
Severely comminuted fractures of distal humerus are challenging to treat and multiple cantilever K-wiring can be used as a preferable alternative for fixation.
Dr. Sushmit Singh, Department of Orthopaedics, Dr. D. Y. Patil Medical College and Hospital, Navi Mumbai, Maharashtra, India. E-mail: drsushmits@gmail.com
Abstract
Introduction: Anterior dislocation of the elbow is comparatively less frequent and is often associated with fractures of the distal humerus. Such injuries require surgical intervention at the earliest but with the surge of COVID-19 pandemic and different protocols being followed by surgeons, such cases are getting neglected. We present a 5-week-old neglected anterior dislocation of the right elbow joint with lateral condyle and medial epicondyle humerus fracture and a unique cantilever K-wiring technique used for its treatment.
Case Presentation: A 30-year-old man presented with pain, deformity, and limited range of movement of his right elbow joint and a non-healing wound over the olecranon after he had a road traffic accident 5 weeks back. The patient had been initially treated in a local hospital where he tested positive for COVID-19 and was managed conservatively. Radiographs revealed lateral condyle and medial epicondyle humerus fracture and an unreduced anterior dislocation of the right elbow joint.
Conclusion: Neglected fracture-dislocation of the elbow is challenging and is further complicated by comminuted fragments with loss of bone stock. A unique use of multiple Kirschner wires in a cantilever fashion provides a good fixation alternative for such cases.
Keywords: Anterior elbow dislocation, neglected elbow injury, cantilever K-wiring.
There have been many challenges faced by the medical and surgical community worldwide after the spread of COVID-19 around the world. The surgical management of patients has also been affected severely and the impact of delay in surgeries can be seen in primary surgical outcomes. With the increasing burden of COVID-19 on the hospitals, cases of conservatively managed fractures and dislocations with adverse outcomes have become more prevalent. Elbow dislocation is a serious injury requiring immediate surgical intervention, especially when neglected and associated with fractures [1]. The goal should be to provide good fixation to the bony fragments with better handling of soft tissues for which any available method can be used by the surgeon. The severity of osseous trauma in combination with soft-tissue damage may affect the function in the elbow region [2]. Here, we present an unusual case of a 5-week-old unreduced anterior dislocation of the elbow joint with medial epicondyle and lateral condyle humerus fracture in a 30-year-old male patient and describe a unique technique for fixation of comminuted articular fragments.
A 30-year-old male presented to us in the outpatient department with the complaints of pain and deformity of the right elbow with a non-healing wound for 5 weeks. The patient had a history of a road traffic accident while driving a two-wheeler, following which he had pain, swelling, and deformity of the right elbow with a wound over the olecranon. He had sought treatment from a local hospital and was tested positive for COVID-19 and was managed conservatively with posterior above elbow slab. After getting treatment for COVID-19, the patient visited our hospital for the persistent deformity and stiffness of the right elbow.
On examination, the right elbow joint had flexion deformity and wasting of muscles of arm and forearm was evident. On palpation, the olecranon process was found to be displaced anteriorly from the olecranon fossa of the right humerus, crepitus could be felt and a non-healing wound was present over the olecranon (3*2 cm). There were no signs of active infection, and therefore, blood culture was not done. The flexion deformity was 30° with further flexion up to 60°. Pronation was restricted at 10° and supination was possible till 40°. On further examination, valgus laxity could be appreciated with no associated neurovascular deficit. On radiographic examination, the right elbow was found to be anteriorly dislocated with medial epicondyle fracture and comminuted lateral condyle fracture (Fig. 1). A computed tomogram (CT) with 3D reconstruction (Fig. 2) confirmed an anterior dislocation of the right elbow joint with the associated distal humerus, lateral sagittal, partial articular, trans-trochlear multi-fragmentary, epiphyseal-metaphyseal lateral condyle fracture, and medial epicondyle fracture (AO/OTA Classification – 13-B1.3).
We planned an open reduction internal fixation with plating as it was an already delayed presentation and was an unreduced fracture dislocation of elbow. Surgery was performed under general anesthesia with intubation. The patient was positioned laterally with the elbow flexed on a sidearm fixed to the table. A pneumatic tourniquet was applied and we performed an open reduction and internal fixation of the elbow by taking a midline posterior approach. The dissection was done in layers and the ulnar nerve was identified and preserved avoiding any kind of traction or pressure injuries. We took a paratricipital approach, and after further dissection and extensive release of fibrous and osteoid tissues, we were successful in relocating the elbow joint. Special care was taken to protect the medial and lateral collateral ligaments which were found to be intact. Any overlapping cartilage was further trimmed to attain bleeding metaphyseal bone. During the exposure, the articular cartilage was carefully handled to preserve it and avoid the nibbling of soft tissues around it. The small articular fragments were preserved and disimpacted with the help of a fine elevator and interposed tissues were removed. After the reduction of all major fragments, multiple Kirschner wires (K-wires) were used for provisional fixation (Fig. 3). 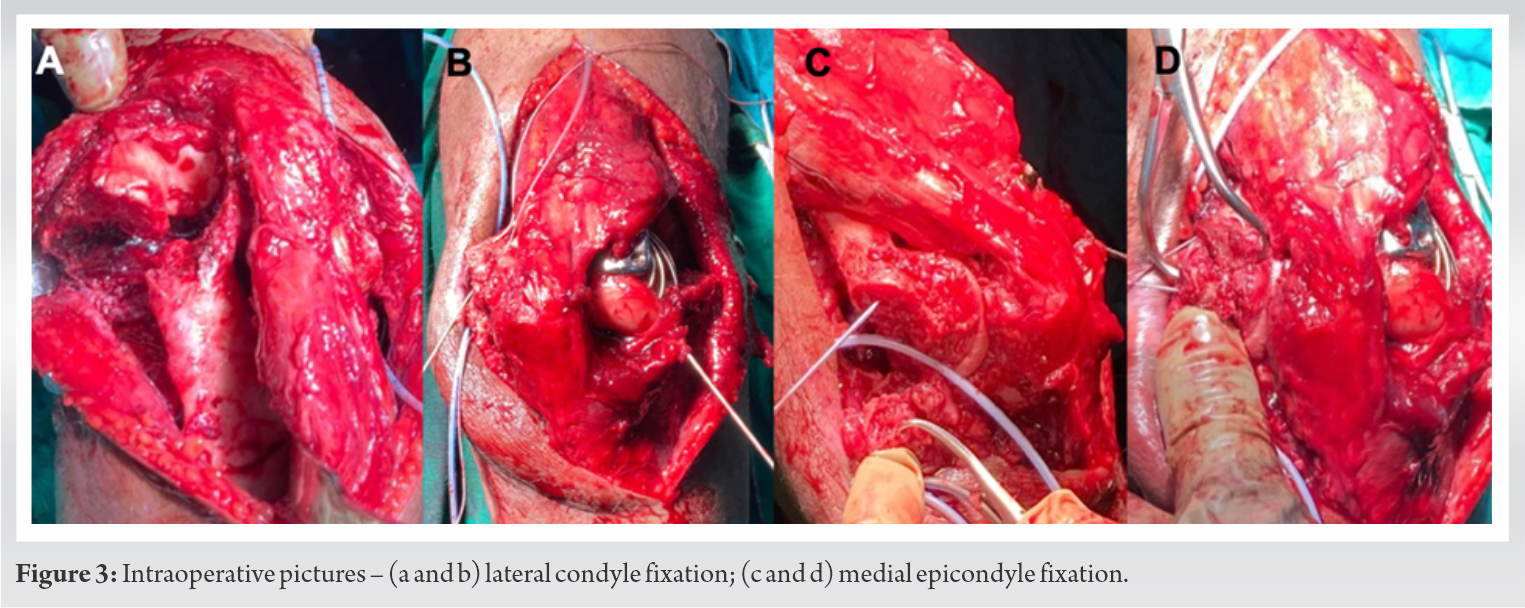 The coronal articular fragments were found to be severely comminuted with a lack of bone stock. The articular fragments were too small and thin for Herbert screws and had minimal subarticular bone for any 2.5 mm screws through the plate. Subarticular K-wires were inserted just below the articular cartilage in parallel cantilever pattern (Fig. 4) and along the para-articular curvature of the articular surface of capitellum and then the ends were coalesced and buried under a lateral pillar plate to provide a stable and rigid interface with the lateral column. Final tightening of the screws was done after engaging all the K-wires behind the plate.
The coronal articular fragments were found to be severely comminuted with a lack of bone stock. The articular fragments were too small and thin for Herbert screws and had minimal subarticular bone for any 2.5 mm screws through the plate. Subarticular K-wires were inserted just below the articular cartilage in parallel cantilever pattern (Fig. 4) and along the para-articular curvature of the articular surface of capitellum and then the ends were coalesced and buried under a lateral pillar plate to provide a stable and rigid interface with the lateral column. Final tightening of the screws was done after engaging all the K-wires behind the plate. K-wires were used for fixation as the articular fragments were too thin to get hold with screws. With lack of bone stock and thin subarticular bone, cancellous screws could not be used for the same.
K-wires were used for fixation as the articular fragments were too thin to get hold with screws. With lack of bone stock and thin subarticular bone, cancellous screws could not be used for the same.
The medial epicondyle was cartilaginous and quite small, making it unsuitable for screw fixation without a substantial risk of comminution. The ulnar collateral ligament was visualized and no frank tear was found. The fracture was stabilized with help of K-wire and was then fixed with the help of suture anchors and FiberWire sutures but satisfactory fixation was not achieved. The medial epicondyle was then fixed with the help of K-wires and tension band wiring. At the end of the procedure, we confirmed the stability of the elbow by testing the range of motion in all planes and found it satisfactory. The wound was then closed in layers after anterior transposition of the ulnar nerve and putting a suction drain. The necrotic skin tissues were excised along with the non-healing wound and skin edges were freshened which left a fresh wound of (4*3 cm) without skin coverage. The rest of the wound was sutured with staples. A posterior above-elbow slab was applied after proper antiseptic dressing of the wound. The drain was in situ for 24 h and later removed. The patient was started on Indomethacin 25 mg 8 hourly for 2 weeks post-surgery. After proper wound care and inspection, the patient was discharged on the 6th post-operative day and was advised for wound management follow-up weekly. Active-assisted mobilization of the elbow joint was started after 3 weeks of surgery. The patient was advised to attend the rehabilitation department for physiotherapy for 6 weeks and his progress was monitored throughout. At 8 months post-operative period, the patient had a painless range of motion of the flexion-extension with flexion of 110° and extension lag of 20°. The radiographic review at 8 months also showed good bony union (Fig. 5). 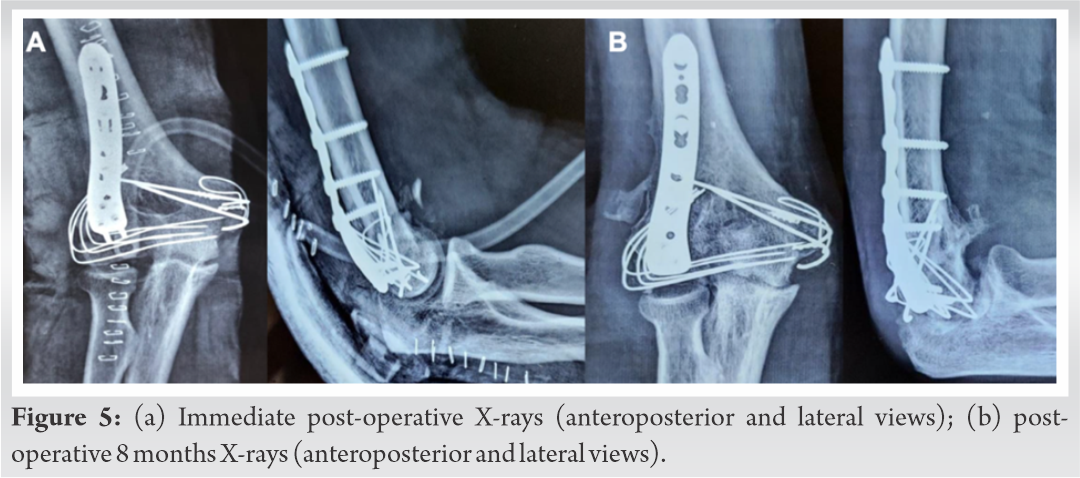 The range of supination was 80° and pronation was at 5° (Fig. 6). The post-operative wound was completely healed with no complications.
The range of supination was 80° and pronation was at 5° (Fig. 6). The post-operative wound was completely healed with no complications.
With COVID-19 being declared a global pandemic and halt of surgeries in infected patients, orthopedic surgeons were forced to delay surgeries to reduce the spread and prevent shortages of essential equipment. Only, urgent surgeries, such as life- or limb-threatening related cases, were being operated on by most surgeons. This has led to an increase in the number of conservatively managed conditions that required early operative intervention. Most of the earlier studies have recommended treatment of elbow dislocation in <3 weeks post-injury [3]. There are more chances of the development of soft-tissue contracture and osteoporosis after 3 weeks which makes the management more difficult and may lead to articular damage too [3,4,5]. Acute anterior elbow dislocations of the elbow joint, though comparatively rare, have been described in the literature [6,7,8,9]. An associated fracture of olecranon and condyles has been reported [6,7,8]. The clinical features of the case described here are similar to previously described cases with flexion deformity, pain, swelling, and restricted range of motion [1,2,3,4,5,6]. The delay in seeking treatment due to associated COVID-19 infection posed a challenge for both the patient and the surgeons. We had to face various challenges while determining the surgical approach, mode of fixation, implants to be used, soft-tissue release, and post-operative immobilization and care in our case. We planned an open reduction of the elbow by utilizing a paratricipital approach as there was an associated fracture of the lateral condyle and medial epicondyle. The triceps sparing approach helped to maintain the extension power and preserve elbow strength. The associated comminuted fracture of the lateral condyle was a big challenge in our case which was further complicated by delayed intervention and the presence of minimal subarticular bone. K-wires are of great help when it is difficult to use headless screws for extremely comminuted fragments of bone [10,11]. The inability to fix the articular comminuted fragments with standard fixation methods due to lack of good bone stock made us apply the unconventional step of using multiple cantilever K-wires and peculiarly coalescing them to provide good stability to the construct. The overall reduction achieved with the help of this method was equivalent to other standard methods and provides a good alternative in similar conditions.
To synopsize, anterior dislocation of the elbow joint when associated with fractures and delayed presentation can be a challenging problem. A good outcome can be expected by making use of multiple cantilever K-wires for the fixation of comminuted articular fragments.
This case introduces a novel technique of multiple cantilever K-wires for fixation of severely comminuted fracture in distal humerus, especially when other standard methods of fixation are non-viable.
References
- 1.Robinson PM, Griffiths E, Watts AC. Simple elbow dislocation. Shoulder Elbow 2017;9:195-204. [Google Scholar | PubMed]
- 2.Kazakos CJ, Galanis VG, Verettas DA, Dimitrakopoulou A, Polychronidis A, Simopoulos C. Unusual patterns of monteggia fracture-dislocation. J Orthop Surg Res 2006;1:12. [Google Scholar | PubMed]
- 3.Arafiles RP. Neglected posterior dislocation of the elbow. A reconstruction operation. J Bone Joint Surg Br 1987;69:199-202. [Google Scholar | PubMed]
- 4.Freeman BL 3rd. Old unreduced dislocations. In: Crenshaw AH, editor. Campbell’s Operative Orthopedics. 9th ed., Vol. 1. St Louis: Mosby; 1998. p. 2673-4. [Google Scholar | PubMed]
- 5.Rockwood CA, editor. Rockwood and Green’s fracture in adults. In: Treatment of old Unreduced Posterior Dislocation of Elbow. 4th ed., Vol. 1. Philadelphia, PA: Lippincot-Raven; 1996. p. 975-6. [Google Scholar | PubMed]
- 6.Guitton TG, Albers RG, Ring D. Anterior olecranon fracture-dislocations of the elbow in children. A report of four cases. J Bone Joint Surg Am 2009;91:1487-90. [Google Scholar | PubMed]
- 7.Venkatram N, Wurm V, Houshian S. Anterior dislocation of the ulnar-humeral joint in a so-called ‘pulled elbow’. Emerg Med J 2006;23:e37. [Google Scholar | PubMed]
- 8.Gyawali GP, Pokharel B, Pokharel RK. Irreducible anterior dislocation of the elbow without associated fracture. J Nepal Med Assoc 2013;52:398-401. [Google Scholar | PubMed]
- 9.Kumar R, Sekhawat V, Sankhala SS, Bijarnia I. Anterior dislocation of elbow joint-case report of a rare injury. J Orthop Case Rep 2014;4:16-8. [Google Scholar | PubMed]
- 10.Dubberley JH. Outcome after open reduction and internal fixation of Capitellar and trochlear fractures. J Bone Joint Surg Am 2006;88:46-54. [Google Scholar | PubMed]
- 11.Carroll MJ, Athwal GS, King GJ, Faber KJ. Capitellar and trochlear fractures. Hand Clin 2015;31:S0749071215000803. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report
April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report August 10, 2020 Gossypiboma: What Happens When a Mop is Left in a Thigh for ten Years
August 10, 2020 Gossypiboma: What Happens When a Mop is Left in a Thigh for ten Years February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review
February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review