip arthroplasty using a larger diameter stem of the same model was performed. The previous fracture site had been a fibrous non-union, and the femur proximal to the previous fracture site had severe atrophy and bone loss due to stress shielding. Two years after surgery, the patient can walk without pain, and progression of stress shielding, loosening of the stem, and breakage of the implants have not occurred.
Conclusion: n the present case, non-union, proximal bone atrophy, the location of the hole of the distal locking screw, and insufficient stem strength were the causes of stem breakage. It is necessary to take measures such as bone grafting and select a stem as long as possible for the position of the distal locking screw to be as far as possible from the fracture line when using a narrow long stem with a distal locking screw.
Keywords: Periprosthetic femoral fractures, revision hip arthroplasty, stem fracture.
In recent years, total hip replacement (THR) and femoral head replacement (FHR) have increased with the improvement of clinical results and the increase of the elderly population, but the complications are also increasing at the same time. Of the complications after THR or FHR, fractures around the femoral stem are difficult to treat, and their number may increase in the future. In general, revision surgery is selected for periprosthetic femoral fractures with loosened stems [1]. In revision surgery especially for elderly people, good results can be obtained by a long cementless stem with a distal locking screw that can help the patients walk immediately without waiting for bone union [2, 3, 4]. However, even if a long stem with a distal locking screw is used to treat a periprosthetic fracture, and the patients can walk immediately after the operation, the implant will be over-stressed and break when bone union cannot be obtained. In fact, there are few such reports, and thus the treatment for cases where the stem itself is broken has not been established. In particular, there have been no reports of breakage of solid long stems with distal locking screws that reduce the risk of breakage, though there are a few reports of the breakage of the hollow inside the long stem (Cannulok, Teijin Nakashima Medical Co., Ltd., Okayama, Japan) [5]. Therefore, a case in which the stem was broken 5 years after revision surgery using a solid long stem with a distal locking screw is presented.
A 69-year-old woman with osteoporosis and rheumatoid arthritis complained of sudden right thigh pain, after which she was unable to walk and was referred to our orthopedic department. She has been taking alendronate for more than 10 years for osteoporosis. Her stage of rheumatoid arthritis was Steinbrocker classification Stage IV [6], and she was treated with bucillamine, tacrolimus, prednisolone, and abatacept by a rheumatologist.
In 2006, she complained of groin pain and was treated using cemented total hip arthroplasty for severe rheumatoid arthritis of the right hip (Fig. 1). She fell in 2013 and suffered a right periprosthetic femoral fracture (Vancouver classification Type C [1]) (Fig. 2). As a result, she underwent revision arthroplasty with a solid long cementless stem with a distal locking screw (Delta-LOCK stem 11-mm diameter, Teijin Nakashima Medical Co., Ltd.) (Fig. 3).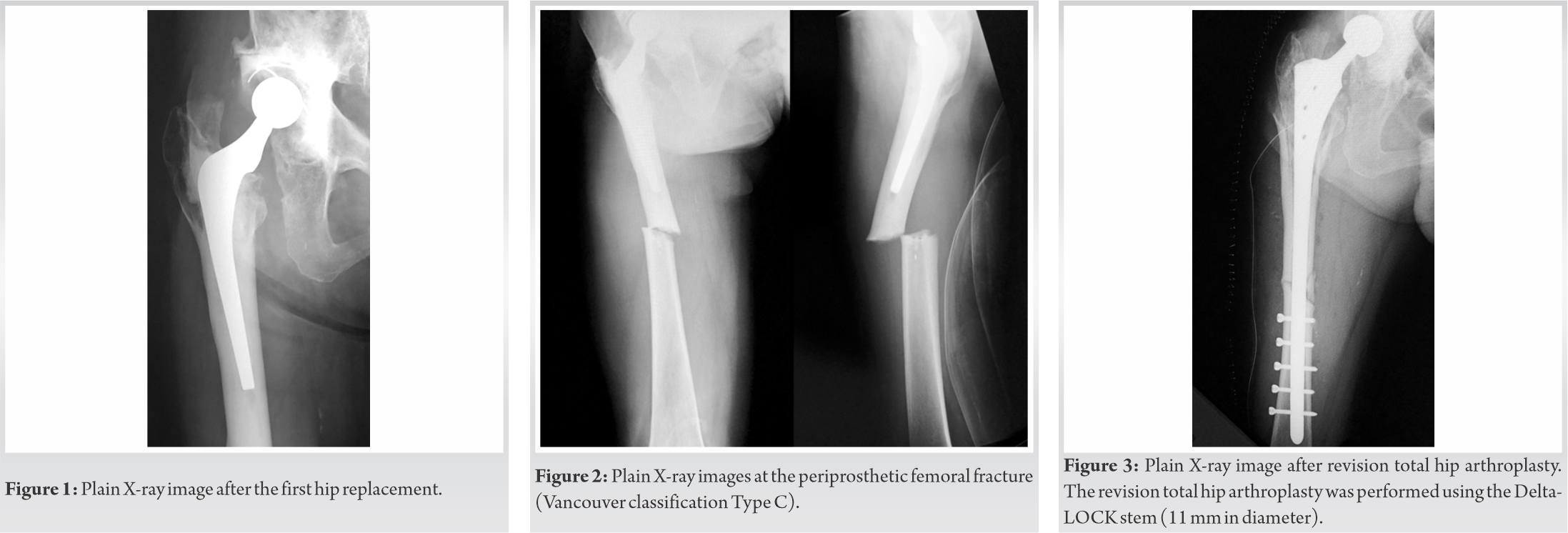 After the revision of the right hip prosthesis, bone union was not found at the fracture site, but she was able to walk without pain.
After the revision of the right hip prosthesis, bone union was not found at the fracture site, but she was able to walk without pain.
However, she fell due to sudden right thigh pain and was then taken to the emergency department of our hospital in 2018. X-ray examination showed breakage of the stem itself at the position of the distal locking screw hole closest to the previous fracture (Fig. 4).
Therefore, the broken 11-mm-diameter stem was removed, and revision total hip arthroplasty was performed using a 15-mm-diameter stem of the same model (Fig. 5). The previous fracture site had been a fibrous non-union. The femur proximal to the previous fracture site had severe atrophy and bone loss due to stress shielding. The cause of the breakage of the stem was considered to be the lack of bone union, and mechanical stress was concentrated on the stem. The fixation and stability of the new stem during surgery were good, so the bone atrophy site and bone defect sites were filled with bone cement, and no bone grafting was performed.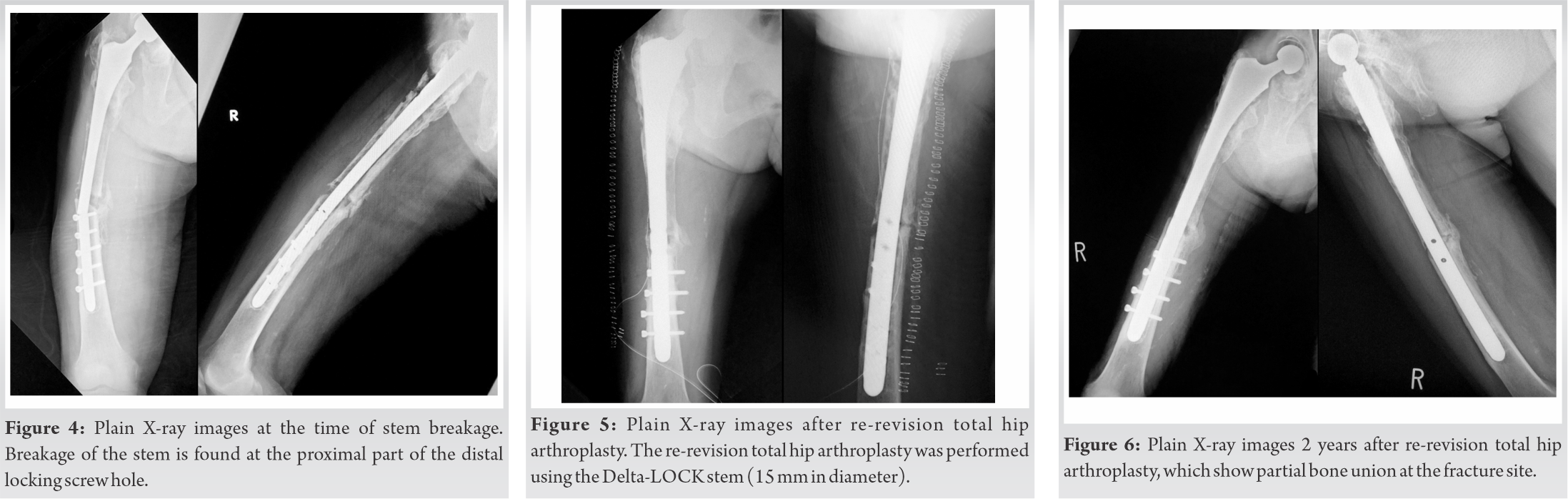
The patient was allowed to walk immediately after the operation, and she was discharged from the hospital 3 weeks after the operation.
Oral administration of alendronate was discontinued after hospitalization, and teriparatide injection was started. Two years after surgery, the patient can walk without pain, and progression of stress shielding, loosening of the stem, and breakage of the stem and screw have not occurred (Fig. 6).
In general, the breakage of implants such as femoral stems or intramedullary nails is a result of local stress concentration on the implants and metal fatigue due to various factors. The main causes of breakage of intramedullary nails are delayed bone union/non-union, surgical technique, improper weight-bearing, and implant quality [7, 8]. The factors that cause the femoral stem to break include varus alignment installation, poor fixation, loosening, cementing technique, and material strength [9, 10]. In the present case, non-union, proximal bone atrophy with a bone defect, and insufficient stem strength (stem diameter was only 11 mm) were the causes of stem breakage.
A common site of intramedullary nail breakage is the distal portion of the nail, particularly the distal locking screw hole closest to the fracture site [11]. There is a particularly high risk of breakage of the nail when the screw hole is located <5 cm of the fracture site [12]. In addition, there have been reports of breakage of the stem in cases of cementless stems with extensive bone atrophy and bone defects in the proximal region and in cases of stems with a diameter of ≤13.5 mm [13]. Therefore, the use of larger diameter stems in combination with bone grafts may be considered.
In the case of cemented stems, breakage of the stem is caused by poor fixation at the proximal part of the stem due to bone defects and insufficient cement filling [10]. If the proximal part of the stem is poorly fixed while the distal part is well fixed, cantilever action may be added, and the risk of breakage may be further increased [14].
In the first revision surgery (revision surgery for periprosthetic fracture) in the present case, bone grafting was not performed because of the absence of a bone defect and bone atrophy. However, the progression of bone atrophy due to postoperative stress shielding led to a relative shortage of stem diameter. The deterioration of bone quality due to comorbidities (osteoporosis and rheumatoid arthritis) and pseudoarthrosis contributed to this. Furthermore, the proximal part had bone atrophy and stem loosening, whereas the distal part had multiple locking screws inserted; thus, the repeated cantilever effect caused breakage of the stem in the present case. Another possible cause is that the distal locking screw was inserted near the fracture site (<5 cm).
At the time of the second revision surgery, it was feared that the fixation would be insufficient due to the nonunion and the bone defect in the proximal part. However, second revision surgery was performed using the same type of stem with a maximum diameter of 15 mm, and good fixation was obtained. In addition, cement infilling for the bone defect site in the proximal part decreased the instability between the proximal bone and the stem. However, bone union was not expected at the nonunion site. In other words, it was expected that using as thick a nail as possible would prolong the time to re-breakage of the stem. If re-breakage occurs, the same stem will be used, or total femoral replacement will be performed.
However, it has been reported that the stress on the stem can be dispersed using a strut allograft from the fibula for revision surgery of periprosthetic fractures [13]. In the present case, it may have been necessary to aggressively perform autologous bone transplantation from the time of the first revision surgery. Furthermore, it may be possible to prevent stem breakage by taking measures to promote bone union if delayed union is observed.
It is thought that the possibility of stem breakage will be considerably decreased if the material is solid with a diameter of about 15 mm, because more than 2 years have passed since the last operation, and breakage of the stem has not recurred. However, it is necessary to take measures such as bone grafting and select a stem as long as possible for the position of the distal locking screw to be as far as possible from the fracture line when a narrow medullary cavity requires the use of a narrow long stem with a distal locking screw.
In the case of revision surgery using a long cementless stem with a distal locking screw, it is thought that the possibility of stem breakage will be considerably decreased if the material is solid with a diameter of about 15 mm. However, it is necessary to take measures such as bone grafting and select a stem as long as possible when a narrow medullary cavity requires the use of a narrow long stem with a distal locking screw.
References
- 1.Brady OH, Garbuz DS, Masri BA, Duncan CP. The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty 2000;15:59-62. [Google Scholar]
- 2.Patrice M, Remy P, Philippe R, Henri M, Jacques T, Denis V. Distal locking stem for revision femoral loosening and peri-prosthetic fractures. Int Orthop 2011;35:275-82. [Google Scholar]
- 3.Kamada T, Imai H, Mashima N, Takeba J, Okumura H, Miura H. Long term results with the interlocking uncemented long stem in revision hip arthroplasty: A mean 15-year follow-up. J Arthroplasty 2015;30:835-9. [Google Scholar]
- 4.El-Bakoury A, Hosny H, Williams M, Keenan J, Yarlagadda R. Management of vancouver B2 and B3 periprosthetic proximal femoral fractures by distal locking femoral stem (cannulok) in patients 75 years and older. J Arthroplast 2017;32:541-5. [Google Scholar]
- 5.Matsumura K, Isoya E, Kawasaki T, Kikuchi K, Matsusue Y. A rare case of CANNULOK stem fracture after a fracture of the femoral stem. Japanese J Rheum Joint Surg 2007;26:125-9. [Google Scholar]
- 6.Steinbrocker O, Traeger CH, Batterman RC. Therapeutic criteria in rheumatoid arthritis. J Am Med Assoc 1949;140:659-62. [Google Scholar]
- 7.Ballal MS, Emms N, Ramakrishnan M, Thomas G. Proximal femoral nail failures in extracapsular fractures of the hip. J Orthop Surg (Hong Kong) 2008;16:146-9. [Google Scholar]
- 8.Li GH, Li F, Xia RY, Wang TP, Chen AM. An analysis of failure factors in treatment of femoral shaft fracture with interlocking intramedullary nailing. Zhonghua Wai Ke Za Zhi 2006;44:538-40. [Google Scholar]
- 9.Markolf KL, Amstutz HC. A comparative experimental study of stresses in femoral total hip replacement components: The effects of prosthesis orientation and acrylic fixation. J Biomech 1976;9:73-9. [Google Scholar]
- 10.Wroblewski BM. Fractured Stem in total hip replacement: A clinical review of 120 cases. Acta Orthop Scand 1982;53:279-84. [Google Scholar]
- 11.Bhat AK, Rao SK, Bhaskaranand K. Mechanical failure in intramedullary interlocking nails. J Orthop Surg 2006;14:138-41. [Google Scholar]
- 12.Bucholz RW, Ross SE, Lawrence KL. Fatigue fracture of the interlocking nail in the treatment of fracture of the distal part of the femoral shaft. J Bone Joint Surg 1987;169:1391-9. [Google Scholar]
- 13.Busch CA, Charles MN, Haydon CM, Bourne RB, Rorabeck CH, Macdonald SJ, et al. Fractures of distally-fixed femoral stems after revision arthroplasty. J Bone Joint Surg Br 2005;87:1333-6. [Google Scholar]
- 14.Woolson ST, Milbauer JP, Bobyn JD, Yue S, Maloney WJ. Fatigue fracture of a forged cobalt-chromium-molybdenum femoral component inserted with cement: A report of ten cases. J Bone Joint Surg Am 1997;79:1842-8. [Google Scholar]