
Clinicians should be aware of this condition as it mimics the signs of an infection, but has a very different treatment course.
Dr. John Christian Parsaoran Butarbutar, Department of Orthopaedic and Traumatology, Faculty of Medicine, Universitas Pelita Harapan, Siloam Hospital Lippo Village, Tangerang, Indonesia. E-mail: john.butarbutar@lecturer.uph.edu
Abstract
Introduction: Calcification in the tendon (Calcific Tendinitis) occurs commonly in the shoulder, but this condition can happen in other tendon sites. Calcific tendinitis of the hand and wrist occurs rarely, which causes unfamiliarity toward the disease. With the symptoms mimicking other causes, misdiagnosis often happens. This can cause ineffective and over treatment.
Case Report: A 51-year-old man presented with a 2-week-pain on his right wrist with localized erythema and tenderness on physical examination. Imaging with ultrasound and X-ray shows calcification on the flexor carpi ulnaris tendon. Patient was treated with splinting for 2 weeks and NSAID for pain management and was free of pain afterwards.
Conclusion: Calcific tendinitis mimics the symptoms of various causes. The ability to differentiate this entity to other differential diagnosis leads to an effective and precise treatment.
Keywords: Calcified tendinitis, hand and wrist, wrist pain, calcification
Calcification of the tendon most commonly occurs in the shoulder, causing rotator cuff pain, but calcification can also be found on other tendon sites such as hip, spine, patella, and Achilles [1]. Calcific tendinitis of the hand and wrist are extremely rare, occurring only 2.4% of calcification deposits in the tendon [2]. The most commonly affected tendon of the hand and wrist is the flexor carpi ulnaris (FCU) tendon, usually at the insertion near the pisiform bone [1]. Due to its rarity, calcific tendinosis of the wrist is often misdiagnosed, most times confused with acute infection, tenosynovitis, and other inflammatory related diseases because of the same clinical manifestation. This leads to overtreatment with antibiotics and to some extent, unnecessary surgeries.
We present a case of a 51-year-old male, presented with pain over the right wrist especially on the ulnar side for approximately 2 weeks before visit. The pain was described as pulsating pain, increased with wrist movement. The patient is right-handed and has a hobby playing table tennis. The patient also denied history of trauma, comorbidities such as diabetes or hypothyroid and denied taking any routine medication.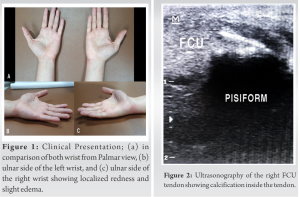
Physical examination showed erythema and edema on the volar on the ulnar side of the right wrist with tenderness specifically on the FCU tendon near the pisiform (Fig. 1, 2, 3). Right wrist movement range of motion was full with mild discomfort. Wrist Press test, Grind Test, Ballottement test, and Phalen and Tinel Test were done and showed negative results (Fig. 1). Ultrasound was performed and the results showed calcium deposit at the FCU tendon above the pisiform bone. No nerve median nerve entrapment was found, and other structures showed unremarkable results. To confirm the diagnosis, the patient was sent to do a wrist X-ray (AP, Lateral and Oblique) and the result supports the diagnosis of calcified tendinitis of the FCU tendon (Fig. 2, 3). The patient underwent wrist splinting in a 10 degrees extension position and was advised to use his left hand for daily activities and let his right-hand rest. Follow-up was done a month post splinting and the pain was relieved after 2 weeks of splinting. The splint was removed independently. The patient complained of mild wrist stiffness and is then fully relieved after few days (Fig. 4).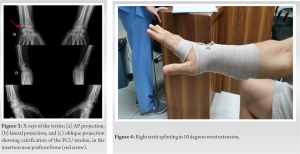
Calcific Tendinitis of the hand and wrist is a rare entity. According to a systematic review by Draghi et al. that highlights locations of calcific tendinitis aside from the shoulder region, there were only 13 and 7 cases of hand and wrist calcific tendinitis reported, respectively, out of 184 cases reviewed [3]. Calcific tendinitis of the hand and wrist slightly affects women more than man. This condition is commonly found within the age of 30–60, with mean age of 45 years, but no age is spared as it can be found in children with an age as early as 9 years old [4,5,6]. FCU tendon is the most commonly affected tendon of the hand and wrist, usually at the insertion site near the pisiform bone [7].
The cause and the process of calcium deposits in the tendon are still poorly understood. There are two most widely accepted etiology theory which are degenerative process of the tendon and the inability to for tissue reparation post trauma and reactive calcification, a cell mediated process accompanied by fibrocartilaginous metaplasia of the tendinous tissue [8,9]. Other theories stated the etiology of the disease involving injury, tissue hypoxia, and failed healing response. The damaged tendon usually began healing process and remodeling, but in case of calcific tendinosis, there’s disturbance at stages of healing process that leads to abnormal healing pathway. These disturbances can be cause by multiple factors such as comorbidities or drug consumption [10]. Uhthoff et al. proposes theory regarding the pathogenesis of calcific tendinosis which consists of three stages. First is the Precalcific stage, where the tendon, undergoes fibrocartilaginous transformation which is a metaplasia process. Then, it continues to the calcific stage where pain usually starts to erupts, which can be divided into three phases, the formative, resting, and resorptive phase. The formative phase is when the calcium crystal is being deposited in matrix vesicles that largens and form a foci with fibrocartilaginous septa. This septa then gradually erodes whilst the deposit grows larger. The resting phase is when the foci of calcification are bordered by fibrocollagenous tissue, in which this terminates the deposition of calcium. Then this continues to the resorptive phase, the calcium deposit is then being resorbed, after being phagocyted by macrophage and multinucleated giant cells. After this, the process continues to the next stage, which is the post calcific stage which is the remodeling of the tendon [9]. Like most calcification in the tendon, patient usually comes complaining of an acute or subacute pain. Contrary to calcified tendons of the shoulder, calcific tendinosis of the hand and wrist are always symptomatic [2,5]. Pain can vary from moderate to disabling pain, this is due to different pain tolerance and different stage of calcification when the patient presents to the hospital [9]. Pain usually is localized to a single area, accompanied with localized erythema, swelling, warmth, and severe tenderness, indicating an inflammation process, which can cause confusion to infection cause [7,11]. Commonly, patient is afebrile, although some reported experiencing mild fever [4,7]. Determining the most severe point of tenderness can be helpful in determining the suspected location of calcium deposit, therefore helps in determining which imaging should be obtained to view the calcification [5,7]. Range of motion may be decreased secondary to pain, and when it affects the FCU, movement of flexing the wrist and ulnar deviation worsens the pain. History of trauma only presents in one third of patient according to a study conducted by Carol et al., and repetitive movement of the wrist causing strain of the tendons such as such as sports involving the use of rackets such as tennis, badminton, and golf can contribute to formation of calcium deposit [5,12]. Most calcific tendinosis of the wrist affects the dominant hand. Most of these symptoms are found in our patient, with no history of significant trauma and a hobby that requires wrist movements. Systemic symptoms were not found in our patient thus we deprioritized the possibility of an infection source. Plain radiographs had been widely used to diagnose calcific tendinitis. Appearance of the calcification on radiographs depends on the phase of tendinitis. Acute condition of calcific tendinitis shows a fluffy, ill-defined and inhomogeneous appearance, whereas a better defined, and homogenous calcification are usually seen in a more chronic condition [1]. Measurement of calcification usually ranges between 2 and 10 mm. Initially, a minimal of two orthogonal views of radiographs is obtained, but additional view can be obtained accordingly [13]. Selecting the projections of the radiographs can be helped by determining the suspected location of calcification by finding the most severe point of tenderness on physical examination [5]. Calcification of the FCU was visualized from the AP X-Ray projection in our patient, which help us further determine the cause of the symptoms are due to calcified tendinitis. Ultrasonography can be one of the greatest utilities in evaluating disorders of the hand and wrist that affects the tendons, nerves, ligaments etc. Although it is operator dependent, it’s proven that ultrasound is very useful in identifying the location of calcification in cases of calcific tendinitis, usually by determining using probe tenderness. It also helps in giving information on the nature of the calcification, whether it’s hard or soft. Doppler utility can also determine whether the calcification is in the acute or chronic phase [14]. With dynamic ultrasonography available in our outpatient clinic, we found calcification on the FCU tendon before confirming with X-ray. These imaging results confirmed the diagnosis of calcified tendinitis of the FCU tendon. Calcific tendinitis of the hand wrist may resolve on its own without any treatment, with an average of 20 days for the symptoms to be relieved [5]. Treatments are usually conservative and surgical intervention is rarely needed and is reserved only for patients with persistent or recurrent calcification, where conservative treatment no longer offered resolution and has been shown to disturb the patient’s daily activities [6,7,11]. Injection using local anesthetics, with or without corticosteroid has shown to be effective, with the complete resolution within 6 days [5]. A series done by Ahuja et al., has shown that ultrasound guided barbotage, has been shown to be effective with immediate improvement of symptoms [14]. Splinting has also shown to be effective as it shortens the span of pain to 12 days, and it is what was done to our patient and has shown good result [15].
The presentation of calcific tendinosis of the hand and wrist mimics the presentation of an infection, with pain and tenderness with localized erythema, and this may lead to most physician treat it with unnecessary antibiotics [4,11,13]. Familiarizing yourself with this condition helps in making a correct diagnosis thus establishing an effective and efficient treatment course.
Clinician should be aware of this condition as it mimics the signs of an infection, but has a very different treatment course.
References
- 1.Beckmann NM. Calcium apatite deposition disease: Diagnosis and treatment. Radiol Res Pract 2016;2016:4801474. [Google Scholar | PubMed]
- 2.Selby CL. Acute calcific tendinitis of the hand: An infrequently recognized and frequently misdiagnosed form of periarthritis. Arthritis Rheum 1984;27:337-40. [Google Scholar | PubMed]
- 3.Selby CL. Acute calcific tendinitis of the hand: An infrequently recognized and frequently misdiagnosed form of periarthritis. Arthritis Rheum 1984;27:337-40. [Google Scholar | PubMed]
- 4.Walocko FM, Sando IC, Haase SC, Kozlow JH. Acute calcific tendinitis of the index finger in a child. Hand (N Y) 2017;12:NP84-7. [Google Scholar | PubMed]
- 5.Carroll RE, Sinton W, Garcia A. Calcium deposits in the hand. J Am Med Assoc 1955;157:422-6. [Google Scholar | PubMed]
- 6.Kim JK, Park ES. Acute calcium deposits in the hand and wrist; Comparison of acute calcium peritendinitis and acute calcium periarthritis. J Hand Surg Eur Vol 2014;39:436-9. [Google Scholar | PubMed]
- 7.Nikci V, Doumas C. Calcium deposits in the hand and wrist. J Am Acad Orthop Surg 2015;23:87-94. [Google Scholar | PubMed]
- 8.Refior HJ, Krödel A, Melzer C. Examinations of the pathology of the rotator cuff. Arch Orthop Trauma Surg 1987;106:301-8. [Google Scholar | PubMed]
- 9.Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: Pathogenesis, diagnosis, and management. J Am Acad Orthop Surg 1997;5:183-91. [Google Scholar | PubMed]
- 10.Oliva F, Via AG, Maffulli N. Physiopathology of intratendinous calcific deposition. BMC Med 2012;10:95. [Google Scholar | PubMed]
- 11.Lee HO, Lee YH, Mun SH, Kang UR, Lee CK, Suh KJ. Calcific tendinitis of the hand and foot: A report of four cases. J Korean Soc Magn Reson Med 2012;16:177-83. [Google Scholar | PubMed]
- 12.Blum AG, Zabel JP, Kohlman R, Batch T, Barbara K, Zhu X, et al. Pathologic conditions of the hypothenar eminence: Evaluation with multidetector CT and MR imaging. Radiographics 2006;26:1021-45. [Google Scholar | PubMed]
- 13.Doumas C, Vazirani RM, Clifford PD, Owens P. Acute calcific periarthritis of the hand and wrist: A series and review of the literature. Emerg Radiol 2007;14:199-203. [Google Scholar | PubMed]
- 14.Ahuja A, Lawande M, Daftary AR. Role of radiographs and ultrasound in diagnosing calcific tendinitis and periarthritis in the wrist and hand with ultrasound-guided barbotage as management tool. Indian J Radiol Imaging 2021;31:605-10. [Google Scholar | PubMed]
- 15.Dilley DF, Tonkin MA. Acute calcific tendinitis in the hand and wrist. J Hand Surg Br 1991;16:215-6. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Kienbock’s Disease in a Young Female without Classical Risk Factors: A Case Report with 1-year Functional Outcome Following Proximal Row Carpectomy
June 1, 2026 Kienbock’s Disease in a Young Female without Classical Risk Factors: A Case Report with 1-year Functional Outcome Following Proximal Row Carpectomy July 8, 2017 Aspergillus Osteomyelitis of the Ribs in Immunocompetent Hosts: Report of Two Rare Cases
July 8, 2017 Aspergillus Osteomyelitis of the Ribs in Immunocompetent Hosts: Report of Two Rare Cases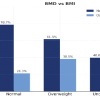 February 1, 2026 Assessment of Bone Mineral Density and Its Correlation with Body Mass Index and Stress Fractures among Paramilitary Recruits
February 1, 2026 Assessment of Bone Mineral Density and Its Correlation with Body Mass Index and Stress Fractures among Paramilitary Recruits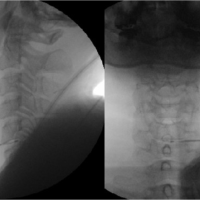 January 10, 2024 Use of Navigable Ablation Decompression Treatment (L-DISQ) for Contained Cervical Disc Herniation – Technical Note and Literature Review
January 10, 2024 Use of Navigable Ablation Decompression Treatment (L-DISQ) for Contained Cervical Disc Herniation – Technical Note and Literature Review