
Fibrocartilaginous dysplasia is a rare variant of fibrous dysplasia which needs to be differentiated from other cartilaginous neoplasms of bone, thereby preventing misdiagnosis.
Dr. Archana Lakshmanan, Department of Histopathology, Apollo Hospitals, Chennai, India. E-mail: mrithulaarchana@gmail.com
Abstract
Introduction: Fibrocartilaginous dysplasia (FCD) is a variant of fibrous dysplasia (FD) with extensive cartilaginous differentiation. This has been reported in both monostotic and polyostotic types of FD, the proximal femur being the most common site involved.
Case Report: We report five cases of fibrocartilaginous dysplasia with varying degrees of cartilaginous differentiation. The age of the patients ranged from 7 to 30 years, and there was a female predominance (M:F ratio of 1:4). The proximal femur was the site of involvement in all the cases. Imaging showed well demarcated radiolucent lesions with stippled calcifications. Histologically, cartilaginous areas were noted juxtaposed to typical areas of fibrous dysplasia. Four of the patients were treated with curettage and one with a marginal resection. None of the five cases had recurrences at the past follow-up.
Conclusion: FCD is a rare variant of fibrous dysplasia which needs to diagnosed and treated early, as there is a high risk of pathological fracture.
Keywords: Fibrous dysplasia, fibrocartilaginous, cartilaginous tumors, enchondroma, chondrosarcoma.
Fibrous dysplasia is a benign fibro-osseous lesion of the bone that occurs due to a dysplastic process involving the bone forming mesenchyme. They can be either monostotic or polyostotic and have a predilection for long bones (especially the femur), craniofacial bones, and ribs [1]. There is a wide morphologic spectrum including the infrequent presence of cartilage. Fibrocartilaginous dysplasia is an extreme end of the spectrum of FD with marked cartilaginous overgrowth. Radiological and histopathological findings in some cases, especially if only the cartilaginous component is sampled at biopsy may be mistaken for cartilaginous neoplasms causing a diagnostic dilemma [2,3,4].
We report five cases of fibrocartilaginous dysplasia with clinical, radiological, and pathological features and review the literature of this interesting entity.
This study included five cases of fibrous dysplasia with varying degrees of cartilaginous differentiation reported at Apollo Hospitals, Chennai. Archived Hematoxylin and Eosin stained sections of these cases were reviewed and fresh sections recut where necessary. The clinical findings of these cases were obtained from the patients’ medical records; and radiological images were available and were reviewed. This study was approved by ethics committee (institutional review board). Four of the cases were children and one was an adult (age range: 8–30 years). There were four females and one male. The presenting symptoms were pain, swelling, or pathological fracture. The duration of symptoms was variable from few weeks to few years. Imaging revealed monostotic, well demarcated, expansile and lytic lesions with cortical thinning, and involving the neck of femur in all the cases. A classical Shepherds’ crook deformity was noted in all the cases. Fracture associated changes were noted in three cases and there was no soft tissue extension in any. Specs of calcification were noted in all the cases in variable proportions. The radiological impression was fibrous dysplasia in two cases and enchondroma in three. Curettage was done on four cases and an en bloc resection was performed in one patient. The radiograph and the image of the gross specimen of the patient with the marginal resection are shown in (Fig. 1).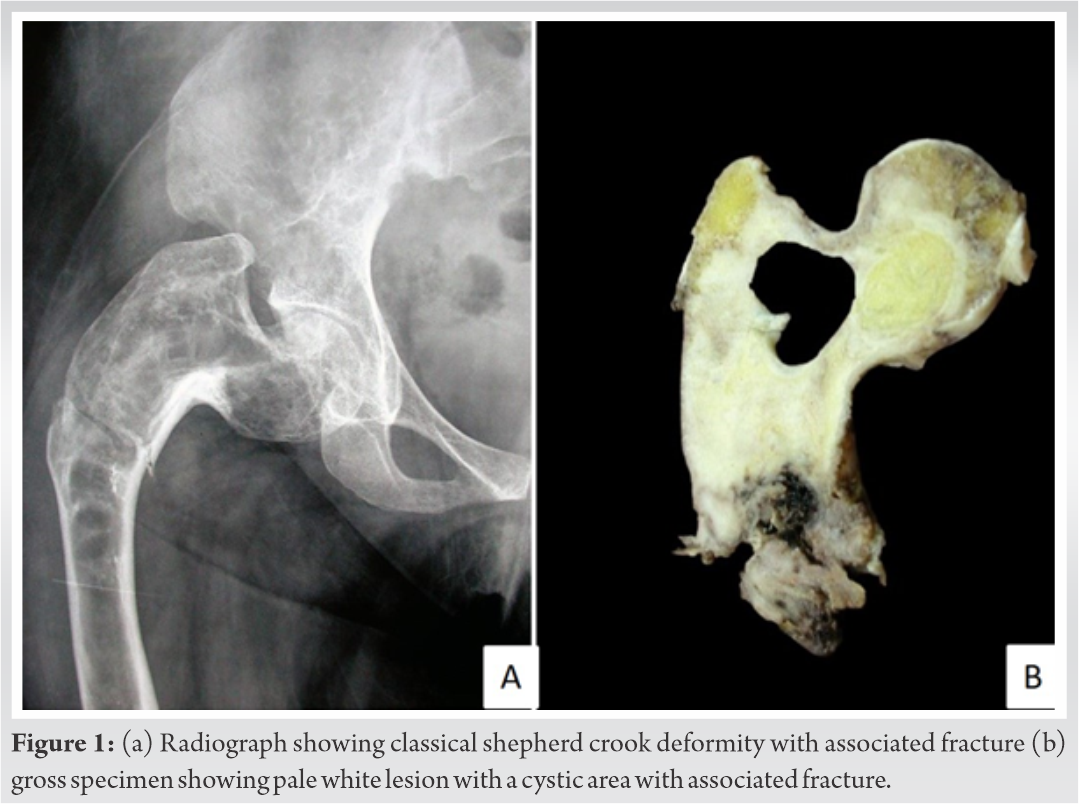

Microscopically, typical areas of fibrous dysplasia areas with scattered irregular woven trabeculae with no osteoblastic rimming against a background of spindle cell stroma were noted in all cases. This component was closely juxtaposed to a cartilaginous component which varied from 25% to 80% of the tissue. Well demarcated islands of hyaline cartilaginous with few interdigitating extensions in the adjacent stroma were noted. The cartilaginous component was predominantly hypocellular except for two cases exhibiting focal hypercellularity with infrequent binucleation of chondrocytes. Many of these chondroid nodules showed peripheral calcification and ossification with osteoblastic rimming. Epiphyseal growth plate like areas with chondrocytes arranged in long columns was noted in three cases. Photomicrographs of the histology are shown in (Fig. 2). Clinical follow of all the patients did not reveal any recurrence at follow-up. The clinical details of all the patients are summarized in (Table 1).
Fibrous dysplasia may rarely exhibit cartilaginous differentiation, which may range from rare microscopic focus to grossly or radiologically evident large areas. The percentage of the cartilaginous component varies and no cutoff has been proposed as to when these should be termed FCD rather than FD. Florid fibrocartilaginous dysplasia is the extreme end of spectrum of FD with cartilaginous differentiation. Radiological and histopathological findings in such cases may mimic cartilaginous neoplasms, causing a diagnostic dilemma [2,3,4]. Fibro chondrodysplasia was the term proposed by Pelzmann et al. for these cases of fibrous dysplasia with prominent cartilaginous component [5]. The term has been replaced and is now called fibrocartilaginous dysplasia. Kyriakos et al. in their review article state that FCD may occur at any age ranging from 3 to 66 years with a mean of 18.3 years. There is slight male preponderance as compared to FD, where there is no gender predilection. They have been reported in both polyostotic and monostotic cases. Some studies have reported its frequent occurrence in monostotic cases and others in polyostotic cases. The femur is the most common location that has been reported. FCD often presents with pain, a mass, or deformities of the limb [2]. There are many hypotheses regarding the origin of the cartilaginous islands. Sankerin et al. proposed that they arise from the developmental rests at the epiphyseal growth plate [4]. This concept is supported by the fact that these cartilaginous nodules often show peripheral enchondral ossification with osteoblastic rimming, unlike the adjacent metaplastic bone of fibrous dysplasia. Areas resembling epiphyseal growth plates are often noted. They suggested that these grow simultaneously with fibrous dysplasia, rather than being part of the lesion itself. This hypothesis is further supported by a study done by Scherer et al., who found incidental cartilage in the femur in 20 of 1125 autopsies [6]. However, this does not explain the origin of FCD in calvarial and vertebral bones where there are no growth plates. In the femoral neck region, the trochanteric growth plate may also be the origin of these cartilaginous areas [7]. Lichtenstein and Jaffe proposed that the cartilaginous areas are an integral part of the dysplastic process and arise by stromal metaplasia [8]. Some authors believe that the cartilaginous nodules arise from displaced cartilage from prior fracture site callus [9]. Radiologically, fibrous dysplasia is usually a well-defined expansile lesion involving the medullary cavity, often with cortical thinning. The density of the tumor varies depending on the relative proportions of fibrous, cartilaginous, and osseous tissue. Soft-tissue extension is not seen. In long standing cases, the bone is markedly expanded causing extreme bowing and angulation, resulting in a classical shepherd crook’s deformity [10]. While FCDs resemble fibrous dysplasia radiologically, the associated cartilaginous foci have dot like, ring like (annular), or floccular calcifications. If the cartilaginous component is extensive, a cartilaginous neoplasm may be mimicked radiologically [2]. Histologically, there is an admixture of typical areas of fibrous dysplasia and hyaline cartilaginous nodules. The cartilaginous areas are often well delineated with peripheral calcification and enchondral ossification and demonstrate scattered chondrocytes lacking atypia with rare binucleation [2]. Occasionally foci resembling epiphyseal growth plates are observed. Molecular studies have shown that fibrous dysplasia is caused by postzygotic missense mutations of GNAS1 gene [11] and is now being incorporated in the diagnostic workup of fibro-osseous lesions. However, its significance in FCD has not been well studied, there being a single case report of FCD with GNAS mutations [12]. These lesions may mimic various cartilaginous neoplasms radiologically and histologically. The main differentials that are considered are enchondroma, low grade chondrosarcoma, dedifferentiated chondrosarcoma, and fibrocartilaginous mesenchymoma. Enchondroma is a consideration especially in small biopsies where FD areas are not sampled. However, the presence of epiphyseal growth plate like areas with enchondral ossification should raise a suspicion of FCD. FCD may rarely show binucleated chondrocytes, thereby raising concern for a low-grade chondrosarcoma. Lack of atypia with absence of a soft-tissue component may help in separating the two entities. Rarely the spindle cell areas next to cartilaginous nodules may mimic a dedifferentiated chondrosarcoma. However, absence of high-grade cellular areas with marked nuclear pleomorphism will exclude dedifferentiated chondrosarcoma. The main differential diagnosis is fibrocartilaginous mesenchymoma which shows significant overlap with FCD clinically, histologically, and radiologically. This is a benign tumor with locally aggressive behavior. Radiologically, they resemble FCD except for some cases showing soft-tissue extension. Histologically, they show cartilaginous nodules within a spindle celled stroma and the cartilaginous areas are similar to FCD with enchondral ossification. Unlike FCDs, however, the stroma is compact and hypercellular with elongated hyperchromatic spindle cells. They may even show mild nuclear atypia [13]. Finally, FCDs should not be confused with focal fibrocartilaginous dysplasia which is a dysplastic process of long bones causing angular deformity in children. It has been suggested that there is failure in mesenchymal differentiation at the region of pes anserinus, resulting in excessive fibrocartilage, which interferes with local bone growth [14].
FCD with abundant cartilage can lead to extreme deformity with attendant significant therapeutic problems. Early treatment is required, as they often predispose the bone for pathological fracture. Treatment is similar to that of FD, often surgical with curettage and bone grafting or osteotomy with internal fixation. Rarely en bloc resection can be done for cases with extreme deformities [2,3,4,7]. Malignancy arising from fibrous dysplasia has been rarely reported, especially osteosarcoma and fibrosarcoma [15]. However, review of literature suggests a benign course of FCD with no reported recurrences or malignancies. Kyriakos et al. in their review article suggested that since cartilage has been in reported in fibrous dysplasia in varying amounts in many cases, fibrocartilaginous dysplasia probably represents the extreme end of cartilaginous differentiation in FD, rather than a distinct entity [2].
FCD is a rare variant of fibrous dysplasia and its distinction from other benign or malignant cartilaginous neoplasms is important. The location and radiology coupled with the biphasic histology enables the alert observer to recognize this entity in curetting’s; though in a needle or small biopsies the presence of only the cartilaginous component could create diagnostic difficulties. Awareness of the entity and radiological correlation helps prevent misdiagnosis.
These five cases are being reported to create greater awareness among pathologists of a rare variant of a common disorder. The histopathological differentiation from other cartilaginous neoplasms is crucial as the treatment is often conservative surgical intervention.
References
- 1.Antonescu C. Soft Tissue and Bone Tumours. Lyon: International Agency for Research on Cancer; 2020. [Google Scholar | PubMed]
- 2.Kyriakos M, McDonald DJ, Sundaram M. Fibrous dysplasia with cartilaginous differentiation (“fibrocartilaginous dysplasia”): A review, with an illustrative case followed for 18 years. Skeletal Radiol 2004;33:51-62. [Google Scholar | PubMed]
- 3.Morioka H, Kamata Y, Nishimoto K, Susa M, Kikuta K, Horiuchi K, et al. Fibrous dysplasia with massive cartilaginous differentiation (fibrocartilaginous dysplasia) in the proximal femur: A case report and review of the literature. Case Rep Oncol 2016;9:126-33. [Google Scholar | PubMed]
- 4.Sanerkin NG, Watt I. Enchondromata with annular calcification in association with fibrous dysplasia. Br J Radiol 1981;54:1027-33. [Google Scholar | PubMed]
- 5.Pelzmann KS, Nagel DZ, Salyer WR. Case report 114. Skeletal Radiol 1980;5:116-8. [Google Scholar | PubMed]
- 6.Scherer E. Exostosen, enchondrome und ihre beziehung zum periost, Frankfurt. Ztschr F Path 1928;36:587-605. [Google Scholar | PubMed]
- 7.Muezzinoglu B, Oztop F. Fibrocartilaginous dysplasia: A variant of fibrous dysplasia. Malays J Pathol 2001;23:35-9. [Google Scholar | PubMed]
- 8.Lichtenstein L, Jaffe HL. Fibrous dysplasia of bone. Arch Pathol 1942;33:777. [Google Scholar | PubMed]
- 9.Prasad HK, Sajjan N, Mathias L, Shetty K, Rao C, Kaliyath S. Fibrocartilagenous dysplasia: A rare variant of fibrous dysplasia. J Orthop Allied Sci 2015;3:37. [Google Scholar | PubMed]
- 10.Fitzpatrick K, Taljanovic M, Speer D, Graham A, Jacobson J, Barnes G, et al. Imaging findings of fibrous dysplasia with histopathologic and intraoperative correlation. Am J Roentgenol 2004;182:1389-98. [Google Scholar | PubMed]
- 11.Jour G, Oultache A, Sadowska J, Mitchell T, Healey J, Nafa K, et al. GNAS mutations in fibrous dysplasia: A comparative study of standard sequencing and locked nucleic acid PCR sequencing on decalcified and nondecalcified formalin-fixed paraffin-embedded tissues. Appl Immunohistochem Mol Morphol 2016;24:660-7. [Google Scholar | PubMed]
- 12.Henderson E, Monforte H, Neustadt J. Fibrocartilaginous dysplasia of the proximal part of the femur with a pathological fracture in a child. JBJS Case Connector 2014;4:e90. [Google Scholar | PubMed]
- 13.Bulychova IV, Unni KK, Bertoni F, Beabout JW. Fibrocartilagenous mesenchymoma of bone. Am J Surg Pathol 1993;17:830-6. [Google Scholar | PubMed]
- 14.Pavone V, Testa G, Riccioli M, Sessa A, Evola FR, Avondo S. The natural history of focal fibrocartilaginous dysplasia in the young child with tibia vara. Eur J Orthop Surg Traumatol 2014;24:579-86. [Google Scholar | PubMed]
- 15.Ruggieri P, Sim FH, Bond JR, Unni KK. Malignancies in fibrous dysplasia. Cancer 1994;73:1411-24. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2021 Bilateral Traumatic Nightstick Fracture of the Ulna – A Rare Case Report and Review of the Literature
July 10, 2021 Bilateral Traumatic Nightstick Fracture of the Ulna – A Rare Case Report and Review of the Literature November 10, 2023 Ipsilateral Knee Dislocation and Ankle Fracture Dislocation
November 10, 2023 Ipsilateral Knee Dislocation and Ankle Fracture Dislocation March 10, 2022 Biceps Femoris Tendon Subluxation Snapping Knee, Treated by a Modified Kennedy Procedure: A Case Report
March 10, 2022 Biceps Femoris Tendon Subluxation Snapping Knee, Treated by a Modified Kennedy Procedure: A Case Report August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy
August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy