
A wide differential diagnosis should be considered when rapid bone loss is observed, as inflammation or infection can be great mimickers of other diseases.
Dr. Valentin Antoci, Department of Orthopedic Surgery, University Orthopedics Inc., East Providence, Rhode Island, United States. E-mail: valentin.antoci@gmail.com
Abstract
Introduction: Knee pain and osteoarthritis are frequent patient complaints, with a rapidly increasing prevalence. By comparison, the prevalence of rheumatoid arthritis (RA) is significantly lower at around 1%. Inflammatory arthropathies, like RA, are difficult to differentiate from infection, crystal arthropathies, or malignancy. In addition, radiography and roentgenograms are often inconclusive or non-specific, making it much more difficult to evaluate, diagnose, and manage this condition. The current case is unique due to its location in the knee joint, rather than more common presentations in the upper extremities, and use of MRI imaging for diagnosis of RA with tenosynovitis.
Case Report: In a Caucasian 70-year-old female with sudden debilitating knee pain and a large atraumatic defect over tibial plateau, MRI showed a large fluid collection within the left gracilis muscle. Gram stain and culture of the aspirate remained negative. The only significant history involved a possible diagnosis of RA.
Conclusion: While rheumatoid tenosynovitis is common in the upper extremities, lower extremity features have not been well reported before. We diagnosed the patient with progressive RA and rheumatoid tenosynovitis. This unique presentation and rare usage of MRI imaging may be contributing to an underreporting of this diagnosis in the lower extremities.
Keywords: Rheumatoid arthritis, knee, adult reconstruction, total joint arthroplasty.
Musculoskeletal pain affects every single person, at 1 time or another, throughout their life. Knee pain accounts for over 2 million primary care visits annually, involving 6% of patients in the office [1]. The prevalence of knee pain is on the rise, with several studies suggesting a 2–4-fold increase over the past 20 years [2]. The most common diagnoses in orthopedic offices include osteoarthritis (24%), meniscus injuries (11%), ligamentous injuries (14%), and fractures (7%) [1]. Radiography and roentgenograms are often inconclusive or non-specific, while physical examination maneuvers can be technically demanding and dependent on skill and experience [3]. In addition, inflammatory arthropathies are hard to differentiate from infection, crystal arthropathies, or malignancy. Ultimately, some diagnoses may not be defined until the time of surgery, due to the reliance on direct clinical observation, examination, pathology, and radiography.
A 70-year-old Caucasian woman was admitted to the general orthopedic service with unrelenting knee pain, unable to ambulate. She had a history of juvenile idiopathic arthritis, rheumatoid factor negative rheumatoid arthritis (RA), psoriasis, osteoporosis, fibromyalgia, and recurrent deep perioperative infections. Her pain was progressive over the past 8 months, with acutization over the past 4–6 weeks. She was seen 8 months previously by a hip and knee reconstructive surgeon in the setting of knee pain and concern for arthritis. At that time, she showed Kellgren–Lawrence grade 3 arthritic changes with about 25–50% loss of joint space, subchondral sclerosis, and osteophytosis (Fig. 1a). Her body mass index is 18.7 kg/m2. She thought and she has some kind of inflammatory arthritis but had not received a definite diagnosis in the past.
Eight months later, her symptoms are different; she was admitted to the hospital with pain and swelling in her left thigh. Her symptoms were significant enough over the past week that she had been largely bedridden and dependent on another person’s assistance. Her physical examination was positive for a systolic heart murmur, as well as decreased range of motion, tenderness, swelling, pain, and deformity at multiple sites including her back, hands, hips, feet, and shoulders. The same day, her left knee had significant swelling with medial synovial thickening at the bursa with no clear free flowing effusion and tenderness, while her right knee appeared normal. Overall, she displayed diffuse symmetric muscle atrophy and an abnormal gait. She was seen by her primary care physician with a concern for deep venous thrombosis and preemptively started on anticoagulation medication. A subsequent ultrasound revealed only thrombosis within the left posterior tibial vein and no evidence of deep vein thrombosis. New radiographs revealed significant bone loss with a 1.5 cm depression over medial tibial plateau (Fig. 1b). The patient denied any recent trauma or falls. Full workup including inflammatory markers revealed an erythrocyte sedimentation rate of 1 mm/h and C-reactive protein of 0.52 mg/L. Peripheral white count was 6,900 cells/mL and hemoglobin was 8.3 g/dL, with significant chronic anemia. Immunological laboratory work and other testing are shown in Table 1. An MRI of the thigh was then obtained (Fig. 2) and was read as a large, T2 hyperintense, and rim-enhancing fluid collection centered within the left gracilis muscle, which extended from the level of the mid femur to the knee, measuring approximately 13.4 cm × 2.2 cm × 2.3 cm, with adjacent muscular edema and enhancement. Radiology concluded that the patient had a large intramuscular abscess centered within the left gracilis muscle, with associated myositis and overlying subcutaneous cellulitis. A subsequent ultrasound guided aspiration then showed over 2 million red blood cells, 49,500 nucleated cells, and a 73% neutrophil count. Gram stain showed no organisms present and culture ultimately came back negative. After extensive discussion with the multiple consulting services, the new diagnosis was progressive RA with rheumatoid tenosynovitis, unlikely to be infectious. Considering the patient’s limited ambulatory status, significant pain, and discomfort, a shared decision to proceed with early total knee arthroplasty was taken. During surgery, a standard medial parapatellar approach was conducted. The medial condyle was significantly eroded, especially laterally, with varus collapse (Fig. 3). The patient had extensive synovitis in the suprapatellar pouch and both medial and lateral gutters. The tibia showed a large defect and collapse with overall poor bone quality. Pathology identified extensive villous hypertrophy (Fig. 4a) with histiocytic and lymphoplasmacytic reactions (Fig. 4b) consistent with acute on chronic inflammatory processes. No malignancy was reported.
After appropriate bone cuts and balance of soft tissues, the knee was reconstructed with the primary posterior stabilized total knee arthroplasty components (Fig. 5). To address the contracted medial structures, the deep medial collateral ligament was raised subperiosteally from the bone, exposing it to the posterior aspect of the tibia. The medial bone defect was reconstructed with a 10 mm metal augment. A cemented tibial stem was used to compensate for poor bone quality and improve component support. The femur was cut in 5° of valgus, which is standard for our technique. The patella was resurfaced with a three-peg cemented polyethylene button.
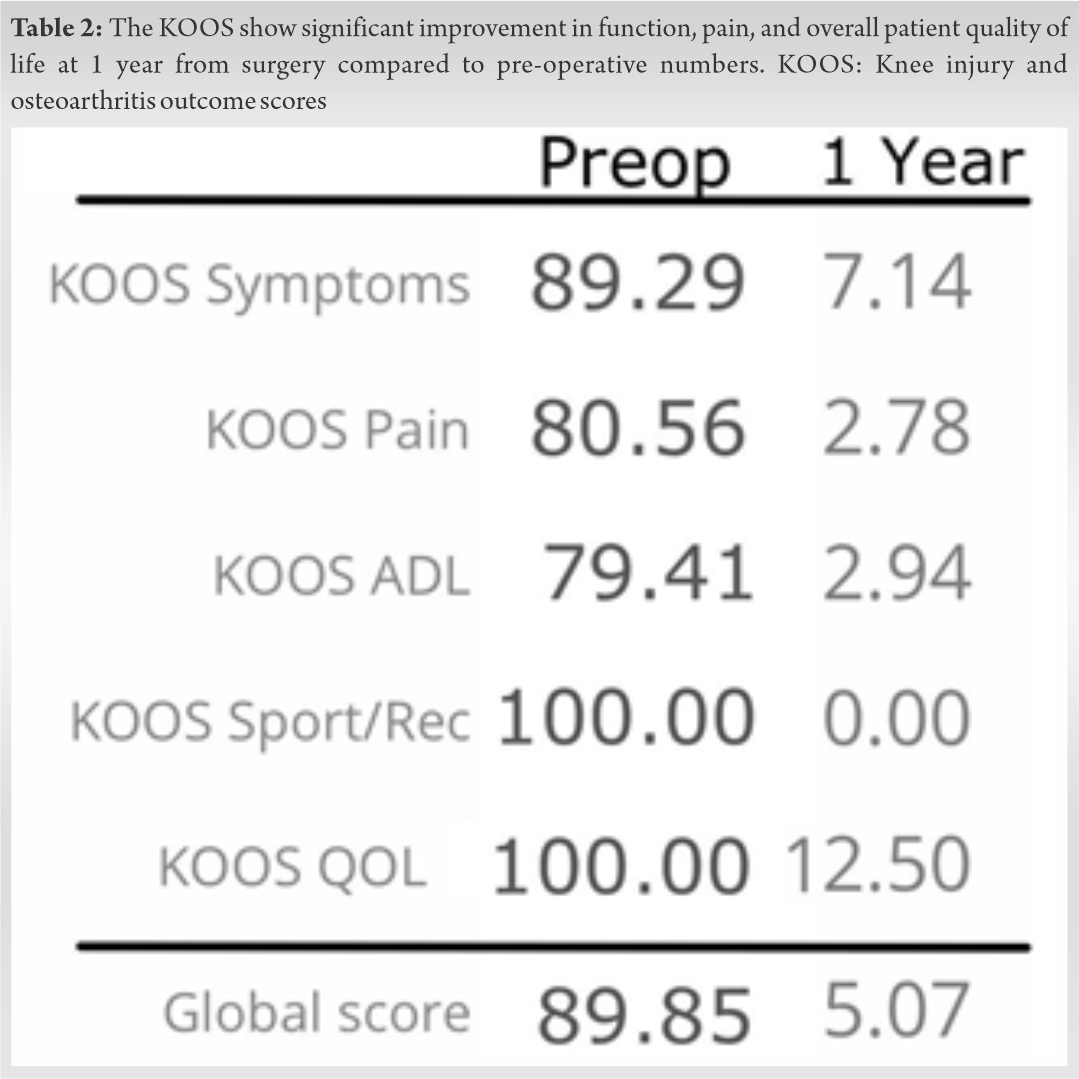
The patient tolerated the procedure without any perioperative complications, was ambulatory the same day with physical therapy, and was discharged to her home on post-operative day 2. One year from surgery, she is independent, happy with the overall function of the total knee arthroplasty but continues to have generalized joint pain involving all joints, including intermittent effusion in the affected knee. Her knee injury and osteoarthritis outcome score has improved from 89.85 before the surgery to 5.07 at 1 year after the surgery. The improvements were similar across all areas tested, including symptoms, pain, and activities of daily living (Table 2). The patient has given her informed consent to be included in this case report.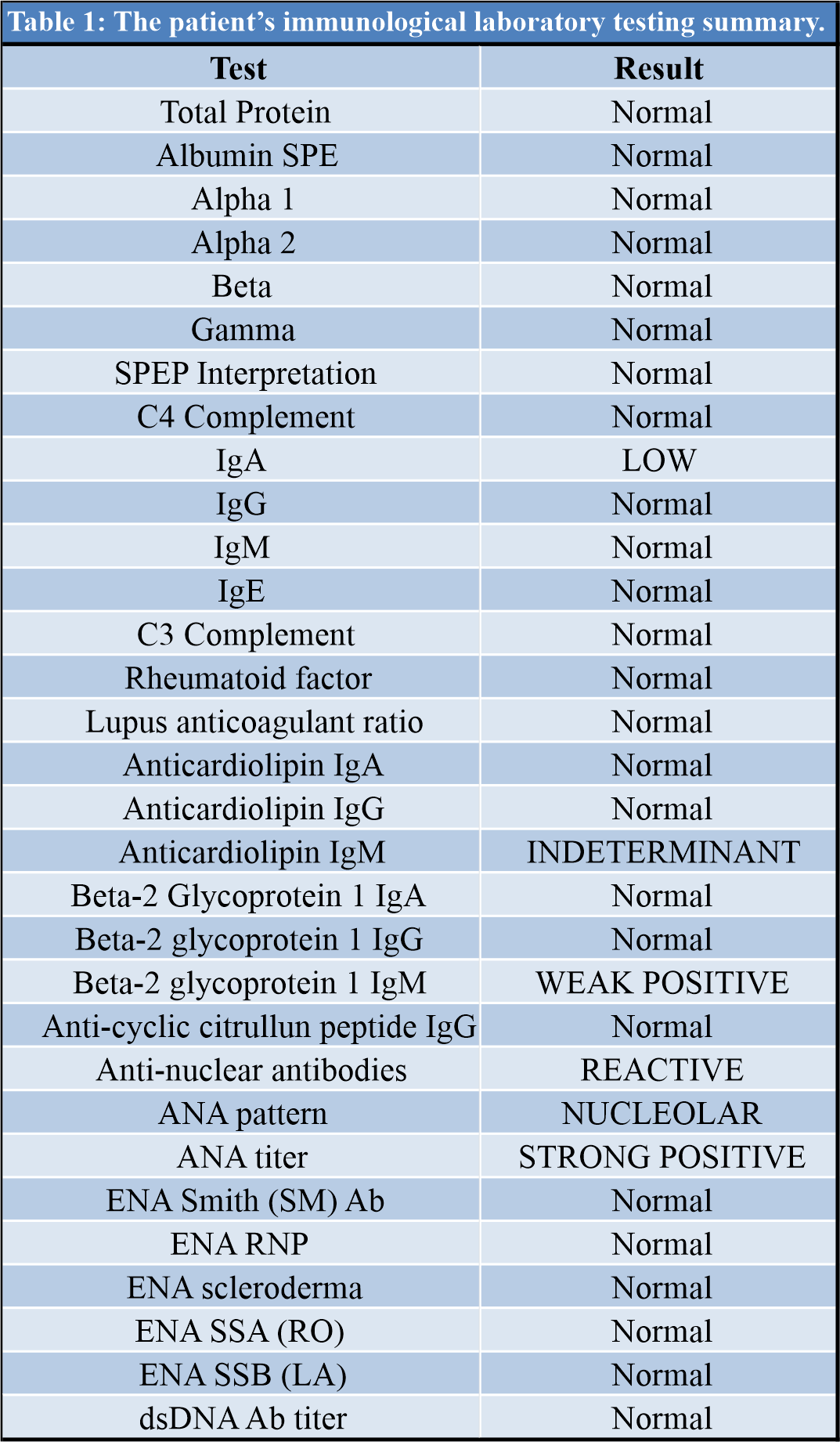
Knee pain is a frequent patient complaint, with a rapidly increasing prevalence. The lifetime risk of developing knee osteoarthritis is 40% in men and 47% in women. Obesity doubles the risk compared to normal weight or underweight individuals, with rates as high as 60.5% prevalence [4]. Average medical charges for osteoarthritis were estimated to be around $2,600/year in 1997 and had ballooned to over $5,700 in 2000 [4]. From 1991 to 2004, the number of knee arthroplasties performed has tripled, with close to 500,000 surgeries performed in 2004, costing more than 14 billion dollars [4]. By comparison, the prevalence of RA is only 0.5–1.1%, which makes it much more difficult to evaluate, diagnose, and manage [5]. RA is an inflammatory arthropathy that causes synovitis and leads to joint damage and bone destruction. The hypothesis behind RA is based on an autoimmune premise, where antibodies specific for IgG, also called rheumatoid factors, cause an inflammatory response and destruction of cartilage and joint [6]. However, the presence of rheumatoid factors can precede the clinically detectable onset of inflammatory arthritis for years without symptoms or interventions. In the interim, the joint can deteriorate and rapidly progress toward the need for total joint arthroplasty. Ultimately, the diagnosis of progressive arthritis and management often derives from imaging to visualize the degree of joint space deterioration. Larsen et al. introduced six stages to clearly differentiate between the previously described Stages II and III [7]. They proposed grade 0 as a normal joint up to grade 5 as complete loss of articular surface and gross bone deformity. Over a short period of 6 months, the patient started with a grade 2 image and later showed complete loss of articular surface with the collapse of the tibia and gross deformity. Furthermore, the deformity now presents with significant bone loss and likely change in ligamentous balance. Literature searches did not reveal any previous reports of such findings in the knee joint. Rheumatoid synovitis is common in the upper extremity and has been described in the wrist and forearms [8,9]. The first report of rheumatoid tenosynovitis was presented by Jacobs et al. in a case of a 41-year-old woman with progressive swelling of the back of her right hand [10]. The pathology described is similar to the current case presented and shows villous hypertrophy and lymphocytic infiltration (Fig. 4). Hamstring tenosynovitis has been described previously as a result of friction in the semimembranosus groove, usually relieved by steroid injections or surgical release [11,12]. Nevertheless, the described symptoms involve “snapping knee” rather than thigh pathology [13]. Other conditions such as pigmented villonodular synovitis can cause progressive tenosynovitis but are less likely to progress proximally along the hamstring or have the imaging seen in the current case (Fig. 2) [14].
The current case is unique in its presentation and has not been reported previously. Rheumatoid tenosynovitis may be affecting more knees than we know and contributing to the significant symptoms of pain in RA. Compared to the wrist or forearm, a similar mass in the thigh would likely be difficult to diagnose due to the deeper location of tendons and the expected swelling and pain around the knee. Eshed et al. suggest the presence of tenosynovitis on MRI as an early marker of RA and propose more widespread use of imaging for diagnosis [15]. Nevertheless, the overall pathophysiology of RA is not well understood, and more studies are needed to define orthopedic indications and management.
The current case is unique and has not been reported previously. RA and tenosynovitis may be affecting more knees than we know and contributing to the significant symptoms of pain in RA.
References
- 1.Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med 2003;139:575-88. [Google Scholar | PubMed]
- 2.Nguyen US, Zhang Y, Zhu Y, Niu J, Zhang B, Felson DT. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann Intern Med 2011;155:725-32. [Google Scholar | PubMed]
- 3.Antoci V Jr., Patel SP, Weaver MJ, Kwon JY. Relevance of adjacent joint imaging in the evaluation of ankle fractures. Injury 2016;47:2366-9. [Google Scholar | PubMed]
- 4.Neogi T, Zhang Y. Epidemiology of osteoarthritis. Rheum Dis Clin N Am 2013;39:1-19. [Google Scholar | PubMed]
- 5.Alamanos Y, Drosos A. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev 2005;4:130-6. [Google Scholar | PubMed]
- 6.McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol 2007;7:429-42. [Google Scholar | PubMed]
- 7.Larsen A, Dale K, Eek M. Radiographic evaluation of rheumatoid arthritis and related conditions by standard reference films. Acta Radiol Diagn 1977;18:481-91. [Google Scholar | PubMed]
- 8.Potter TA, Kuhns JG. Rheumatoid, tenosynovitis; diagnosis and treatment. J Bone Joint Surg 1958;40:1230-5. [Google Scholar | PubMed]
- 9.Cooper HJ, Shevchuk MM, Li X, Yang SS. Proliferative extensor tenosynovitis of the wrist in the absence of rheumatoid arthritis. J Hand Surg 2009;34:1827-31. [Google Scholar | PubMed]
- 10.Jacobs JH, Hess EV, Beswick IP. Rheumatoid arthritis presenting as tenosynovitis. J Bone Joint Surg Br 1957;39:288-92. [Google Scholar | PubMed]
- 11.Melton JK, Memarzadeh A, Dunbar WH, Cross MJ. Semimembranosus tenosynovitis: Diagnosis and management of a commonly missed cause of posteromedial knee pain. Knee 2016;24:305-9. [Google Scholar | PubMed]
- 12.Halperin N, Oren Y, Hendel D, Nathan N. Semimembranosus tenosynovitis: Operative results. Arch Orthop Trauma Surg 1987;106:281-4. [Google Scholar | PubMed]
- 13.Bollen SR, Arvinte D. Snapping pes syndrome. Bone Joint J 2008;90:334-5. [Google Scholar | PubMed]
- 14.Riccio AI, Christoforetti J. Pigmented villonodular synovitis of the pes anserine bursa. J Knee 2007;14:402-7. [Google Scholar | PubMed]
- 15.Eshed I, Feist E, Althoff CE, Hamm B, Konen E, Burmester GR, et al. Tenosynovitis of the flexor tendons of the hand detected by MRI: An early indicator of rheumatoid arthritis. Rheumatology 2009;48:887-91. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 2, 2020 Proximal Femoral Non-unions with Implant In Situ Treated by Revision Osteosynthesis: A Real Challenge
December 2, 2020 Proximal Femoral Non-unions with Implant In Situ Treated by Revision Osteosynthesis: A Real Challenge- July 13, 2013 Pyomyositis of Obturator Muscles: Unusual Late Presentation
 August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series
August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series April 10, 2024 Atlanto-occipital Assimilation with Basilar Invagination and Atlanto-occipital Dislocation Treated by Occipitocervical Fixation: A Rare Case Report
April 10, 2024 Atlanto-occipital Assimilation with Basilar Invagination and Atlanto-occipital Dislocation Treated by Occipitocervical Fixation: A Rare Case Report