
In displaced coracoid fracture, surgical management is better option than non operative treatment to achieve early functional recovery of the limb and promising radiological union.
Dr. Gokul Anand Murugesan, Department of Orthopaedic Surgery, Aarupadai Veedu Medical College, Pondicherry, India. E-mail: mganand97@gmail.com
Abstract
Introduction: Isolated coracoid process fracture of scapula is a rare. Usually, it happens along with the rotator cuff tear, dislocation of acromioclavicular joint, or glenohumeral joint. Displaced fracture will cause impairment of upper limb movement. Since there are very low numbers of cases reported so far, the treatment is still controversial.
Case Report: We report a case of a 42-year-old male laborer with motor vehicle accident, following which he had pain and restricted movements on his left shoulder. On examination, Glasgow Coma Scale 15/15 and left shoulder had swelling and tenderness at mid-third clavicle. Range of motion (ROM) is painful and restricted. Plain radiograph shows suspected fracture at coracoid process and computerized tomography scan confirms displaced isolated coracoid process fracture. He underwent open reduction with internal fixation with a 4 mm cannulated cancellous screw with washer. Following surgery, initial 2 weeks shoulder immobilized in arm sling and gradual pendulum exercise was started as pain tolerable. At the end of 6 weeks, radiological investigation showed fracture united and he was advised to do ROM exercise and restricted activity of daily living. At the end of 3 months, he was able to do his normal activity of daily living as before injury. The patient followed up to 6 months and had full range of movements in all directions and there was no pain and he was able to do daily activities.
Conclusion: In this case of isolated coracoid fracture was found displaced more than 1 cm, hence we preferred open reduction and internal fixation with 4 mm cannulated cancellous screw with washer to avoid non-union.
Keywords: Isolated coracoid fracture, rotator cuff tear, scapula fracture.
It is uncommon to have an isolated coracoid process fracture of the scapula. Coracoid process fractures account for around 1% of all fractures and 2–13% of scapula fractures. Usually, it happens along with the rotator cuff tear, dislocation of acromioclavicular joint, or glenohumeral joint [1,2]. Displaced fracture will cause impairment of upper limb function. Since there are very low number of cases reported so far, the treatment is still controversial [3,4,5]. In our case, a 42-year-old male came with the complaints of the left shoulder pain and tenderness after he met with a motor vehicle accident. He was advised to take radiography and computerized tomography (CT) scan as an isolated coracoid process fracture was diagnosed which was treated surgically.
A 42-year-old male manual laborer presented at the orthopedics department with the complaints of pain and restricted movement in the left shoulder following a motor vehicle accident. On examination, Glasgow Coma Scale 15/15 and left shoulder had swelling and tenderness at mid-third clavicle. Range of motion (ROM) is painful and restricted. Neurovascular examinations were normal. On plain radiograph (Fig. 1) shows suspected isolated coracoid fracture and CT (Fig. 2) confirms displaced isolated coracoid process fracture.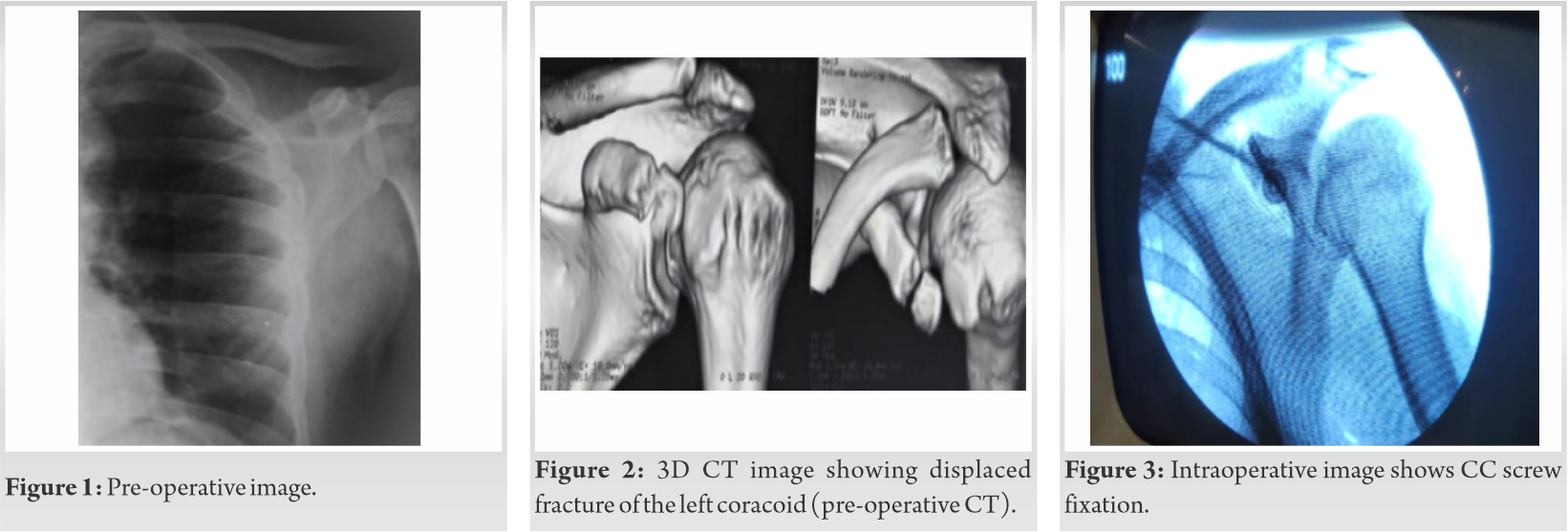 Since the fracture was displaced >1 cm, to avoid non-union and weakness of the left upper limb, the patient was advised to undergo surgical fixation, pre-anesthetic fitness was obtained. Prophylactic intravenous antibiotics given at the time of anesthesia. Under antiseptic precaution, under supraclavicular block, the patient in beach chair position 5 cm incision made over coracoid process and the fracture site exposed and coracoid process found displaced. Fracture ends freshened and coracoid process reduced over its base and temporary fixed with K-wire. Under C-arm fractured reduction and K-wire position confirmed and length of screw measured indirectly. Using 3.2 mm cannulated drill, bit fracture fragments drilled and 4 mm × 22 mm cannulated screw with washer used to fix the fracture and position of screw and stability of fixation confirmed with C-arm. Postoperatively, further, two doses of intravenous antibiotic given. Wound inspected and dressed regularly.
Since the fracture was displaced >1 cm, to avoid non-union and weakness of the left upper limb, the patient was advised to undergo surgical fixation, pre-anesthetic fitness was obtained. Prophylactic intravenous antibiotics given at the time of anesthesia. Under antiseptic precaution, under supraclavicular block, the patient in beach chair position 5 cm incision made over coracoid process and the fracture site exposed and coracoid process found displaced. Fracture ends freshened and coracoid process reduced over its base and temporary fixed with K-wire. Under C-arm fractured reduction and K-wire position confirmed and length of screw measured indirectly. Using 3.2 mm cannulated drill, bit fracture fragments drilled and 4 mm × 22 mm cannulated screw with washer used to fix the fracture and position of screw and stability of fixation confirmed with C-arm. Postoperatively, further, two doses of intravenous antibiotic given. Wound inspected and dressed regularly.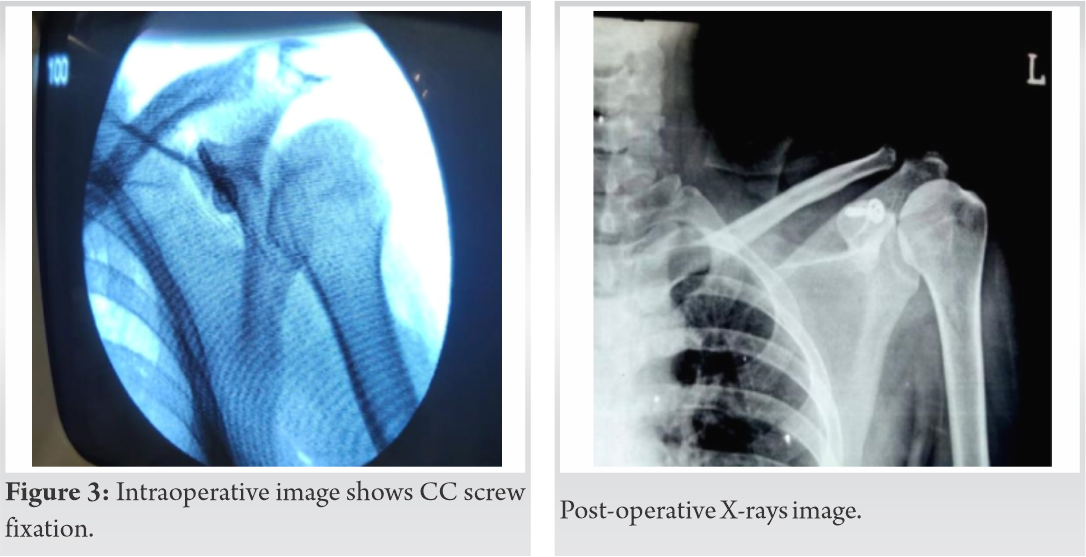 Suture was removed at the end of 2nd week. Initial 2 weeks shoulder immobilized in arm sling and gradual pendulum exercise was started as pain tolerable. At the end of 6 weeks, the patient reviewed found pain free and X-ray shows implant in situ and CT scan confirms implant position and fracture union. The patient advised to do active ROM as pain tolerable and advised to do restricted activities daily living. At the end of 3 months, he was able to do full ROM and X- ray shows implant in situ and fracture union and the patient advised to do his normal activity of daily living as before injury. At the end of 6 months, the patient reviewed and he had a pain-free full ROM in all directions. X-ray shows implant in situ and fracture union (Fig. 3). He was able to do activities of daily living as before injury (Fig. 4).
Suture was removed at the end of 2nd week. Initial 2 weeks shoulder immobilized in arm sling and gradual pendulum exercise was started as pain tolerable. At the end of 6 weeks, the patient reviewed found pain free and X-ray shows implant in situ and CT scan confirms implant position and fracture union. The patient advised to do active ROM as pain tolerable and advised to do restricted activities daily living. At the end of 3 months, he was able to do full ROM and X- ray shows implant in situ and fracture union and the patient advised to do his normal activity of daily living as before injury. At the end of 6 months, the patient reviewed and he had a pain-free full ROM in all directions. X-ray shows implant in situ and fracture union (Fig. 3). He was able to do activities of daily living as before injury (Fig. 4).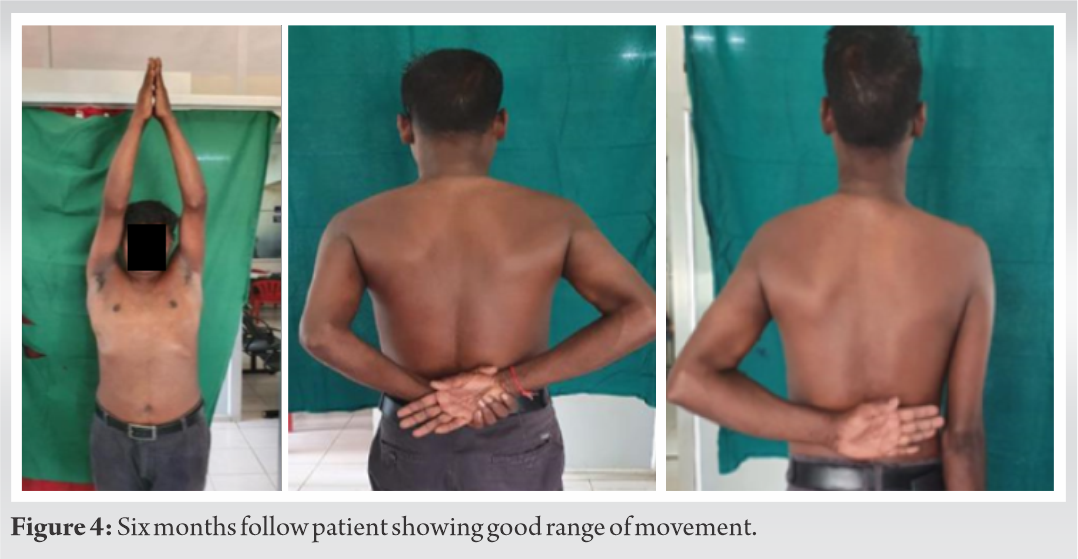
Coracoid fractures have been described as rare injuries; however, there has lately been an increase in the number of occurrences. The incidence has ranged between 2% and 13% of all scapular fractures; they account for 1% of all fractures and 5% of shoulder fractures [6]. Fractures at the base of the coracoid process are common, and they are usually little displaced and associated with acromioclavicular joint injuries. Painful non-union and >1 cm displacement on the coracoid process were acknowledged as indications for surgical therapy. There are no hard and fast rules when it comes to the best way to treat coracoids process fractures. The vast majority of non-displaced fractures are dealt with conservatively. The majority of prior research on this topic were in the form of case reports or small case series, with no definitive conclusion of the optimal treatment approach.
Vaienti and Pogliacomi in a series of nine cases with delayed diagnosis applied conservative treatment, and however, outcome was poor [7].
Anavian et al., in case study, 26 patients taken including scapula fractures. Out of which isolated coracoid process fracture, 14 case surgeries were applied and successful result was obtained for all patients. Other 12 patients treated conservatively [8].
Spormann et al. successfully operated on three instances of isolated coracoid process fractures treated with CC screws. Subramanian et al. reported surgical treatment of an isolated coracoid fracture in an unstable shoulder yielded satisfactory outcomes once more [9,10].
Archik et al., an isolated displaced coracoid process fracture treated with open reduction and internal fixation and discussed in young athletes surgical surgery, may be a useful choice to achieve early use of the limb, excellent radiographic union, and better clinical function [11].
Conservative treatment of coracoid fractures in athletes and patients engaged in hard manual labor was attempted in investigations by Guttentag and Rechtine, but unsatisfactory outcomes were found in such cases [12].
Surgery was selected in the current case of an isolated coracoid process fracture with >1 cm displacement and a patient engaged in intensive manual labor to avoid non-union due to the action of forces around the coracoid. Despite the fact that this is an uncommon fracture, surgical care is preferable.
Isolated coracoid fracture is an uncommon condition that impairs upper limb function. A CT scan can provide a more accurate diagnosis. In our case study, surgery was selected to avoid non-union of the coracoid process fracture due to the isolated coracoid process fracture displaying displacement >1 cm and he involved in hard manual work. In our instance, fracture union was achieved after 6 weeks of fixation with a CC screw, and he returned to his pre-injury activities after 3 months. For displaced coracoid process fractures, we choose open reduction and internal fixation with a CC screw.
Isolated coracoid process fracture showing displacement >1 cm and he engaged in heavy manual work, surgery was preferred to avoid non-union and impairment of upper limb function. We prefer open reduction and internal fixation with CC screw for displaced coracoid process fracture.
References
- 1.Petty OH. Fracture of the coracoid process of the scapula caused bymuscula action. Ann Surg 1907;45:427-30. Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17-9. [Google Scholar | PubMed]
- 2.McGinnis M, Denton JR. Fractures of the scapula: A retrospective study of 40 fractured scapulae. J Trauma 1989;29:1488-93. [Google Scholar | PubMed]
- 3.Ogawa K, Inokuchi S, Matsui K. Fracture of the coracoid process. Act Orthop Scand 1990;61:7-8. [Google Scholar | PubMed]
- 4.Eyres KS, Brooks A, Stanley D. Fractures of the coracoid process. J Bone Joint Surg Br 1995;77:425-8. [Google Scholar | PubMed]
- 5.Fery A, Sommelet J. Fracture of the coracoid process (author’s transl). Rev Chir Orthop Reparatrice Appar Mot 1979;65:403-7. [Google Scholar | PubMed]
- 6.Ada JR, Miller ME. Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-80. [Google Scholar | PubMed]
- 7.Vaienti E, Pogliacomi F. Delayed diagnosis of isolated coracoid process fractures: Results of 9 cases treated conservatively. Acta Biomed 2012;83:138-46. [Google Scholar | PubMed]
- 8.Anavian J, Wijdicks CA, Schroder LK, Vang S, Cole P. Surgery for scapula process fractures: Good outcome in 26 patients. Acta Orthop 2009;80:344-50. [Google Scholar | PubMed]
- 9.Spormann C, Holzach P, Ryf C. Open reduction and internal fixation of isolated fractures of the coracoid-process-presentation of three cases and review of the literature. Swiss Surg 1998;4:198-202. [Google Scholar | PubMed]
- 10.Subramanian AS, Khalik MA, Shah MM. Isolated fracture of the coracoid process associated with unstable shoulder. ANZ J Surg 2007;77:188-9. [Google Scholar | PubMed]
- 11.Archik S, Nanda SN, Tripathi S, Choudhari A, Rajadhyaksha H. An isolated displaced fracture of the coracoid process treated with open reduction and internal fixation-a case report and review of literature. J Orthop Case Rep 2016;6:37-9. [Google Scholar | PubMed]
- 12.Guttentag IJ, Rechtine GR. Fractures of the scapula. A review of the literature. Orthop Rev 1988;17:147-58. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2023 Great Toe Osteoid Osteoma with Atypical Presentation: A Case Report
December 10, 2023 Great Toe Osteoid Osteoma with Atypical Presentation: A Case Report May 9, 2017 Transient Migratory Osteoporosis of the Hip and Talus: A Case Report
May 9, 2017 Transient Migratory Osteoporosis of the Hip and Talus: A Case Report August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients
August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients September 10, 2021 Monteggia Fracture-Dislocation with Associated TFCC Injury and DRUJ Subluxation – A Very Rare Case Report
September 10, 2021 Monteggia Fracture-Dislocation with Associated TFCC Injury and DRUJ Subluxation – A Very Rare Case Report