
Aneurysmal bone cysts can lead to pathological fractures, which require stabilization with internal fixation in weight bearing bones. Extended curettage decreases the rate of recurrence.
Dr. Satvik N Pai, Department of Orthopaedic Surgery, Sri Ramachandra Medical College and Research Institute, Chennai - 600 116, Tamil Nadu, India. E-mail: satvik.pai@gmail.com
Abstract
Introduction: Aneurysmal bone cyst (ABC) is a rare, benign, and cystic lesion. The most common sites are the femur, tibia, humerus, and spine. It is more common in females and usually occurs during the second decade of life.
Case Report: A 5-year-old female child had a trivial fall, following which she developed pain in her left hip. Radiographs revealed an expansile, lytic lesion in the metaphysis of the left proximal femur. Cortical breach was present resulting in a pathological fracture. Biopsy of the lesion showed blood filled cystic spaces confirming the diagnosis of ABC. We performed an extended curettage of the lesion, bone grafting, and angle blade plate fixation. The angle blade plate was removed 1 year after the surgery. Two years later, she complained of pain in the left hip. Radiographs showed a geographic lytic lesion surrounding the previously inserted bone graft. Magnetic resonance imaging revealed multiple blood fluid levels. We performed an extended curettage with high speed burr. We filled the cavity with bone substitute and stabilized the region using a proximal humerus internal locking system plate. The histopathological examination of intraoperative samples confirmed the diagnosis of recurrence of ABC. We found no further recurrence of the tumor after 3 years of follow-up.
Conclusion: ABCs can present with pathological fractures and requires management of the cyst and stabilization of the bone. Recurrent ABCs can be managed by re-curettage of the lesion and prophylactic internal fixation. The curettage has to be extensive through a large cortical window and using a high speed burr.
Keywords: Aneurysmal bone cyst, recurrence, pathological fracture, treatment.
Aneurysmal bone cyst (ABC) is a rare, benign, blood filled, and cystic lesion. It occurs in approximately 1.4 individuals/10,000 population/year and accounts for 9.1% of all bone tumors [1]. The most common sites are the distal femur, proximal tibia, proximal humerus, and spine. It is more common in females and usually occurs during the second decade of life [2]. ABC is known to have a chance of recurrence after treatment [3]. We report a case of recurrent ABC which managed by recurettage and internal fixation.
A 5-year-old female child had a trivial slip and fall and complained of pain in her left hip following the fall. She was unable to bear weight over the left lower limb following the fall. On examination, she was found to have swelling and tenderness over the left hip. Radiographs revealed an expansile, lytic lesion in the metaphysis of the left proximal femur. Trabeculations were visible within the lesion. Cortical breach was present resulting in a pathological fracture. The child underwent a biopsy of the lesion, which showed anastomosing cavernous areas lined by fibrous tissue and filled with blood. A diagnosis of ABC was made. It was classified as stage 3 (aggressive) as per Enneking’s staging of benign musculoskeletal neoplasms. We performed an extended curettage of the lesion, bone grafting, and angle blade plate fixation. The child was followed up regularly and the fracture was radiologically found to have healed completely. The angle blade plate was removed 1 year after the surgery.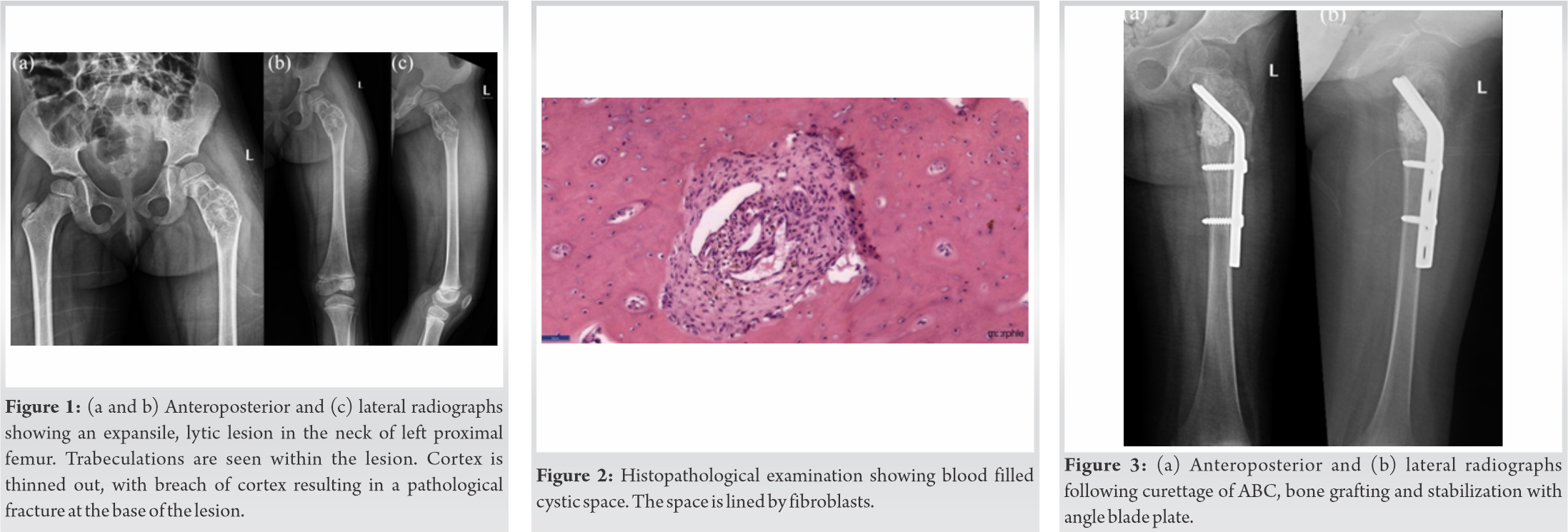
Two year following the curettage surgery, child complained of pain in the left hip for 2 months. The pain was insidious in onset, dull aching type, non-radiating, and gradually progressive. On examination, the scar from the previous surgery was found to have healed completely and there were no other significant findings. She had painless, full range of movements of the left hip joint. There was no limb length discrepancy compared to the contralateral limb. Radiographs showed an eccentrically located, geographic lytic lesion in the metaphysis of proximal femur surrounding the dense opacity of the previously inserted bone graft. Pattern of destruction could be identified as Lodwick pattern IB. Cortical thinning and periosteal scalloping were noted in the lesion. There was a narrow zone of transition. Cortex was found to be intact and there was no periosteal reaction. Magnetic resonance imaging (MRI) revealed a well-defined lobular lesion in the metaphysis of proximal femur extending into the diaphysis, and measuring 5.8 × 3.3 × 2.8 cm. Multiple blood fluid levels were noted. Thin incomplete septations were also noted. It was diagnosed to be a recurrence of ABC. We then performed an extended curettage, creating a large cortical window, and performed curettage with high speed burr and thermal cauterization of the lesion. We also augmented the curetted lesion with bone substitute. We stabilized the region using a proximal humerus internal locking system (PHILOS – Depuy Synthes® Switzerland) plate and screws as the pediatric proximal femur locking plate was unavailable at the time. The histopathological examination of intraoperative samples confirmed the diagnosis of recurrence of ABC. We followed up the child for 3 years and found no further recurrence of the tumor. She was walking unaided and had full range of the movement of the left hip joint.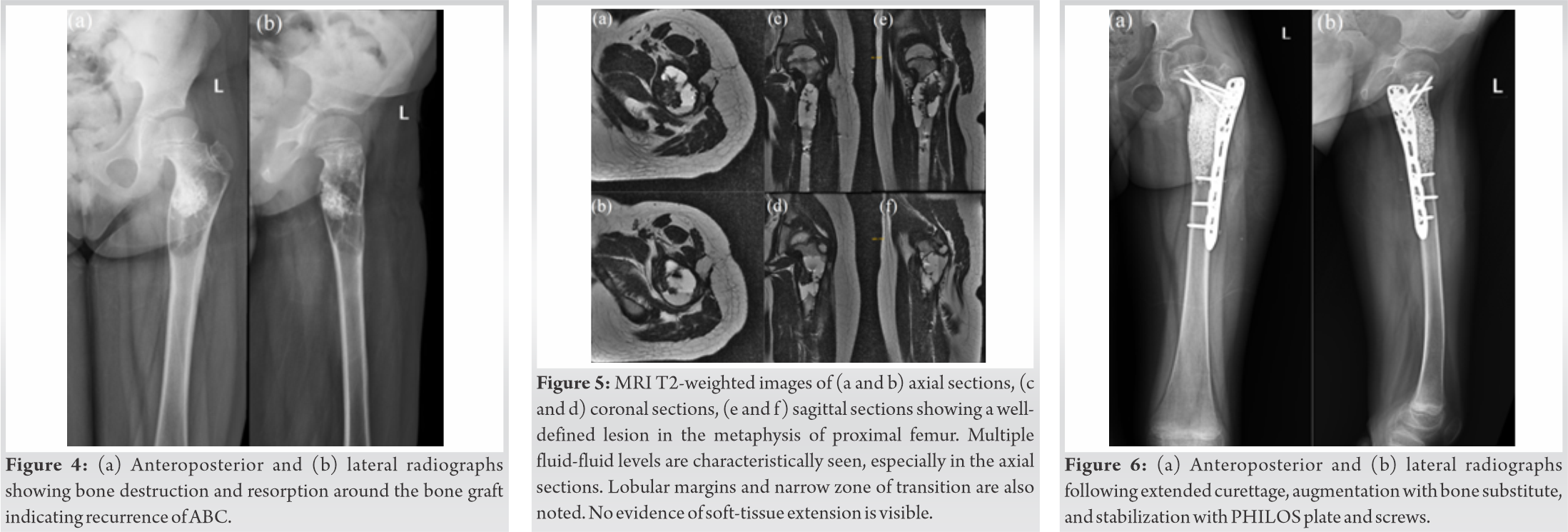
ABCs is a hemorrhagic bone tumor. In 70% of the cases, it arises de novo and is called primary ABC. In 30% of the cases, it occurs in underlying bone tumors and is called secondary ABC [4]. Insidious pain is the most common symptom. Swelling and tenderness in the region of the tumor may be present. Radiographs reveal a lytic, expansile lesion, located eccentrically in the metaphyseal region of bones. MRI shows the lesion to have multiple fluid levels and septations [5]. The diagnosis should always be confirmed with a biopsy.
ABCs cause erosion and resorption of involved bone. They can, thus, lead to pathological fractures [6]. Pain, younger age of presentation, change in the size of a cavity with age, multiple septations, and early recurrence are signs of an active cyst and have increased fracture risk [7]. When a pathological fracture occurs, the treatment is required for the cyst as well as the fracture. Primary fixation of pathological fractures in children should be avoided until a histological diagnosis is obtained. Unstable fractures and fractures in weight-bearing bones require internal fixation of the fracture [8]. Fracture fixation for pathological fractures associated with ABC in proximal femur has been described with dynamic hip screw [9], plate osteosynthesis [10], dynamic condylar screw plate system [11], or intramedullary fixation like ender’s nail [12]. We performed a closed, core needle biopsy under fluoroscopic guidance. Only after confirmation of histological diagnosis, we went ahead with the definitive treatment of the lesion with extended curettage of the lesion and bone graft augmentation. We stabilized the fracture with a 4 holed, 135 degree angle blade plate. ABCs are known to recur after treatment in approximately 10% of the cases. Age <15 years, central location, and incomplete removal of the cyst cavity are risk factors for recurrence [7]. Proximal femur ABCs are proposed to have a higher risk of recurrence [3]. Intralesional curettage, with or without bone grafting, is the standard treatment for ABCs [13]. Supplemental use of adjuvants such as high-speed burr, argon beam coagulation, phenol, and cryotherapy is termed as extended curettage and has been shown to decrease the rate of recurrence [14]. En block resection has a lower recurrence rate but is associated with significantly greater morbidity. In our case, when the tumor was found to have recurred, we choose performed an extended curettage using a high speed burr and cauterized all the walls of the curetted cavity. We filled the cavity with bone substitute constituting of 60% hydroxyapatite and 40% tricalcium phosphate. The cavity created was significantly larger than the first surgery; hence, we stabilized the region using a PHILOS plate. We believe that the successful treatment with extended curettage with the absence of recurrence demonstrated that extended curettage produces satisfactory results without requiring en bloc excision, even for cases of recurrent ABC.
ABCs can present with pathological fractures and requires management of the cyst and stabilization of the bone. Recurrent ABCs can be managed by recurettage of the lesion and prophylactic internal fixation. The curettage has to be extensive through a large cortical window and using a high speed burr.
ABCs can lead to pathological fractures. Such pathological fractures in weight-bearing bones require stabilization with internal fixation. Extended curettage decreases the rate of recurrence.
References
- 1.Cottalorda J, Bourelle S. Current treatments of primary aneurysmal bone cysts. J Pediatr Orthop B 2006;15:155-67. [Google Scholar | PubMed]
- 2.Stevens KJ, Stevens JA. Aneurysmal Bone Cysts. In: StatPearls Treasure Island, FL: StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546654 [Last accessed on 2020 Sep 05]. [Google Scholar | PubMed]
- 3.Mohaidat ZM, Al-Gharaibeh SR, Aljararhih ON, Nusairat MT, Al-Omari AA. Challenges in the diagnosis and treatment of aneurysmal bone cyst in patients with unusual features. Adv Orthop 2019;2019:2905671. [Google Scholar | PubMed]
- 4.Mascard E, Gomez-Brouchet A, Lambot K. Bone cysts: Unicameral and aneurysmal bone cyst. Orthop Traumatol Surg Res 2015;101:S119-27. [Google Scholar | PubMed]
- 5.Zishan US, Pressney I, Khoo M, Saifuddin A. The differentiation between aneurysmal bone cyst and telangiectatic osteosarcoma: A clinical, radiographic and MRI study. Skeletal Radiol 2020;49:1375-86. [Google Scholar | PubMed]
- 6.Dormans JP, Pill SG. Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-67. [Google Scholar | PubMed]
- 7.Subramanian S, Kemp AK, Viswanathan VK. Bone cyst. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2020. [Google Scholar | PubMed]
- 8.Jackson WF, Theologis TN, Gibbons CL, Mathews S, Kambouroglou G. Early management of pathological fractures in children. Injury 2007;38:194-200. [Google Scholar | PubMed]
- 9.Lin J, Chen R, Yan W, Zhang Y, Chen D. Treatment of benign bone lesions of proximal femur using dynamic hip screw and intralesional curettage via Watson-Jones approach. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2018;32:31-5. [Google Scholar | PubMed]
- 10.Tomaszewski R, Rutz E, Mayr J, Dajka J. Surgical treatment of benign lesions and pathologic fractures of the proximal femur in children. Arch Orthop Trauma Surg 2020;142:615-24. [Google Scholar | PubMed]
- 11.Purohit S, Raja BS, Marathe NA, George PK. A case report of aneurysmal bone cyst with pathologic fracture of proximal femur managed with enblocexcision and autologous non-vascularized fibular graft. J Orthop Case Rep 2019;10:51-3. [Google Scholar | PubMed]
- 12.Kapoor C, Shah M, Soni R, Patwa J, Merh A, Golwala P. Aneurysmal bone cyst of the proximal femur and its management-a case report. Cureus 2017;9:e991. [Google Scholar | PubMed]
- 13.Grahneis F, Klein A, Baur-Melnyk A, Knösel T, Birkenmaier C, Jansson V, et al. Aneurysmal bone cyst: A review of 65 patients. J Bone Oncol 2019;18:100255. [Google Scholar | PubMed]
- 14.Park HY, Yang SK, Sheppard WL, Hegde V, Zoller SD, Nelson SD, et al. Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9:435-44. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Percutaneous Tenotomy for Chronic Tennis Elbow: A Minimally Invasive Technique with Better Outcomes – A Case Series
February 10, 2024 Percutaneous Tenotomy for Chronic Tennis Elbow: A Minimally Invasive Technique with Better Outcomes – A Case Series June 21, 2021 Metastatic Adenocarcinoma of Lungs, Mimicking Primary Scapular Tumor: A Case Report and Review of Literature
June 21, 2021 Metastatic Adenocarcinoma of Lungs, Mimicking Primary Scapular Tumor: A Case Report and Review of Literature November 1, 2024 Resistant and Refractory Distal Tibia Non-Union Using an Intramedullary Free Fibular Graft and Ilizarov Fixation – An Illustrative Case Report
November 1, 2024 Resistant and Refractory Distal Tibia Non-Union Using an Intramedullary Free Fibular Graft and Ilizarov Fixation – An Illustrative Case Report October 10, 2022 Intra-articular osteoid osteoma of the hip mimicking as monoarthritis-A case report
October 10, 2022 Intra-articular osteoid osteoma of the hip mimicking as monoarthritis-A case report