
“Management of unconventional representation of osteochondroma needs in-depth clinical, radiological and histopathological examination."
Dr. Gireesh Khodnapur, Department of Orthopaedics, Shri B.M. Patil Medical College, BLDE Deemed to be University, Bijapur, Karnataka, India. E-mail: giri2410@gmail.com
Abstract
Introduction: Osteochondroma usually occurs in long bones, whereas smaller bones are less commonly involved. Common locations include metaphysis of the proximal tibia, distal femur, distal tibia, distal fibula, proximal femur, and proximal humerus. Metacarpals are rarely affected.
Case Report: A case report of a twenty 20-year-s old male presenting with swelling for five 5 years, which is gradually increasing in size over the hand and reached 4 cm ×x 3 cm ×x 2 cm; following clinical and radiological examination, the patient was diagnosed with osteochondroma of a fifth metacarpal head of the right hand. We did magnetic resonance imaging scan for confirmation and reported it as osteochondroma which was treated surgically with excision of swelling in total, and specimen sent for histopathology and osteochondroma was confirmed.
Conclusion: Osteochondromas can rarely occur at unusual sites such as small bones of the hand and foot. Therefore, osteochondroma should be considered a differential diagnosis alongside other common tumours of the hand and foot, such as enchondroma (Olliers diseases).
Keywords: Metacarpal, olliers disease, osteochondroma.Metacarpal, Osteochondroma, Olliers disease
Osteochondroma is one of the most common benign tumors of bone [1]. Osteochondroma of hand is uncommon, accounting for 4% of solitary cases. It usually presents in the second or third decade of life. It usually grows away from the growing end of the bone until the patient attains bone maturity. It when presents at multiple sites, it is called multiple hereditary exostoses. Osteochondromas can develop as a single tumor (osteocartilaginous exostosis) or as many tumors (multiple osteochondromatosis) [2]. A solitary osteochondroma may develop if bone grows out from the growth plate instead of in line with it. Most of the bony exostosis are asymptomatic until they grow to start compressing neurovascular bundles or nearby vital organs. Osteochondromas more frequently affect the appendicular skeleton (upper and lower limbs). In situations in which excision of the osteochondroma has been chosen, this is usually curative. Recurrence has been seen in cases of incomplete removal, which means incomplete removal of the cartilaginous cap. These bony outgrowths sometimes may aggressively turn into malignant lesions.
In January 2021, a 20-year-old male presented with swelling over the right hand for 5 years, insidious in onset, progressive in nature, located over the medial border on the palmar side (Fig.1 and 2). The swelling was associated with dull aching minimal pain, aggravated with excessive activities and relived on rest. However, the swelling was not associated with night pain, fever, and restriction in daily routine activities.
On clinical examination, the swelling was of size 4 cm × 3 cm × 2 cm (Fig.1 and 2), bony hard, irregular surface, adherent to the underlying bone with no coronal or sagittal plane movement possible. It was palpable on the ulnar aspect of the hand. There was no local rise of temperature, and the patient has no regional lymphadenopathy, scars, sinuses, dilated veins, and skin changes on and around the swelling. There are no similar swellings elsewhere in the body.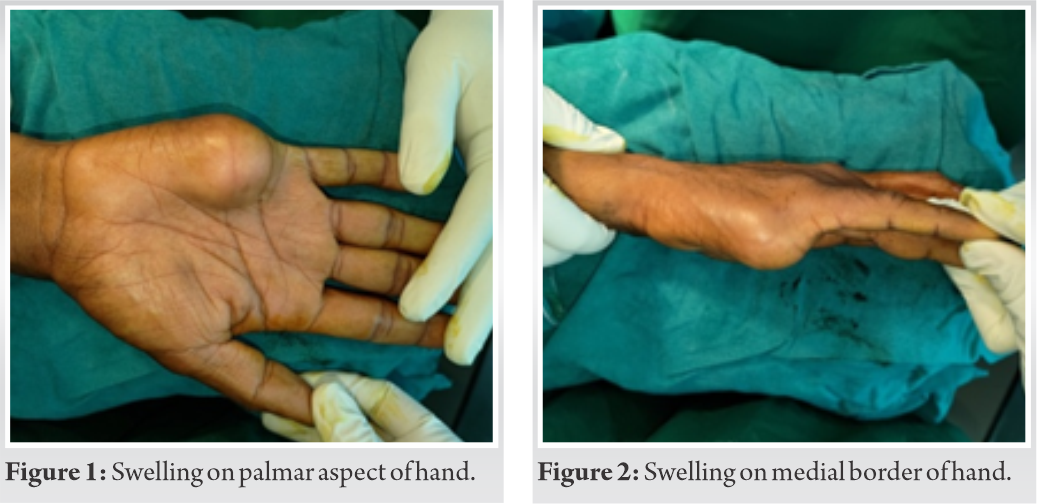
Radiographs (X-ray) showed a pedunculated bony lesion arising from the distal metaphyseal region of the fifth metacarpal (Fig. 3).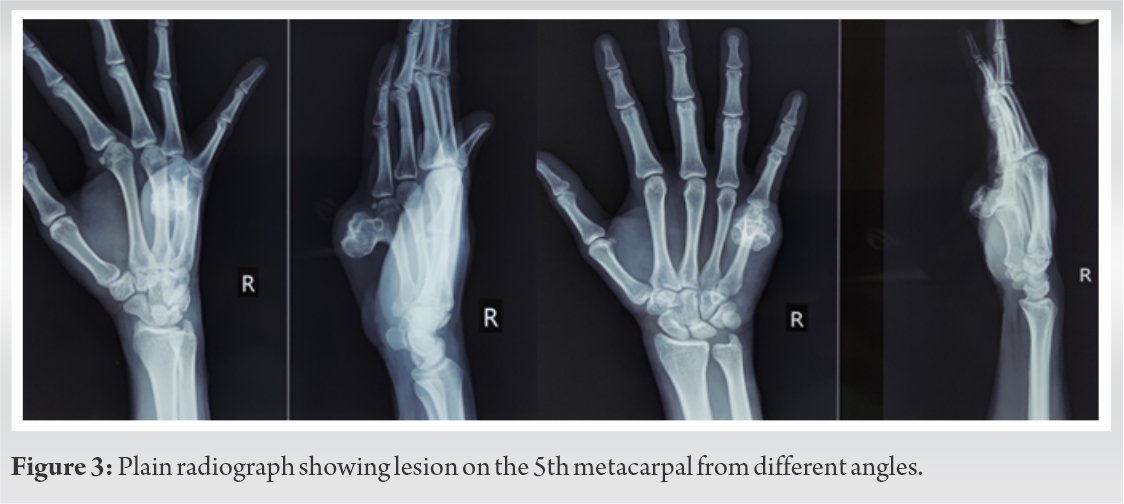
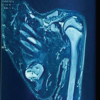
In magnetic resonance imaging, there was evidence of 2 × 2.5 × 3 cm (AP × TR × SI) sized bony overgrowth seen arising from distal metaphyseal region of 5th metacarpal bone showing continuity with a medullary cavity in growing away from epiphysis (Fig. 4). 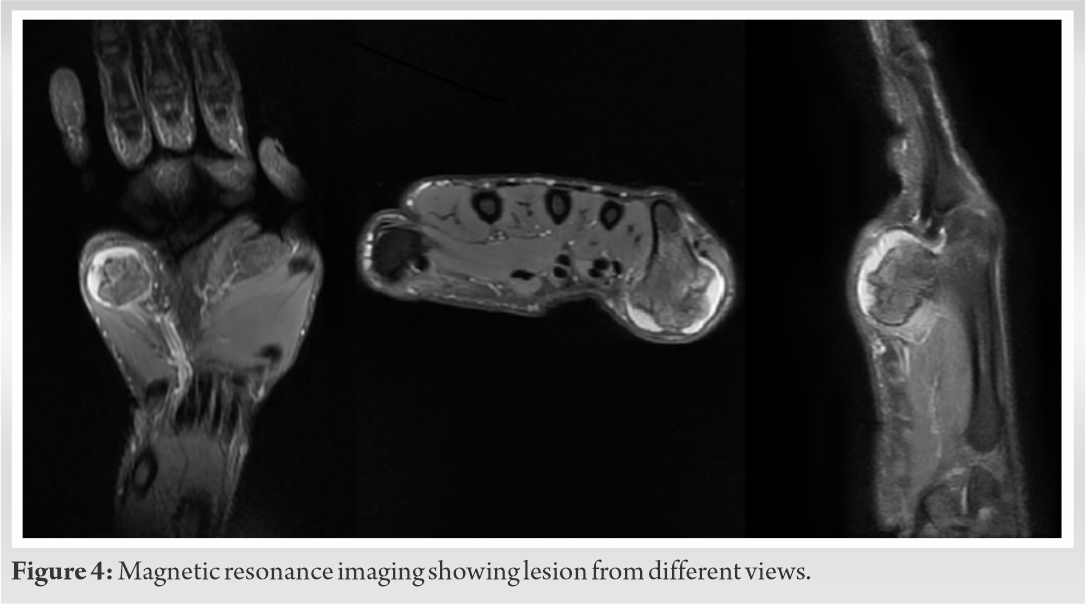 This lesion is seen displacing the 5th flexor digitorum profundus tendon laterally and causing compression over flexor digiti minimi and abductor digiti minimi muscles. In addition, there was evidence of the formation of bursa with inflammatory collection within the bursa. A provisional diagnosis of osteochondroma was made based on clinical and radiological findings.
This lesion is seen displacing the 5th flexor digitorum profundus tendon laterally and causing compression over flexor digiti minimi and abductor digiti minimi muscles. In addition, there was evidence of the formation of bursa with inflammatory collection within the bursa. A provisional diagnosis of osteochondroma was made based on clinical and radiological findings.
Osteochondroma excised under general anesthesia and tourniquet control, the bony swelling was approached through the posteromedial incision (Fig. 5). Tumor of size approximately 3 × 2 cm was excised from the root of the pedicle (Fig. 6). The excised specimen was then sent for histopathological examination.
The histopathological report (HPR) showed a cartilaginous cap with underlying bony tissue with bony trabeculae. The cartilaginous tissue is lined by perichondrium and is composed of clusters of chondrocytes. At foci, the chondrocytes are organized into cords and show endochondral ossification, which is continuous with bony tissue. HPR did not show any mitotic activity or necrosis in the sections studied (Fig. 7).
Post-operative period was uneventful, check x-ray of the hand was taken on day 1 with satisfactory findings (Fig. 8), regular dressing was done and sutures were removed on post-operative day 12. The patient had minimal pain at the operative site with a complete and painless range of motion at the wrist and metacarpophalangeal joint. At 1 year of follow up patient was evaluated radiologically (Fig. 9) and clinically (Fig. 10) with satisfactory outcome.
A study reported that only four of 1024 solitary osteochondromas were in the metacarpal [3]. A solitary osteochondroma of the metacarpal neck resulting in flexion deformity of the metacarpophalangeal joint was treated by excision [4].
They are usually asymptomatic and are discovered incidentally. The clinical picture includes a painless, non-tender lump/mass. Osteochondroma involves the epiphysis of a long bone in patients with open physeal cartilage [5]. They are developmental malformation rather than true neoplasm and are thought to be originated from the periosteum [6]. It is also defined as a cartilage caped osseous tumor projecting from the surface of the affected bone. Exostosis is produced by progressive endochondral ossification of the hyaline cartilaginous cap, which essentially functions as a growth plate [7]. Osteochondroma commonly occurs at metaphysis of the proximal tibia, distal femur, distal tibia, distal fibula, proximal femur, and proximal humerus.
Kishore et al. reported a rare case of osteochondroma in the craniofacial region located at the left parasymphyseal area of the mandible in a 9-year-old female child [8].
Bhatnagar et al. reported a rare clinical and radiologic finding of a patellar osteochondroma in a 50-year-old female, which was surgically resected and was followed up for 2 years, confirming no complaints and sign of recurrence [9].
Patella, mandible, and scapula are the other rare sites where osteochondroma has been reported [8,9,10].
In our case presentation, the patient presented with osteochondroma with an unusual location of the 5th metacarpal.
The radiograph shows an irregular outgrowth with a cartilage cap arising from the metaphysic of the 5th metacarpal.
A case report by Rajappa et al. shows recurrence of osteochondroma of metacarpals after excision [11].
The lesion was extra-articular and allowed to be excised completely, thus reducing the chance of recurrence.
Although unusual, osteochondromas can present in the hand region and need to be evaluated with clinical and radiological suspicion. Whenever a patient is having pressure-related symptoms, excision should be performed. Histopathological confirmation is must be following complete excision. The patient needs to be counseled for the recurrence of the tumor.
Diagnosing osteochondroma at common sites such as distal femur, proximal tibia, and proximal humerus may not be challenging, but bony growth at unusual locations such as metacarpal, metatarsal, scapula, fibula, and skull require thorough clinical, radiological, and histopathological examination to confirm osteochondroma.
References
- 1.Singh R, Jain M, Siwach R, Rohilla S, Sen R, Kaur K. Large para-articular osteochondroma of the knee joint: A case report. Acta Orthop Traumatol Turc 2012;46:139-43. [Google Scholar | PubMed]
- 2.Haaga JR, Dogra VS, Frosting M, Gilkeson RC, Sundaram M. CT and MRI of Whole Body. 5th ed., Vol. 2. Philadelphia, PA: Mosby, Elsevier; 2009. p. 2134-5. [Google Scholar | PubMed]
- 3.Unni KK, Dahlin DC. Dahlin’s Bone Tumors. General Aspects and Data on 11,087 Cases. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996. [Google Scholar | PubMed]
- 4.Kamath BJ, Menezis R, Binu S, Bhardwaj P. Solitary osteochondroma of the metacarpal. J Hand Surg Am 2007;32:274-6. [Google Scholar | PubMed]
- 5.Weinstein SL, Buckwalter JA, editors. Turek’s Orthopaedics: Principles and their Application. Philadelphia, PA: Lippincott Williams and Wilkins; 2005. [Google Scholar | PubMed]
- 6.Azar FM, Canale ST, Beaty JH. Campbell’s Operative Orthopaedics, E-Book. Amsterdam, Netherlands: Elsevier; 2020. [Google Scholar | PubMed]
- 7.Herring JA, Tachdjian MO. Pediatric Orthopaedics. In: Benign Musculoskeletal Tumours. 5th ed., Ch. 9. Philadelphia, PA: WB Saunders; 2002. [Google Scholar | PubMed]
- 8.Kishore DN, Kumar HR, Umashankara KV, Rai KK. Osteochondroma of the mandible: A rare case report. Case Rep Pathol 2013;2013:167862. [Google Scholar | PubMed]
- 9.Bhatnagar AS, Malhan K, Mehta S. A rare case report of patellar osteochondroma. J Orthop Case Rep 2015;5:72. [Google Scholar | PubMed]
- 10.Ambulgekar RK, Jaiswal N, Kandolkar PG, Thakkar RD, Rahul B. A case report of a rare location solitary osteochondroma: Scapula. Niger J Basic Clin Sci 2015;12:126. [Google Scholar | PubMed]
- 11.Rajappa S, Kumar MM, Shanmugapriya S. Recurrent solitary osteochondroma of the metacarpal: A case report. J Orthop Surg 2013;21:129-31. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report