
We have experienced two patients who required thoracoscopic hematoma removal after anterior spinal surgery and have concluded that intraoperative care and adequate hemostasis are necessary to avoid complications such as post-operative hemothorax and hemopneumothorax.
Dr. Tomohito Mukaihata, Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1 Inohana, Chuo-ku, Chiba, 260-8670, Japan. E-mail: msa681u@yahoo.co.jp
Abstract
Introduction: We report two cases that required revision surgery with thoracotomy for massive hematoma after anterior kyphorectomy surgery.
Case Report: A woman with significant thoracolumbar kyphosis due to L1 vertebral fracture showed associated vertebral instability and pain resistant to conservative treatment. She underwent surgery for a one-stage anterior kypholectomy with spinal fusion. We performed an extrapleural approach. On the 4th post-operative day, the patient developed respiratory distress with decreased SpO2. Contrast-enhanced computed tomography (CT) revealed a left hemothorax with active bleeding. Revision surgery was performed to arrest the bleeding, and a large hematoma in the thoracic cavity was observed around the intercostal artery just below the skin incision, not around the surgical site. A man suffered from impaired activities of daily living caused by postural abnormalities due to severe kyphosis from vertebral fractures at the L1 and L2 vertebrae. Thus, we performed two-stage kypholectomy surgery. First, we performed posterior fixation with posterior facet resection. Then, corpectomy of the 1st and 2nd lumbar vertebrae through an anterior extrathoracic approach was performed. A CT scan on the 2nd post-operative day showed a massive hemopneumothorax, indicating persistent bleeding, and we performed a revision surgery to open the chest for additional hemostasis. Intraoperative findings showed a large hematoma, including reactive pleural effusion in the subcutaneous, retroperitoneal, and intrathoracic cavities.
Conclusion: We experienced two patients who required thoracotomy hematoma removal after anterior spinal surgery. Intraoperative patronage and adequate hemostasis are necessary to avoid post-operative complications such as hemothorax and hemopneumothorax.
Keywords: Anterior thoracolumbar kyphorectomy, thoracolumbar kyphosis, hemothorax, hematoma.
In cases of severe kyphoscoliosis, anterior reconstructive kyphorectomy surgery with a mesh cage or plate is considered [1,2,3]. Such procedures require treatment of thoracoabdominal organs such as the diaphragm and intercostal arteries, as well as perispinal vascular vessels such as segmental arteries [4]. This may cause intraoperative complications such as massive bleeding if not adequately deployed [5]. These complications are associated with high mortality [6]. Herein, we report two cases that required revision surgery with thoracotomy for massive hematoma after anterior kyphorectomy surgery.
Case 1:
A 73-year-old woman with significant thoracolumbar kyphosis due to L1 vertebral fracture showed associated vertebral instability. She underwent surgery for a one-stage anterior kypholectomy with spinal fusion. We performed an extrapleural approach (resection of the 10th rib, diaphragmatic incision), L1 corpectomy, mesh cage (autologous bone filling) fixation of L1, and interbody fixation of L2/3 (Clydesdale®, Medtronic Sofamor Danek, Minneapolis, MN) followed by anterior plate fixation from the T12 to L3 vertebra (Antares® spinal system, Medtronic Sofamor Danek, Minneapolis, MN) (Fig. 1). The intraoperative hemoglobin (Hb) level showed a gradual decrease due to intraoperative bleeding from the expanded soft tissues and osteotomy site, requiring blood transfusion. A single drainage tube was placed in the retroperitoneal cavity at the end of surgery. On the 4th post-operative day, the patient developed respiratory distress with decreased SpO2 to approximately 93%. Contrast-enhanced computed tomography (CT) revealed a left hemothorax with active bleeding (Fig. 2). Revision surgery was performed to arrest the bleeding, and a large hematoma in the thoracic cavity was observed around the intercostal artery just below the skin incision, not around the surgical site. After reoperation, the patient ambulates well and was discharged without complications and resolution of pain and vertebral instability. At follow-up 2 year after the operation, the patient was well.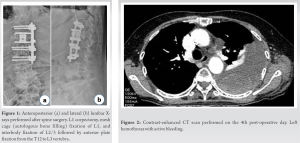
Case 2
A 73-year-old man suffered from impaired activities of daily living caused by postural abnormalities due to severe kyphosis from vertebral fractures at the L1 and L2 vertebrae. Thus, we performed two-stage kypholectomy surgery. In the first stage of surgery, we performed posterior fixation from T8 to S2-alar-iliac with T12-L3 posterior facet resection along with bone grafting using autogenous bone, allogeneic bone, and artificial bone. In the second stage of surgery, corpectomy of the 1st and 2nd lumbar vertebrae through an anterior extrathoracic approach and fixation with a mesh cage (autogenous bone filling) was performed (Fig. 3). During the surgery, the pleura were lacerated by 1 cm followed by an immediate suture. There was a progressive decrease in Hb levels due to intraoperative bleeding, and a continuous blood transfusion was required. After confirming hemostasis, a drain was placed in the retroperitoneal cavity. A CT scan on the 2nd post-operative day showed a massive hemopneumothorax, indicating persistent bleeding (Fig. 4), and we performed a revision surgery to open the chest for additional hemostasis. Intraoperative findings showed a large hematoma, including reactive pleural effusion in the subcutaneous, retroperitoneal, and intrathoracic cavities, but no obvious active bleeding in the retroperitoneal and intrathoracic cavities. We concluded that bleeding from the vertebral body resection site and soft tissues progressed immediately after the surgery. The patient was able to ambulate without difficulty. At follow-up 1 year after the operation, the patient was well.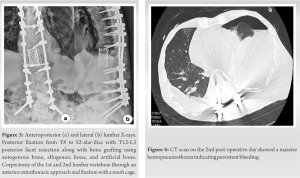
We report two cases of massive post-operative hematoma after thoracolumbar corrective kypholectomy surgery followed by revision open hemostasis surgery. The previous studies have shown that intraoperative complications such as pneumonia, atelectasis, pneumothorax, and pleural effusion have been reported in 13–34% of anterior spine surgery procedures [5,7,8,9,10,11,12]. Among these complications, those affecting the respiratory organs require special attention because they are associated with high mortality [6]. The origin of the hemothorax after anterior thoracolumbar surgery includes epidural vessel rebleeding, bleeding from the osteotomy site, pulmonary parenchymal laceration, and vascular injury. Spontaneous intercostal artery hemorrhage has also been reported, although it is rare [13]. In the present cases, bleeding from the intercostal artery was suspected in Case 1, and bleeding from the osteotomy, including the surrounding soft tissue, was suspected in Case 2. In both cases, rib resection and diaphragmatic incision were performed. In Case 2, we encountered an intraoperative pleural injury, which could have easily caused hemothorax due to negative pressure in the thoracic cavity during expiration, leading to bleeding from the invaded tissue into the thoracic cavity. Intraoperatively, positive pressure ventilation with artificial respiration may act as tamponade and mask excessive bleeding. Considering these facts, it is necessary to check for bleeding even when negative pressure is applied before the wound is closed.
In any case, it is crucial to perform patronizing deployment maneuvers to avoid intraoperative pleural and vascular injuries, to carefully hemostat soft tissue and osteotomy sites, and to perform proper post-operative chest imaging evaluation to avoid delay in diagnosis in cases of hemopneumothorax.
We experienced two patients who required thoracotomy hematoma removal after anterior spinal surgery. Intraoperative patronage and adequate hemostasis are necessary to avoid post-operative complications such as hemothorax and hemopneumothorax.
Anterior reconstructive kyphorectomy surgery is considered in cases of severe kyphoscoliosis. Such procedures require treatment of thoracoabdominal organs. This may cause intraoperative complications such as massive bleeding. Intraoperative patronage and adequate hemostasis are necessary to avoid post-operative complications.
References
- 1.Ikard RW. Methods and complications of anterior exposure of the thoracic and lumbar spine. Arch Surg 2006;141:1025-34. [Google Scholar | PubMed]
- 2.Ayhan S, Nelson C, Gok B, Petteys RJ, Wolinsky JP, Witham TF, et al. Transthoracic surgical treatment for centrally located thoracic disc herniations presenting with myelopathy: A 5-year institutional experience. J Spinal Disord Tech 2010;23:79-88. [Google Scholar | PubMed]
- 3.Quraishi NA, Khurana A, Tsegaye MM, Boszczyk BM, Mehdian SM. Calcified giant thoracic disc herniations: Considerations and treatment strategies. Eur Spine J 2014;23(suppl 1):S76-83. [Google Scholar | PubMed]
- 4.Burrington JD, Brown C, Wayne ER, Odom J. Anterior approach to the thoracolumbar spine: Technical considerations. Arch Surg 1976;111:456-63. [Google Scholar | PubMed]
- 5.Coe JD, Arlet V, Donaldson W, Berven S, Hanson DS, Mudiyam R, et al. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine (Phila Pa 1976) 2006;31:345-9. [Google Scholar | PubMed]
- 6.Memtsoudis SG, Vougioukas VI, Ma Y, Gaber-Baylis LK, Girardi FP. Perioperative morbidity and mortality after anterior, posterior and anterior/posterior spine fusion surgery. Spine 2011;36:1867-77. [Google Scholar | PubMed]
- 7.Shapiro G, Green DW, Fatica NS, Boachie-Adjei O. Medical complications in scoliosis surgery. Curr Opin Pediatr 2001;13:36-41. [Google Scholar | PubMed]
- 8.Geervliet PC, van Royen BJ, Vonk Noordegraaf A, Kranendonk SE, David EF, Paul MA. Late spontaneous hemothorax complicating anterior spinal instrumentation in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2007;32:E730-3. [Google Scholar | PubMed]
- 9.Anderson TM, Mansour KA, Miller JI. Thoracic approaches to anterior spinal operations: Anterior thoracic approaches. Ann Thorac Surg 1993;55:1447-52; discussion 1451-2. [Google Scholar | PubMed]
- 10.Naunheim KS, Barnett MG, Crandall DG, Vaca KJ, Burkus JK. Anterior exposure of the thoracic spine. Ann Thorac Surg 1994;57:1436-9. [Google Scholar | PubMed]
- 11.Dwyer AF, Schafer MF. Anterior approach to scolosis. J Bone Joint Surg Br 1974;56:218-24. [Google Scholar | PubMed]
- 12.Gabel BC, Schnell EC, Dettori JR, Jeyamohan S, Oskouian R. Pulmonary complications following thoracic spinal surgery: A systematic review. Global Spine J 2016;6:296-303. [Google Scholar | PubMed]
- 13.Rentenberger C, Shue J, Soffin EM, Stiles BM, Craig CM, Hughes AP. Intercostal artery hemorrhage with hemothorax following combined lateral and posterior lumbar interbody fusion: A case report. Spinal Cord Ser Cases 2019;5:60. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review
April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review May 10, 2024 Myelopathy Associated with Rapid Progression of a Dystrophic Neurofibromatosis-1 Curve – A Case Report and Review of Literature
May 10, 2024 Myelopathy Associated with Rapid Progression of a Dystrophic Neurofibromatosis-1 Curve – A Case Report and Review of Literature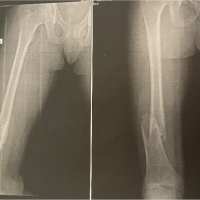 January 10, 2024 An Uncommon Presentation of Osteosarcoma in a Child: A Case Report
January 10, 2024 An Uncommon Presentation of Osteosarcoma in a Child: A Case Report December 10, 2023 Effects of the Percutaneous Carbon Dioxide Therapy on Post-surgical and Post-traumatic Hematoma, Edema and Pain
December 10, 2023 Effects of the Percutaneous Carbon Dioxide Therapy on Post-surgical and Post-traumatic Hematoma, Edema and Pain