
CLAP may be a novel treatment method that can be expected to achieve bone healing while preserving the implant in FRI cases after open tibial fracture
Dr. Akihiro Maruo, Department of Orthopaedic Surgery, Steel Memorial Hirohata Hospital, 3-1, Yumesaki-cho, Hirohata-ku, Himeji 671-1122, Japan. E-mail: maruchan777natu@me.com
Abstract
Introduction: We encountered a case of post-operative infection of an open tibial fracture that was controlled by continuous local antibiotic perfusion (CLAP), a novel method of fracture-related infection (FRI) that we have developed. CLAP is a procedure in which a bone marrow needle and a double lumen tube are placed in the infected area, and an appropriate concentration of antimicrobial agent is continuously administered and perfused.
Case Report: The patient was a 78-year-old woman. She was hit by a motor vehicle and fell to the farmyard floor. She suffered multiple traumas, including a lower leg open fracture, multiple rib fractures, clavicle fracture, pelvic fracture, mandibular fracture, and liver injury. Her tibial fracture was a Gustilo-Anderson type IIIA open fracture. After debridement and external fixation of the tibial open fracture on the same day, open reduction and internal fixation with an intramedullary nail was performed 3 days after the injury. Twelve days after the injury, local heat and redness were observed at the nail insertion wound and the posteromedial calf, and a purulent clot was discharged from the open wound. We performed curettage of the lesion and retained the implant. CLAP was then constructed to perfuse local antibiotics along the nail and large hematoma area. Locally, the inflammation improved and the inflammatory response became negative 3 weeks after the initiation of CLAP. Six months after surgery, bony union was achieved. At present, 3.5 years after the internal operation, there is no sign of infection, and the patient has returned to her pre-injury life with no abnormalities in motor function.
Conclusion: CLAP may be a novel treatment method that can be expected to achieve bone healing while preserving the implant in FRI cases after open tibial fracture.
Keywords: Open tibial fracture, fracture-related infection, continuous local antibiotic perfusion, gentamicin.
An open fracture is generally defined as a soft-tissue injury with a fracture, where there is a connection between the fracture site and the outside. The pathogenesis of open fractures is composed of four elements: Fracture, soft-tissue injury, neurovascular injury, and wound infection. In cases of open fracture, it is important to fully evaluate the condition, comprehensively understand the trauma, and formulate a treatment plan based on the evaluation. One of the most important factors is the control of wound infection. Strict infection control is considered necessary because many open fractures acquire bacteria after trauma [1]. Previously, bone cement containing antimicrobial agents, antibiotic-eluting ceramic bone substitutes, and coated nails have been used to treat fracture-related infection (FRI); however, their therapeutic effect is limited, with a recurrence rate of approximately 12% to chronic infection [2]. In our hospital, difficult-to-treat FRI and soft-tissue infections have been treated using continuous local antibiotic perfusion (CLAP), in which antibiotics are continuously circulated throughout the infected lesion. We addressed the treatment for FRI by “intra-medullary antibiotic perfusion” (iMAP) and for soft-tissue infection by “intra-soft tissue antibiotic perfusion” (iSAP); some cases are treated with a combination of both. In this study, we report a case of acute infection in an elderly patient with an open fracture of the lower leg treated with CLAP, which resulted in bone healing while preserving the implant.
A 78-year-old woman was injured in a traffic accident while riding a motorcycle and thrown to the farmyard floor. The patient was transported to our hospital by helicopter. On arrival at the hospital, she was conscious and her vital signs were maintained. Fractures of AO classification 42B2 and 4FB2 were observed on the left lower leg and a Gustilo-Anderson classification Type IIIA open fracture was observed on the posteromedial surface of the lower leg (Fig. 1, 2). She also suffered multiple traumas, including multiple rib fractures, clavicle fracture, pelvic wing fracture, and liver injury, which were treated conservatively. An operation on the mandibular fracture was performed later.
On the same day of the injury, debridement and external fixation for the tibial open fracture were performed in the operating room (Fig. 3). Three days after the injury, internal fixation with intramedullary nails was performed (Fig. 4).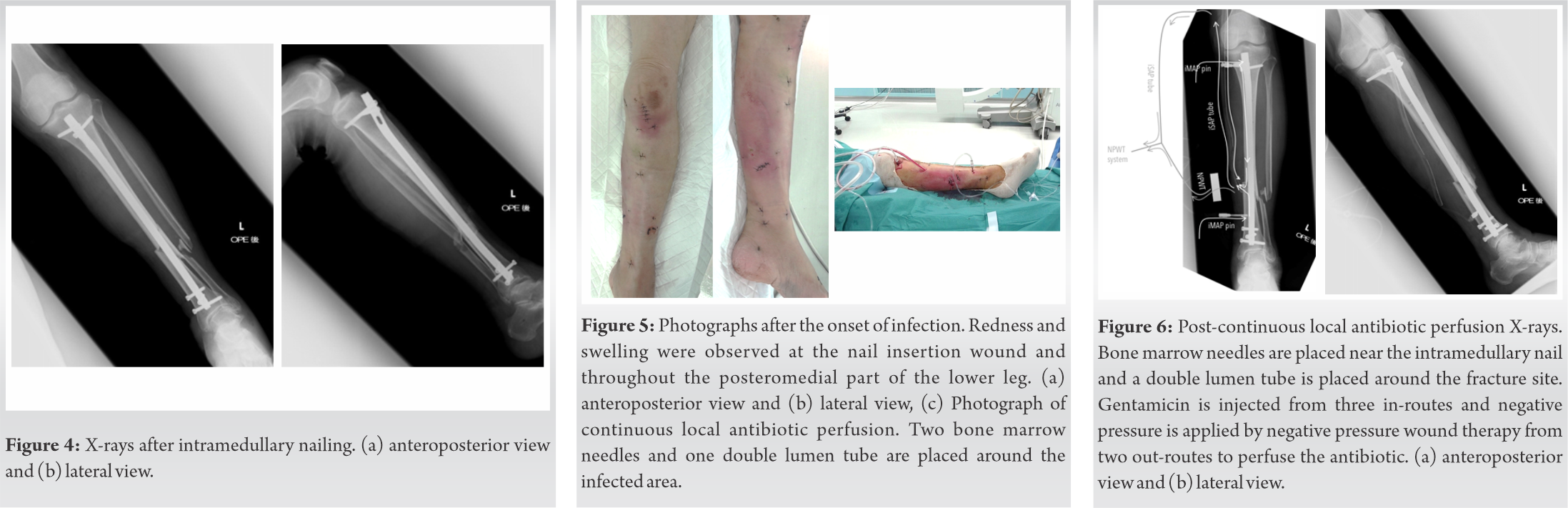 Twelve days after the injury, local heat and pus discharge from the wound were observed, and Aeromonas hydrophila was detected in the wound culture examination. Redness and swelling were observed at the nail insertion wound and throughout the posteromedial part of the lower leg (Fig. 5), suggesting that the infection had spread along the whole nail, resulting in a large subcutaneous hematoma on the calf. In addition, an increased white blood cell count and C-reactive protein levels were recognized in the blood examination, which matched the major and minor criteria of FRI [3].
Twelve days after the injury, local heat and pus discharge from the wound were observed, and Aeromonas hydrophila was detected in the wound culture examination. Redness and swelling were observed at the nail insertion wound and throughout the posteromedial part of the lower leg (Fig. 5), suggesting that the infection had spread along the whole nail, resulting in a large subcutaneous hematoma on the calf. In addition, an increased white blood cell count and C-reactive protein levels were recognized in the blood examination, which matched the major and minor criteria of FRI [3].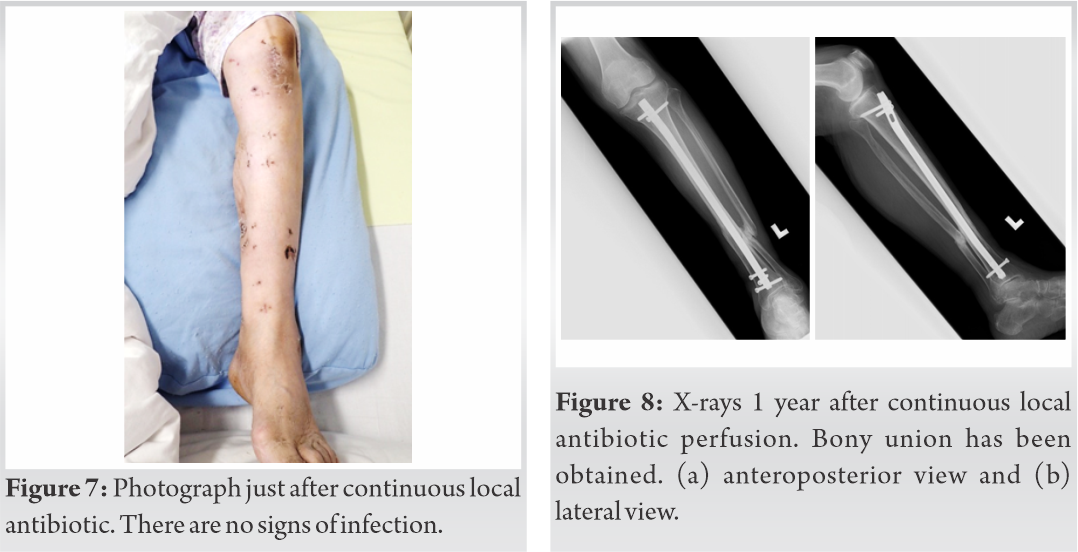
Curettage of the infected lesion and CLAP was initiated (Fig. 5, 6). Bone marrow needles (Senko Medical, Tokyo, Japan) with a diameter of 3 mm as an iMAP pin were percutaneously inserted at the proximal end of the nail and distal part of the fracture site. Both iMAPs confirmed that fluid flow was observed throughout the fracture gap allowing intensive washout along the nail. Using this method, intramedullary contaminated bacteria were eliminated during surgery and the antibiotic solution was perfused postoperatively, instead of hematoma pooling along the nail for recurrent risk of infection. A 22Fr double-lumen tube (Salem sump tube: Coviden Japan) as an iSAP tube was placed from the proximal end of the hematoma area to the fracture site and the fluid flow from the iMAP pin was aspirated by this tube. Therefore, CLAP systems were constructed in the water stream for the entire infection area, including inside the tibia and affected soft tissue. Immediately, after surgery, 1200 μg/ml gentamicin was administered at 2 ml/h through three routes (two needles and the in-route of double-lumen tube). Negative pressure wound therapy (NPWT) was applied to the subcutaneous dead space area to prevent pooling hematoma and to connect the out-route of the double-lumen tube to the NPWT tube for drainage collection. In this way, negative pressure was applied to the NPWT of the soft port as well as the iSAP tube. This system may help to effectively circulate the CLAP system under negative pressure. According to the trough value of gentamicin (1.0 mg/ml), we applied a protocol in which the upper limit of the blood concentration of gentamicin was set at 1.0 mg/dl, and the administration dose was decreased if the blood concentration exceeded the upper limit. In this case, the blood concentration of gentamicin was 1.8 mg/ml on the 7th day after beginning CLAP, so the three in-routes were changed to 600 μg/ml. The blood concentration of gentamicin dropped to the safe level at the next blood examination and was maintained until termination of CLAP. The local concentration of gentamicin was monitored by collecting fluid using NPWT. The gentamicin concentration was maintained at more than 600 μg/ml to confirm that a sufficient dose was distributed in the infected area. On the 18th day after the start of CLAP, the bone marrow needles were removed, local administration of gentamicin was terminated, and NPWT was continued until the discharge fluid was diminished. Two days later, fluid discharge was stopped from the tube, the double-lumen tube was removed, and NPWT was discontinued on the 20th day after the start of CLAP. Local findings improved a few days after CLAP and completely disappeared at the end of CLAP. Furthermore, the inflammatory response became negative 3 weeks after CLAP was applied (Fig. 7). In combination with systemic administration of antibiotics, 6 g/day of ABPC/SBT was administered for 6 weeks at the same time as CLAP. During the CLAP treatment, a continuous passive motion machine of the knee was applied during the daytime to facilitate fluid circulation in the CLAP system and prevent knee stiffness. Therefore, the patients maintained a knee range of motion from 0° to 130° by the end of CLAP. She started 1/3 partial weight bearing (PWB) 6 weeks after internal fixation and 2/3 PWB at 8 weeks. She was allowed to walk with a walker from 9 weeks. Bone union was achieved 6 months postoperatively. Three years and 6 months after CLAP, she returned to her pre-injury life with no signs of infection and no abnormalities in her motor function (Fig. 8).
The treatment principle for open fractures is debridement of the necrotic and infected tissues, followed by bone stabilization and soft-tissue reconstruction [4]. Regarding infection caused by open fractures of the lower leg, a recent review reported that systemic administration of antibiotics within 3 h of injury reduced the infection rate by 1/6, and that when antibiotics were administered within 66 min of injury, the infection rate was 0%; however, when antibiotics were administered beyond this time, the infection rate increased by 17% [5]. Therefore, prevention and treatment of infection by the administration of antibiotics are very important in the treatment of open fractures. The risk of infection increases with the severity of the fracture, and in patients with Gustilo and Anderson Type IIIB and IIIC fractures, the infection rate was reported to be more than 31% in patients who received systemic antibiotics alone, but improved to less than 9% when antibiotic-containing coated nails were used in combination with systemic antibiotics [6]. This suggests that systemic antibiotic administration and local antibiotic administration are important in preventing post-operative infection in open fractures. Therefore, implant removal is required to eradicate biofilms; however, implant removal leads to disadvantages for infection control as it results in a large dead space to grow bacteria, instability of the fracture site, and a disrupted blood supply to the segmental bone. Implant retention and biofilm eradication are essential to cure FRI and local antibiotic administration plays a key role in the treatment. In a meta-analysis of patients with open tibial fractures, those who received systemic antibiotics in the perioperative period had an infection rate of 14.4% while those who received local antibiotics using antibiotic-coated nails in combination with systemic antibiotics had a reduced infection rate of 2.4% with an odds ratio of 0.17. Local antibiotic administration methods include antibiotic-impregnated cements, antibiotic-impregnated ceramics, and antibiotic-coated implants [7,8]. However, these methods of antibiotic administration have been reported to have several problems. First, antibiotic-impregnated cements and ceramics do not allow immediate removal of the cause if allergic symptoms appear [8]. Therefore, there is a risk of implant removal or revision surgery to remove the cause of the allergic reaction. Second, in local administration methods that use local implantation of antibiotic-coated implants and sustained release of antimicrobial agents (e.g., antibiotic-impregnated cement implantation and antibiotic-coated implants), it has been pointed out that the local concentration of antibiotics increased to very high levels on the 1st day and rapidly decreased to less than the minimal biofilm eradication concentration (MBEC) from a few days after surgery and maintained the minimum inhibitory concentrations (MIC) for a month [8]. Antimicrobial agents at concentrations of 100–1000 times the MIC have been reported to be required to eradicate the biofilm, which is defined as the MBEC [9]. Therefore, it may be difficult to retain the implant that is affected by biofilm formation. In addition, biofilm formation was observed at the surface of the cement after release of the antimicrobial agent. [10]. Third, when the infection subsided with antibiotic-impregnated cement implantation, it was necessary to remove the antibiotic-impregnated materials. The dead space after antibiotic carriers could be a risk factor for infection recurrence.
The advantages of CLAP are that the antimicrobial agent can be administered locally at any concentration for any period of time. The application of negative pressure enables the delivery of antibiotic agents to any place including inside the bone. The iMAP pin and iSAP tube can be removed without general anesthesia after termination of the treatment without creating a dead space. In CLAP, antibiotics are administered through the route of the double-lumen tube, which is implanted in the bone marrow needle and soft tissue, and antibiotic perfusion is performed by collecting drainage through the out-route of the double-lumen tube. The out-route was drained using a NPWT system (Renasys; Smith and Nephew Medical Ltd., Kingston upon Hull, UK). We believe that the concentration of antibiotics can be maintained at a constant level by administering antibiotics continuously from each route. Biofilms are known bacteria aggregating the extracellular matrix at the surface of the implant and necrotic tissue and cause high antibiotic resistance. Antibiotic resistance is enhanced during biofilm maturation. For the selection of antibiotics in CLAP, we used gentamicin, an aminoglycoside antibiotic that is bactericidal and concentration dependent. The usefulness of gentamicin has been reported previously, especially against bacterial biofilms in post-operative orthopedic infections, and it has been reported that high concentrations of gentamicin have sufficient antimicrobial activity regardless of the species [11,12]. However, an increase in the blood concentration of gentamicin may cause complications such as renal dysfunction [13]; therefore, we believe that it is important to monitor the blood concentration of gentamicin. We monitored the blood levels of gentamicin as a standard protocol for CLAP. Regarding the cause of this infection, A. hydrophila is an anaerobic bacteria widely detected in rivers, lakes, and farmyards; it has been reported to be a serious skin and soft-tissue infection as a result of trauma. The mortality rate of septic shock caused by A. hydrophila is extremely high [14]. There have been no reports of the successful treatment of FRI cases infected with this bacterium while preserving implants [15]. Anaerobic bacteria are hard to detect by culture because air exposure may deactivate the bacteria, which survive anaerobic environments such as deep soft tissue and inside the bone. We believe that CLAP could provide appropriate drug delivery for severe FRI caused by A. hydrophila.
CLAP may be a novel drug delivery system that can be expected to achieve bone healing while preserving the implant in FRI cases after open tibial fracture.
CLAP may be a novel treatment method that can be expected to achieve bone healing while preserving the implant in FRI cases after open tibial fracture.
References
- 1.Gustiko RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bone: Retrospective and prospective analysis. J Bone Joint Surg Am 1976;58:453-8. [Google Scholar | PubMed]
- 2.Leung AH, Hawthorn BR, Simpson AH. The effectiveness of local antibiotics in treating chronic osteomyelitis in a cohort of 50 patients with an average of 4 years follow-up. Open Orthop J 2015;9:372-8. [Google Scholar | PubMed]
- 3.Metsemakers WJ, Morgenstern M, Senneville E, Borens O, Govaert GA, Onsea J, et al. General treatment principles for fracture-related infection: Recommendations from an international expert group. Arch Orthop Trauma Surg 2020;140:1013-27. [Google Scholar | PubMed]
- 4.Diwana A, Eberlinb KR, Smith RM. The principles and practice of open fracture care. Chin J Traumatol 2018;21:187-92. [Google Scholar | PubMed]
- 5.Sop JL, Sop A. Open fracture management. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2021. [Google Scholar | PubMed]
- 6.Craig J, Fuchs T, Jenks M, Fleetwood K, Franz D, Iff J, et al. Systematic review and meta-analysis of the additional benefit of local prophylactic antibiotic therapy for infection rates in open tibia fractures treated with intramedullary nailing. Int Orthop 2014;38:1025-30. [Google Scholar | PubMed]
- 7.Pesch S, Hanschen M, Greve F, Zyskowski M, Seidl F, Kirchhoff C. Treatment of fracture related infection of the lower extremity with antibiotic eluting ceramic bone substitutes: Case series of 35 patients and literature review. Infection 2020;48:333-44. [Google Scholar | PubMed]
- 8.Ferguson J, Diefenbeck M, McNally M. Ceramic biocomposites as biodegradable antibiotic carriers in the treatment of bone infections. J Bone Joint Infect 2017;2:38-51. [Google Scholar | PubMed]
- 9.Sandoe JA, Wysome J, West AP, Heritage J, Wilcox MH. Measurement of ampicillin, vancomycin, linezolid and gentamicin activity against enterococcal biofilms. J Antimicrob Chemother 2006;57:767-70. [Google Scholar | PubMed]
- 10.Neut D, van de Belt H, Stokroos I, van Horn R, van der Mei HC, Busscher HJ. Biomaterial-associated infection of gentamicin-loaded PMMA beads in orthopaedic revision surgery. J Antimicrob Chemothther 2001;47:885-91. [Google Scholar | PubMed]
- 11.Wininger DA, Fass RJ. Antibiotic-impregnated cement and beads for orthopedic infections. Antimicrob Agents Chemothe 1996;40:2675-9. [Google Scholar | PubMed]
- 12.Meo DD, Cannari FM, Petriello L, Persiani P, Villani C. Gentamicin-coated tibia nail in fractures and nonunion to reduce fracture-related infections: A systematic review. Molecules 2020;25:5471. [Google Scholar | PubMed]
- 13.Maczynska B, Secewicz A, Smutnicka D, Szymczyk P, Wicher RD, JunkaI A, et al. In vitro efficacy of gentamicin released from collagen sponge in eradication of bacterial biofilm preformed on hydroxyapatite surface. PLoS One 2019;14:e0217769. [Google Scholar | PubMed]
- 14.Monaghan SF, Anjaria D, Mohr A, Livingston DH. Necrotizing fasciitis and sepsis caused by Aeromonas hydrophila after crush injury of the lower extremity. Surg Infect (Larchmt) 2008;9:459-67. [Google Scholar | PubMed]
- 15.Agrawal S, Srigyan D, Nag HL, Kapil A, Dhawan B. Chronic osteomyelitis by Aeromonas hydrophila: A silent cause of concern. J Lab Physicians 2017;9:337-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2024 Multiple Vertebral Compression Fractures Secondary to Pregnancy-induced Osteoporosis: A Case Report
June 10, 2024 Multiple Vertebral Compression Fractures Secondary to Pregnancy-induced Osteoporosis: A Case Report September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber
September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber July 10, 2016 Non-traumatic Thoracic Vertebral Compression Fractures Occurred in a Young Epileptic Patient: A Case Report
July 10, 2016 Non-traumatic Thoracic Vertebral Compression Fractures Occurred in a Young Epileptic Patient: A Case Report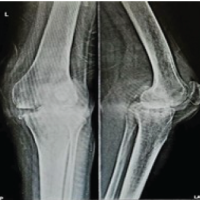 September 1, 2025 Total Knee Arthroplasty in Tuberculous Arthritis of the Knee – A Case Report
September 1, 2025 Total Knee Arthroplasty in Tuberculous Arthritis of the Knee – A Case Report